Answers
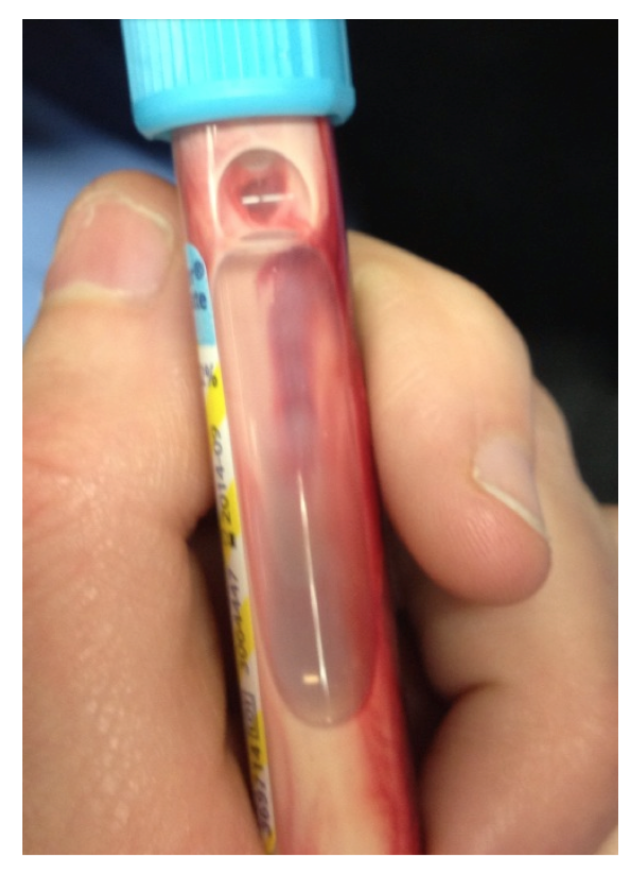
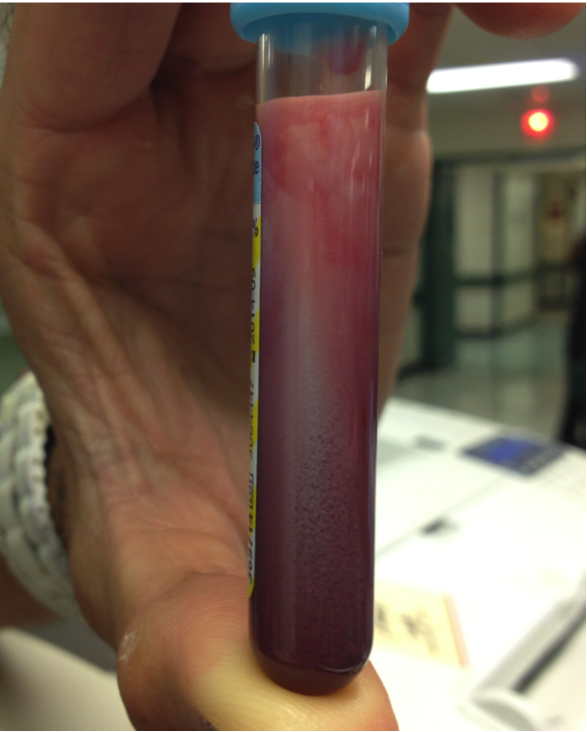
- Lipemic Serum
- Hypertriglyceridemia-induced acute pancreatitis (HTGP)
Discussion
Hypertriglyceridemia (HTG) is an uncommon cause of acute pancreatitis (AP). The greatest risk for hypertriglyceridemia-induced acute pancreatitis (HTGP) occurs with triglyceride levels above 1000 mg/dL or 10 mmol/L; however, pancreatitis can occur at lower levels. (1,2) HTGP often causes a more severe clinical course, when compared to other etiologies of AP. (3) Serum triglycerides are nontoxic, but their metabolites lead to a profound inflammatory response. (4)
HTGP presents with abdominal pain, nausea, and vomiting; unique are xanthomas, hepatosplenomegaly, or lipemia retinalis (creamy white appearance to the retinal arteries and veins). Treatment includes conventional management of AP (bowel rest, hydration, pain medication) as well as decreasing serum triglyceride levels with options of apheresis, insulin or heparin. (5-7) While total plasma exchange apheresis has been shown to be effective, no evidence is available comparing it to insulin or heparin therapies. Patients should be started on oral antihyperlipidemic therapy as well to help further prevent pancreatic organ failure or necrosis. (8,9)
Our patient had a computed tomography of the abdomen and pelvis that showed acute pancreatitis congruent with the grossly lipemic samples. The labs revealed a triglyceride level of 17,155mg/dL, lipase 208U/L, glucose 280mg/dL and hemogobin A1C 7.0%. The hyponatremia found on labs is secondary to the HTG and is not physiologically significant. (10) While admitted, he received apheresis, oral gemfibrozil and insulin for goal triglyceride level of <1000mg/dL.
Pearls
- Consider alternate etiologies for pancreatitis, such as triglyceridemia, diuretics or ischemia.
- HTGP requires adjunctive treatment to reduce triglycerides.
References
- Tsuang, W., Navaneethan, U., Ruiz, L., Palascak, J. B. & Gelrud, A. Hypertriglyceridemic pancreatitis: presentation and management. Am. J. Gastroenterol. 104, 984–991 (2009).
- Durrington, P. Dyslipidaemia. The Lancet 362, 717–731 (2003).
- Kyriakidis, A. V. et al. Plasmapheresis in the management of acute severe hyperlipidemic pancreatitis: report of 5 cases. Pancreatol. Off. J. Int. Assoc. Pancreatol. IAP Al 5, 201–204 (2005).
- Baranyai, T., Terzin, V., Vajda, A., Wittmann, T. & Czakó, L. [Acute pancreatitis caused by hypertriglyceridemia]. Orv. Hetil. 151, 1869–1874 (2010).
- Aryal, MR.Acute pancreatitis owing to very high triglyceride levels treated with insulin and heparin infusion. BMJ Case Rep. 2013 Apr 22;2013
- Ewald, N. & Kloer, H.-U. Treatment options for severe hypertriglyceridemia (SHTG): the role of apheresis. Clin. Res. Cardiol. Suppl. 7, 31–35 (2012).
- Milionis, H. The hyponatremic patient: a systematic approach to laboratory diagnosis. CMAJ. 2002. April 16: 166 (8)
- Iskandar, S. B. & Olive, K. E. Plasmapheresis as an adjuvant therapy for hypertriglyceridemia-induced pancreatitis. Am. J. Med. Sci. 328, 290–294 (2004).
- Syed, H., Bilusic, M., Rhondla, C. & Tavaria, A. Plasmapheresis in the treatment of hypertriglyceridemia-induced pancreatitis: A community hospital’s experience. J. Clin. Apheresis 25, 229–234 (2010).
- Lloret Linares, Célia MD. Acute Pancreatitis in a Cohort of 129 Patients Referred for Severe Hypertriglyceridemia. Pancreas: July 2008






2 thoughts on “"Rule out SBO"”
Great case