
The Time-Sensitive Conundrum of Diagnosing Spinal Epidural Abscess in the ED
Stephen Alerhand, MD
Resident Physician
Icahn School of Medicine at Mount Sinai
Introduction
- Spinal epidural abscess is an extremely rare diagnosis but a potentially devastating one.
- It has proven to be a difficult ER diagnosis.
- Unfortunately, once the classic symptoms appear and a definitive diagnosis is made, the very symptoms we look for have often become irreversible.
- How can we change the way we evaluate for SEA in order to minimize diagnostic delay and thereby decrease morbidity/mortality?
Incidence/Pathogenesis
- Previously reported to occur in 0.2-1.2 patients per 10,000 hospital admissions in 1975 by Baker et al.1 Has risen to 2.5-3 patients per 10,000 admissions due to an increase in predisposing conditions and spinal instrumentation.2
- Collection of pus or inflammatory granulation between the dura and vertebral column, usually in the wider thoracic/lumbosacral regions containing more infection-prone fat tissue. Extends an average of 3-5 spinal cord segments.3
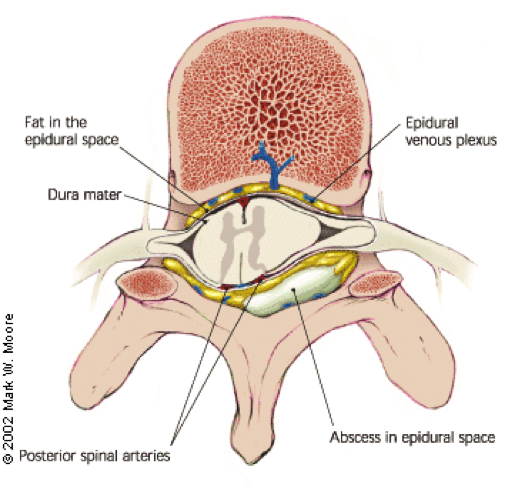
- Entry into epidural space: via contiguous infected tissue (vertebral body, psoas muscle), hematogenous spread (skin, soft-tissue, urinary, and respiratory tract infections), or iatrogenic inoculation (epidural analgesia, paraspinal steroid injection, lumbar puncture, surgery, nerve block). No source identified in 30-40% of cases. 3, 4
- Damage to spinal cord caused by: direct compression, thrombosis, and thrombophlebitis of nearby veins, interruption of arterial blood supply, bacterial toxins, inflammatory mediators.
Risk factors
- Spinal instrumentation, contiguous bony or soft tissue infection, bacteremia secondary to distant infection, diabetes mellitus, HIV, trauma, IV drug abuse, immunosuppressive therapy, cancer, renal failure, alcoholism, tattooing. 5, 6
Classic Triad
- Spinal pain, fever, neurologic deficits (see discussion below).
Diagnosis
- Imaging: Definitive diagnosis made by MRI, with sensitivity and specificity above 90%. 7, 8 Worse outcomes with: central stenosis >50% and abscess length >3 cm. 9
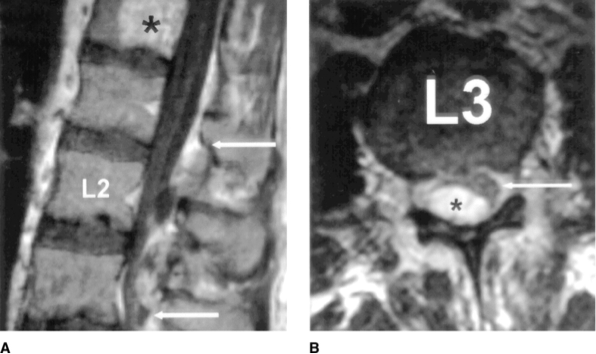
A: arrows delineate abscess margins; B: asterisk – abscess, arrow – thecal sac
http://www.jaaos.org/content/12/3/155/F1.expansion
- Tests: Positive cultures from abscess in 90% and blood cultures 62% 10, and CSF 19% while almost always negative Gram-stain.3 Staph aureus by far most frequent pathogen (60%).11 Lumbar puncture not indicated because as the needle passes through the abscess, pathogens may be iatrogenically pushed into the meninges or subdural space.
- Labs: ESR >20 mm/h is found in up to 95%3, 12 and in all but one of 63 SEA patients in a study by Davis et al.13 Neither ESR, CRP, nor WBC is specific for SEA. Low platelets (<100) and extremely high ESR (>110) predicted a poor outcome in one study of 46 SEA patients. 14
Management
- Goals: reduce abscess size, eliminate abscess, eradicate causative organism.
- Surgery: Most cases call for surgical decompression by laminectomy, hemilaminectomy, or interlaminar fenestration. Neurological improvement unlikely if paresis exceeds 24-36 hours. 15
- CT-guided needle aspiration combined with antibiotics: for patients with posterior SEA, no neurological deficit, high surgical risk, and who do not respond to antibiotics alone.
- Antibiotics alone: if high surgical risk or when neurological deficits are present >3 days and unlikely to improve.
- Antibiotics against Staph, Strep, and Gram-negative bacilli. Example: Vancomycin plus Ceftriaxone/Cefotaxime/Ceftazidime plus Metronidazole.
- Against Pseudomonas if IV drug use, Coag-negative Staph if implanted device such as epidural catheters.
- Duration between 4-16 weeks depending on: co-morbidities, isolated microorganism, bactericidal effect of agent.16 Frequent follow-up of neurological status and MRI studies (after 2-4 weeks) required. Efficacy of non-surgical therapy usually apparent within first 48-72 hours.17
How well do ER physicians diagnose SEA?
- In a study of 63 SEA patients, Davis et al. found that diagnostic delays (multiple ED visits before diagnosis, admission without SEA diagnosis, >24 hrs to a definitive study) were present in 75% of SEA patients.13
Why do we miss it?
- SEA is an extremely rare diagnosis.
- Low back pain is a very common reason for physician visits. It is all-too-easy to attribute to degenerative joint etiology. Symptoms may even be masked by NSAID or steroid use.
- Symptoms to look for are not necessarily present.
- Classic triad present in only 10-15% of cases at first physician contact in Davis et al.’s study. 13
- Fever in only 32% at first ED visit, neurological exam documented as normal in 68%.
- In a review of 75 cases, Rigamonti et al. found the classic triad present in 37%, while 22% had no neurologic deficit with or without back pain.16
- Over a range of studies, back pain and severe local tenderness were the most frequent early findings at 75% and 58%, respectively.13
- Classic triad present in only 10-15% of cases at first physician contact in Davis et al.’s study. 13
- The earliest symptoms are non-specific.
- Stage I: back pain (focal, severe), fever, tenderness.
- Stage II: radicular pain (“shooting”, “electric shocks”), nuchal rigidity/neck stiffness, reflex changes.
- Not until the abscess has lingered or progressed do the obvious symptoms present.
- Stage III: sensory abnormalities, motor weakness, bowel and bladder dysfunction.
- Stage IV: paralysis.
- Time varies from symptom onset to the patient seeking medical attention. Patients thus present at variable stages.
- For Davis et al., mean duration was 5 and 9 days, respectively, with median number of ED visits before admission being 2. 13
- Neurological deficits can be wide-ranging. Motor: focal motor signs along dermatome, complete paraplegia. Sensory: paresthesias, hyperesthesias, pressure sensation.
- Laboratory markers have limited specificity.
- MRI is not always readily available to emergency departments.
- Bed-bound patient sick for other reasons may have “hidden” neurological symptoms.
What are the consequences of missing this diagnosis?
- Increased risk of residual weakness with diagnostic delay vs no delay (45% vs 13%).13
- Symptoms often irreversible by the time they present in Stages III, IV. Almost 50% of survivors with residual neurologic deficits, including 15% with paresis or complete paralysis.16, 18
- Final outcome (after up to 1 year) strongly correlates with severity (Stage III, IV) and duration (>24-36 hours) of neurological deficits before surgery.
- Mortality rates (2-20%) usually due to severe sepsis and in patients with multiple co-morbidities. Worse outcomes associated with leukocytosis (>14), thrombocytopenia (<100), MRSA, prior spinal surgery, corticosteroid treatment, and HIV infection.13
Pearls
- Early diagnosis is the major prognostic factor for favorable outcome.
- Put SEA on the differential for spinal pain and with recent spinal instrumentation.
- Use risk factor assessment rather than “classic triad” exam screening.
