
Author: Brit Long, MD (@long_brit, EM Chief Resident at SAUSHEC, USAF) // Edited by: Alex Koyfman, MD (@EMHighAK, EM Attending Physician, UT Southwestern Medical Center / Parkland Memorial Hospital) and Manpreet Singh, MD (@MPrizzleER – Clinical Instructor & Ultrasound/Med-Ed Fellow / Harbor-UCLA Medical Center)
You’re working a slow Sunday morning ED shift, and you had just grabbed your coffee and sat down when EMS calls with a patient with right-sided hemiparesis. They want to activate a prehospital stroke alert, and you give them the go ahead without asking for any other patient information.
The EMS crew brings in a 42 year-old female with a history of hypertension. The Cincinnati Prehospital Stroke Scale is positive for limb weakness. Initial vital signs and glucose check are normal. You send the patient for a rapid head CT (computed tomography), and neurology calls back to let you know they are on their way to see the patient.
Introduction
Stroke is the third leading cause of death and number one cause of disability in the U.S.1,2 A significant push exists to rapidly diagnose stroke and obtain glucose and head CT in patients with concern for stroke, as provision of thrombolytics requires specific time criteria and contraindication considerations.1-3 However, the diagnosis of stroke is not always straightforward. Classically, strokes present as the sudden onset of a focal neurologic deficit in a vascular distribution. There are multiple diagnoses that may mimic this presentation. Misdiagnosis of stroke ranges from 5% to 31% of patients, which can potentially lead to unnecessary and harmful treatments.4-7
A stroke mimic is defined as a nonvascular disease that presents with stroke-like symptoms, often indistinguishable from an actual stroke. Why does it matter if a mimic is diagnosed as a stroke? Several studies have demonstrated a low risk of symptomatic intracranial hemorrhage from thrombolytics provided to patients with stroke mimic. However, the risk is not 0, but actually closer to 0.5%-1%, or 1 in 100-200 patients.8,9 The harmful side effects of thrombolytics, most commonly bleeding, are not insignificant; thus, accurate diagnosis is essential.
Are there physical exam or history findings that suggest stroke or mimic?
Libman et al. found that abnormal eye movements, increased diastolic blood pressure greater than 90mm Hg, and a history of atrial fibrillation or angina increased the odds of stroke and decreased the odds of a mimic.6 Other findings suggestive of stroke include lateralization to the right or left cerebral hemispheres, symptoms with exact time of onset, history of focal deficit, and ability to determine a clinical stroke subclassification.4,5 Studies have demonstrated that decreased level of consciousness, cognitive dysfunction, and normal eye movements are predictors of mimic.6 Merino et al. found that patients with stroke mimic were younger, more likely female, and were without risk factors (atrial fibrillation, hypertension, and hyperlipidemia).5 However, these findings are not concrete and can only suggest a diagnosis. In fact, the best combination of all predictors leaves 15% of cases misdiagnosed!4-8
Unfortunately, CT scanning and its interpretation are not always reliable in diagnosing acute ischemic stoke or mimic. One study in JAMA 1998 found an accuracy of stroke diagnosis for emergency physicians based on CT to vary from 44% to 85%. Neurologists and radiologists demonstrated higher rates of correct diagnosis of stroke on imaging, but still unreliable in finding small intracranial hemorrhages.10 A second study demonstrated moderate agreement in stroke diagnosis based on CT between physicians (nine neurologists, three ED physicians, two stroke fellows and two radiology fellows) who were participating in the NINDS trial. Agreement was fair (Kappa of 0.20 to 0.39) for subtle findings of stroke (loss of gray-white distinction, hypodensity).11
What are common stroke mimics?
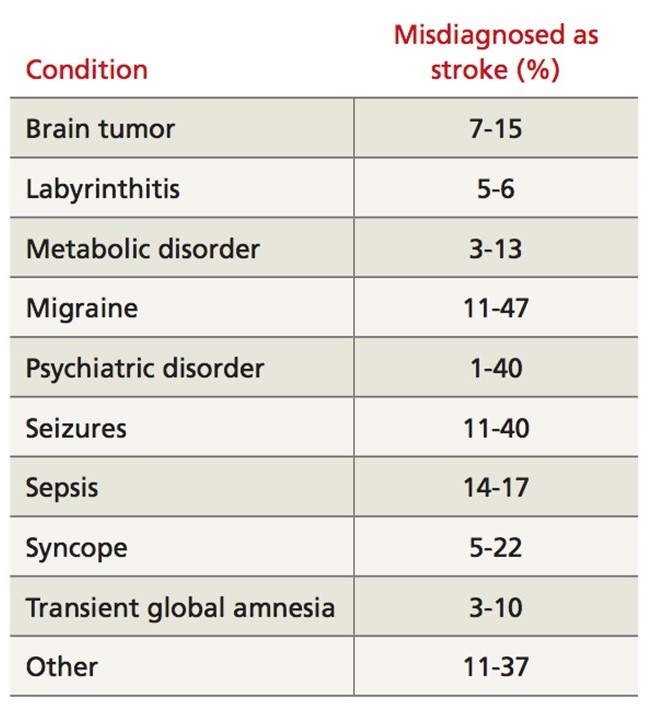
From Konrad CN, Crocco T, Biola J, Larrabee H. Is it stroke, or something else? The Journal of Family Practice. 2010 Jan;59(1):26-31.
Hypoglycemia
One of the first conditions we evaluate for with weakness, syncope, seizure, or focal deficit is hypoglycemia. Hypoglycemia is defined by a blood glucose level less than 45 mg/dl. The exact pathogenesis is not known. Administering IV glucose will usually rapidly resolve the deficit; however, deficit resolution may require several hours, which has been reported in several cases.6,7,12,13
Encephalopathy
Encephalopathy can present with aphasia, homonymous hemianopsia, hemisensory deficits, hemiparesis, unilateral hyperreflexia, and Babinski sign. There are several conditions that can cause encephalopathy, which can be broken into metabolic and infectious causes. Metabolic include hyperglycemia (particularly with hyperosmolar state), hyponatremia, and hepatic encephalopathy. These account for close to 13% of mimics. If hyperglycemic hyperosmolar nonketotic state is present, intravenous fluid should be provided. Insulin is further down the treatment line after fluid repletion is completed. Hyponatremia with focal deficits is most commonly seen in sodium levels less than 120 meq/L. