Authors: Cameron Upchurch, MD (EM and Critical Care Attending, University of Vermont Larner College of Medicine); Talat Raja, MD (Pulmonary and Critical Care Fellow, University of Vermont Medical Center); Isaac Sellinger, MS 3 (University of Vermont Larner College of Medicine); Skyler Lentz, MD (@SkylerLentz, EM and Critical Care Attending, University of Vermont Larner College of Medicine) // Reviewed by: Alex Koyfman, MD (@EMHighAK) and Brit Long, MD (@long_brit)
Case
A 45-year-old man with a past medical history of diabetes, hypertension, and known multivessel coronary artery disease (CAD) presents to the emergency department (ED) with substernal chest pain and diaphoresis. He is ill appearing, tachycardic, has a blood pressure of 88/60 mm Hg, cool extremities, and a lactic acidosis. Electrocardiogram shows > 1 mm ST segment elevation in inferior leads. The catheterization lab is activated and cardiology is paged who plans for emergent cardiac catheterization and requests placement of an arterial line for hemodynamic monitoring while they are preparing the catheterization lab. As the emergency medicine (EM) resident prepares for arterial line placement and instinctively targets the forearm radial artery (fRA), chart review indicates that the patient has been evaluated for planned coronary artery bypass graft (CABG) recently, and the radial artery was considered as a potential option for graft harvest. The team pauses to discuss alternative arterial cannulation sites that would not compromise the integrity of a potential graft-harvesting site for future CABG.
Background
Arterial lines may be placed for invasive, beat-to-beat measurement of the blood pressure in critically ill patients. A single center ED resuscitation unit-based study showed a clinically significant difference in blood pressure (≥ 10 mmHg difference in mean arterial pressure that would change management) between an invasive arterial measurement and non-invasive blood pressure cuff in 16% of patients on vasopressors with septic shock.1 Arterial lines have been shown to be safe with a major complication rate of < 1%.2 The most common site for placement is the forearm radial artery (fRA), traditionally placed in the radial artery in the forearm near the wrist because of its safety and accessibility.2 The distal radial artery (dRA) over the dorsal hand in the region of the anatomical snuffbox is an appealing option that has not been described in the EM literature.
What is a distal radial arterial line?
The brachial artery bifurcates into the radial and ulnar arteries. The radial artery continues down the lateral forearm toward the wrist where it is anterior to the radius bone—often the site for traditional radial arterial line placement (we term, the forearm radial artery [fRA]). From here the radial artery continues distally and gives branch to the superficial palmar branch artery which eventually joins the ulnar artery completing the superficial palmar arch system to perfuse the hand. After this branch, the radial artery continues distally and under the extensor pollicis brevis tendon into the anatomical snuffbox between the extensor pollicis brevis and longus tendons and superficial to the scaphoid and trapezium bones.3 The radial artery in this location within the anatomical snuffbox we term the distal radial artery (dRA). The dRA continues distally under the extensor pollicis longus tendon and gives branch to the princeps pollicis artery that perfuses the thumb (Figure 1).4
Figure 1. Anatomy of forearm arteries. The ideal location for cannulation of the distal radial artery (dRA) for an arterial line is after the take-off of the superficial palmar artery branch from the proximal forearm radial artery but proximal to the take-offs of the princeps pollicis artery and the deep palmar branch. dRA; distal radial artery; PPA, princeps pollicis artery; SPB, superficial palmar branch; DPB, deep palmar branch.

A dRA line is percutaneous vascular access of the radial artery at the dorsum of the hand in this region of the anatomical snuffbox. Applications and indications are similar to traditional fRA arterial lines including percutaneous coronary intervention, interventional radiology and neuroradiology procedures, as well as placement of indwelling catheters for invasive continuous blood pressure monitoring.
Why distal radial arterial lines?
The dRA site may be more ideal than the traditional fRA site for several reasons. An arterial line at the dRA allows the patient to flex/extend their wrist more freely, and may be more comfortable as compared to the fRA site. The dRA site may be more accommodating for a patient that requires wrist restraints despite verbal and/or medication de-escalation and management. Additionally, some patients simply may not have anatomy conducive to placement of an arterial line in the traditional fRA site (e.g., wrist/arm contractures or inability to extend the wrist). Furthermore, the dRA offers an alternative invasive blood pressure monitoring site for patients who may not have a traditional fRA site available for access (e.g., already occluded, surgically absent, vasospasm/hematoma due to previous puncture attempts). Lastly, the dRA site keeps the fRA site free of punctures, catheters, and potential damage. This, coupled with the ability to have antegrade perfusion maintained through the proximal fRA and superficial palmar arch to the hand has been associated with lower rates of proximal radial artery occlusion, which can be as high as >30% in cases of fRA access use.5–11 This may allow the fRA to be potentially used in the future for important interventions such as endovascular interventional procedures, harvesting for CABG, or arterio-venous (AV) fistula creation for dialysis access.12
The majority of data on the use of the dRA for arterial access comes from the interventional cardiology, radiology, and neurology literature where the dRA is often used as arterial access for a variety of reasons. In addition to being associated with less radial artery occlusion, in this population the use of the dRA as compared to the fRA for arterial access is associated with less bleeding and hematoma formation, and shorter times to hemostasis—likely due to the more compressible site of the dRA over the scaphoid and lower likelihood for hematoma to track up the forearm.7–10,13,14 The use of the dRA site has been associated in some studies with lower first-attempt success and increased time-to-successful cannulation as compared to the fRA site.5,8,9,13 We believe this is likely due to decreased familiarity with a new anatomical location, and like many procedures, success rates improve over time with increased practice and with the use of ultrasound.14–20 In our health system, residents, fellows, and attendings routinely successfully place dRA arterial lines on critically ill patients in the ED, ICU, and even critical access hospital settings.
In the ICU setting, several non-inferiority randomized controlled trials have demonstrated no difference in success rates in dRA as compared to fRA access for arterial lines with overall success rates >95%.21–23 Available data on the use of dRA arterial lines in the ICU for invasive blood pressure monitoring suggest the dRA site is feasible, safe, with potentially lower complications and less frequent loss of arterial pressure waveforms or inadvertent line dislodgement.19–21,23–25 However, to date there exists a paucity of published data on the use of dRA arterial lines in the ED.
How to perform a distal radial arterial line
The procedure for placing a dRA line is similar to the placement of an arterial line in the traditional fRA site (see emDocs post “Unlocking Common ED Procedures: arterial lines”), except the cannulation site instead is in the dRA in the anatomical snuffbox.
Prepare necessary materials including: needle and syringe for drawing up and injecting local anesthetic (such as 1% lidocaine), arterial catheter access kit with guidewire, linear ultrasound probe with sterile cover, sterile gloves and mask/cap, sterile drape/towel, antiseptic prep, non-absorbable suture with needle driver and scalpel for securing the line or other catheter securement device, sterile dressing, and arterial pressure transducer line set-up.
The patient’s arm is positioned in a “holding a wine glass” position with the wrist extended to align the first metacarpal parallel with the radius and the hand with ulnar deviation to flatten the anatomical snuffbox area and bring the dRA more superficial for ease of access (Figure 2). The hand can be taped in this position if needed and a small towel roll can be used for the patient to grasp in their hand to aid in achieving the appropriate position described.
Figure 2. Hand positioning for placement of a distal radial arterial line. A. “Holding a wine glass” position. B. Utilizing a small towel roll for the hand to grasp for optimal positioning for distal radial arterial line placement.

Consent is obtained. A time out is completed. Then prepare the area with antiseptic and drape sterile. Don sterile gloves, place sterile probe cover over the linear ultrasound probe, and scan the anatomical snuffbox to locate the dRA (Figure 3).
Figure 3. Ultrasound placement for dynamic ultrasound-guided distal radial arterial line placement.

Under dynamic ultrasound-guidance, anesthetize the skin and subcutaneous tissue with local anesthetic over and around the dRA taking care to ensure there is no intravascular delivery. Under dynamic ultrasound-guidance access the dRA with the needle into the middle of the lumen and thread the guidewire ensuring there is no significant resistance to ensure intra-luminal placement, then utilizing Seldinger technique advance the arterial line catheter over the wire (Figure 4).
Figure 4. Ultrasound images of distal radial artery in the anatomical snuffbox region. A. Non-compressed ultrasound image. B. Compressed ultrasound image compressing adjacent veins. CV: cephalic vein; RV, radial vein; dRA, distal radial artery; SB, scaphoid bone.

Connect the pressure transducer to the arterial line and confirm appropriate arterial waveform pressure (Figure 5). Secure the arterial catheter with suture and place sterile dressing.
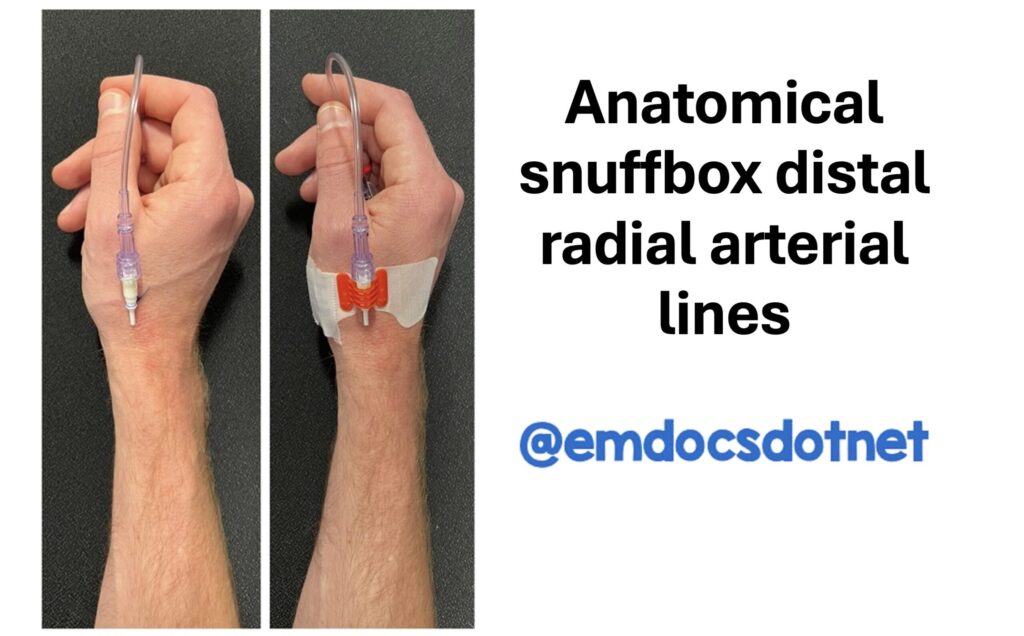
Figure 5. Example of distal radial arterial line post-placement using a standard 20 Gauge 4.45 cm arterial catheter. A. Placement of distal radial arterial line secured with suture. B. Placement of distal radial arterial line with securement device.

Potential pitfalls
Pitfalls of dRA line placement are similar to traditional fRA placement such as inability to successfully cannulate the vessel, bleeding, pain, hematoma, dissection, pseudoaneurysm formation, air embolism, infection, or damage to nearby structures.2 Considerations unique to the dRA site include avoiding the cephalic vein that is often superficial to the dRA in this site, as well as the radial veins that often accompany the dRA on each side in addition to the superficial radial nerves in the area.
Additionally, care should be taken to avoid the extensor pollicis longus and brevis tendons that border each side of the dRA. The dRA is often slightly smaller diameter than the fRA, but most often is able to accept similar sized arterial catheters (e.g., 20 gauge often used in the ED/ICU or often even 5-6 Fr sheaths used in interventional procedures in the catheterization laboratory) as the fRA.23 The use of ultrasound can help mitigate all of these risks.14,26 Importantly, we recommend cannulating the dRA in the anatomical snuffbox area rather than through the first dorsal interosseous muscle even more distally in the dorsal hand after the dRA dives under the extensor pollicis longus tendon. In this more distal dorsal hand location, the catheter is more likely to fail given its course through the muscle, and this more distal location encroaches upon the take-off of the princeps pollicis artery that supplies the thumb. Instead, cannulating the dRA in the anatomical snuffbox is proximal to this location thereby avoiding the princeps pollicis artery branch and deep palmar artery branch.