- Perform full neurological exam including: reflexes, sensory and motor function, anal sphincter tone, ability to completely void—especially if patient is bed-bound or with other comorbidities. Focus on specific extremities/dermatomes corresponding to affected spine level.
- Consider ESR as screening tool in patients with spinal pain and a risk factor but without neurological deficits.
- Consider urgent MRI for high-risk patients with: neurological deficit and focal back pain, deficit and unexplained fever, deficit and elevated ESR, severe focal back pain and fever, severe focal back pain with markedly elevated ESR, unexplained extremely severe focal back pain. 16
- Advocate for your patient—early surgical intervention unless otherwise indicated.
References / Further Reading
- Baker AS, Ojemann RG, Swartz MN, Richardson EP Jr. Spinal epidural abscess. N Engl J Med 1975; 293:463-8.
- Sampath P, Rigamonti D. Spinal epidural abscess: a review of epidemiology, diagnosis, and treatment. J Spinal Disord 1999; 12:89-93.
- Darouiche RO, Hamill RJ, Greenberg SB, et al. Bacterial spinal epidural abscess. Review of 43 cases and literature survey. Medicine (Baltimore) 1992; 71:369-85.
- Danner RL, Hartman BJ. Update on spinal epidural abscess: 35 cases and review of the literature. Rev Infect Dise 1987; 9:265-74.
- Reynolds F. Neurological infections after neuraxial anesthesia. Anesthesiol Clin 2008; 26:23.
- Reihsaus E, Waldbaur H, Seeling W. Spinal epidural abscess: a meta-analysis of 915 patients. Neurosurg Rev 2000; 23:175-204; discussion 5.
- Angtuaco EJ, McConnell JR, Chadduck WM, Flanigan S. MR imaging of spinal epidural sepsis. Am J Roentgenoli 1987; 149:1249-53.
- Wong D, Raymond NJ. Spinal epidural abscess. N Z Med J 1998; 111:345-7.
- Tung GA, Yim JW, Mermel LA, Philip L, Rogg JM. Spinal epidural abscess: correlation between MRI findings and outcome. Neuroradiology 1999; 41:904-9.
- Gellen BG, Weingarten K, Gamache FW Jr, et al. Epidural Abscess. In: Infections of the Central Nervous System, 2nd Ed, Scheld WM, Whitley RJ, Durack DT (Eds), Lippincott-Raven Publishers, Philadelphia 1997. P 507.
- Curry WT Jr, Hoh BL, Amin-Hanjani S., Eskandar EN. Spinal epidural abscess: clinical presentation, management, and outcome. Surg Neurol 2005; 53:364-71; discussion 71.
- Soehle M, Wallenfang T. Spinal epidural abscesses: clinical manifestations, prognostic factors, and outcomes. Neurosurgery 2002; 51:79-85; discussion 6-7.
- Davis DP, Wold RM, Patel RJ, et al. The clinical presentation and impact of diagnostic delays on emergency department patients with spinal epidural abscess. J Emerg Med 2004; 26:285-91.
- Tang HJ, Lin HJ, Liu YC, Li CM. Spinal epidural abscess—Experience with 46 patients and evaluation of prognostic factors. Journal of Infection 2002; 45:76-81.
- Bluman EM, Palumbo MA, Lucas PR. Spinal epidural abscess in adults. J Am Acad Orthop Surg 2004; 12:155-163.
- Rigamonti D, Liem L, Sampath P, et al. Spinal epidural abscess: contemporary trends in etiology, evaluation, and management. Surg Neurol 1999; 52:189-96; discussion 97.
- Hlavin ML, Kaminski HJ, Ross JS, Ganz E. Spinal epidural abscess: a ten-year perspective. Neurosurgery 1990; 27:177-84.
- Reihsaus E, Waldbaur H, Seeling W. Spinal epidural abscess: a meta-analysis of 915 patients. Neurosurg Rev 2000;23: 175-204.
- http://www.ncbi.nlm.nih.gov/pubmed/21417700
- http://www.ncbi.nlm.nih.gov/pubmed/21308559





1 thought on “Spinal Epidural Abscess”
Pingback: emDOCs.net – Emergency Medicine EducationMedical Malpractice Insights: Anchoring bias, limited differential leads to quadraplegia - emDOCs.net - Emergency Medicine Education