Case Review
The EM resident successfully places a left dRA arterial line under ultrasound-guidance on first attempt without complication. The patient goes emergently to the catheterization laboratory. He became more hypotensive during the procedure requiring norepinephrine infusion and was found to have cardiogenic shock on right heart catheterization during the procedure. He underwent a microaxial flow pump (e.g., Impella®)-assisted percutaneous coronary intervention to the culprit right coronary artery that was 95% occluded. During the left heart catheterization, he was found to have severe multivessel CAD. He was admitted to the ICU and recovered. Once stabilized, he was taken for three-vessel CABG for his remaining severe CAD and the cardiac surgeon harvested the left proximal radial artery for one of his coronary bypass grafts after it was deemed suitable.
Pearls and Pitfalls
-The dRA in the anatomical snuffbox is a suitable alternative site for arterial catheter placement for invasive blood pressure monitoring
-The dRA site may be more comfortable for patients, associated with less complications, and is associated with less radial artery occlusion as compared to the traditional fRA site
-The use of the dRA site spares the fRA site for future potential needed interventions such as interventional cardiology/radiology procedures or future use of the fRA for CABG grafts, AV fistula creation, or flaps
-dRA line allows continuous antegrade perfusion of the hand from the fRA and superficial/deep palmar arches and therefore may be lower risk for hand malperfusion
Further Reading:
- Tran QK, Gelmann D, Alam Z, et al. Discrepancy Between Invasive and Noninvasive Blood Pressure Measurements in Patients with Sepsis by Vasopressor Status. West J Emerg Med. 2022;23(3):358-367. doi:10.5811/westjem.2022.1.53211
- Scheer BV, Perel A, Pfeiffer UJ. Clinical review: Complications and risk factors of peripheral arterial catheters used for haemodynamic monitoring in anaesthesia and intensive care medicine. Crit Care. 2002;6(3):199-204. doi:10.1186/cc1489
- Cerda A, Del Sol M. Anatomical Snuffbox and it Clinical Significance: A Literature Review. Int J Morphol. 2015;33(4):1355-1360. doi:10.4067/S0717-95022015000400027
- Narsinh KH, Mirza MH, Duvvuri M, et al. Radial artery access anatomy: considerations for neuroendovascular procedures. J NeuroIntervent Surg. 2021;13(12):1139-1144. doi:10.1136/neurintsurg-2021-017871
- Zahedmehr A, Dousti A, Alemzadeh-Ansari MJ, et al. Comparison of radial artery occlusion between traditional radial access and distal radial access for coronary angiography and intervention: A prospective cohort study. Heliyon. 2024;10(20):e39451. doi:10.1016/j.heliyon.2024.e39451
- Eid-Lidt G, Rivera Rodríguez A, Jimenez Castellanos J, Farjat Pasos JI, Estrada López KE, Gaspar J. Distal Radial Artery Approach to Prevent Radial Artery Occlusion Trial. JACC: Cardiovascular Interventions. 2021;14(4):378-385. doi:10.1016/j.jcin.2020.10.013
- Babunashvili AM, Pancholy S, Zulkarnaev AB, et al. Traditional Versus Distal Radial Access for Coronary Diagnostic and Revascularization Procedures: Final Results of the TENDERA Multicenter, Randomized Controlled Study. Catheter Cardiovasc Interv. 2024;104(7):1396-1405. doi:10.1002/ccd.31271
- Feghaly J, Chen K, Blanco A, Pineda AM. Distal versus conventional radial artery access for coronary catheterization: A systematic review and meta-analysis. Catheterization and Cardiovascular Interventions. 2023;101(4):722-736. doi:10.1002/ccd.30602
- Rehman MEU, Raja HAA, Osama M, et al. Efficacy and Safety of Distal Radial Artery Access versus Proximal Radial Artery Access for Cardiac Procedures: A Systematic Review and Meta-Analysis. Med Princ Pract. 2025;34(4):328-337. doi:10.1159/000543817
- Mufarrih SH, Haider S, Qureshi NQ, et al. Distal Versus Proximal Radial Arterial Access for Percutaneous Coronary Angiography and Intervention: Updated Meta-Analysis of Randomized Controlled Trials. The American Journal of Cardiology. 2024;218:34-42. doi:10.1016/j.amjcard.2024.02.032
- Rashid M, Kwok CS, Pancholy S, et al. Radial Artery Occlusion After Transradial Interventions: A Systematic Review and Meta-Analysis. J Am Heart Assoc. 2016;5(1):e002686. doi:10.1161/JAHA.115.002686
- Tehrani BN, Sherwood MW, Damluji AA, et al. A Randomized Comparison of Radial Artery Intimal Hyperplasia Following Distal Versus Proximal Transradial Access for Coronary Angiography: PRESERVE RADIAL. Journal of the American Heart Association. 2024;13(4):e031504. doi:10.1161/JAHA.123.031504
- Tsigkas G, Papageorgiou A, Moulias A, et al. Distal or Traditional Transradial Access Site for Coronary Procedures: A Single-Center, Randomized Study. JACC: Cardiovascular Interventions. 2022;15(1):22-32. doi:10.1016/j.jcin.2021.09.037
- Hadjivassiliou A, Kiemeneij F, Nathan S, Klass D. Ultrasound-guided access to the distal radial artery at the anatomical snuffbox for catheter-based vascular interventions: a technical guide. doi:10.4244/EIJ-D-19-00555
- Cereda A, Allievi L, Busetti L, et al. Nurse-led distal radial access: efficacy, learning curve, and perspectives of an increasingly popular access. Does learning by doing apply to both the doctor and the nurse? Minerva Cardiol Angiol. 2023;71(1):35-43. doi:10.23736/S2724-5683.22.05843-4
- Mori S, Hirano K, Yamawaki M, et al. A Comparative Analysis between Ultrasound-Guided and Conventional Distal Transradial Access for Coronary Angiography and Intervention. J Interv Cardiol. 2020;2020:7342732. doi:10.1155/2020/7342732
- Saunders SL, Casinader SJ, Fernandez RS, et al. “Distal radial first”: feasibility and safety for coronary angiography and PCI in Australia. AsiaIntervention. 2025;11(1):35-43. doi:10.4244/AIJ-D-24-00036
- Roh JW, Kim Y, Lee OH, et al. The learning curve of the distal radial access for coronary intervention. Sci Rep. 2021;11:13217. doi:10.1038/s41598-021-92742-7
- Wang J, Zhang J, Zhang Y, et al. Feasibility and safety analysis of distal radial arterial catheterization for arterial pressure monitoring in ICU. J Clin Monit Comput. 2025;39(4):767-774. doi:10.1007/s10877-025-01313-y
- Maruhashi T, Oi M, Hattori J, Asari Y. Distal radial approach for arterial pressure monitoring with a long catheter provides safe and stable monitoring in the intensive care unit: A single-center retrospective study. J Vasc Access. 2025;26(1):168-174. doi:10.1177/11297298231212393
- Cumitini L, Giubertoni A, Rossi L, Patti G. Distal Radial Artery Approach for Invasive Blood Pressure Monitoring in Intensive Cardiac Care Unit. The American Journal of Cardiology. 2025;248:16-22. doi:10.1016/j.amjcard.2025.04.005
- Xiong J, Hui K, Xu M, Zhou J, Zhang J, Duan M. Distal radial artery as an alternative approach to forearm radial artery for perioperative blood pressure monitoring: a randomized, controlled, noninferiority trial. BMC Anesthesiol. 2022;22(1):67. doi:10.1186/s12871-022-01609-5
- Peng C, Wu W, Zhang Y, et al. Distal versus conventional radial artery catheterization for hemodynamic monitoring in intensive care setting: a randomized, controlled, non-inferiority trial. BMC Anesthesiol. 2025;25(1):348. doi:10.1186/s12871-025-03228-2
- Oi M, Maruhashi T, Ishikura A, et al. Safety of arterial catheterization using the distal radial approach in intensive care unit management: A pilot study. J Vasc Access. 2022;23(4):538-542. doi:10.1177/11297298211003374
- Oi M, Maruhashi T, Kurihara Y, Asari Y. Evaluation of a new insertion site for arterial pressure line in intensive care unit management: a prospective study. J Clin Monit Comput. 2023;37(3):867-872. doi:10.1007/s10877-022-00957-4
- Gibbons RC, Zanaboni A, Saravitz SM, Costantino TG. Ultrasound Guidance Versus Landmark-Guided Palpation for Radial Arterial Line Placement by Novice Emergency Medicine Interns: A Randomized Controlled Trial. The Journal of Emergency Medicine. 2020;59(6):911-917. doi:10.1016/j.jemermed.2020.07.029





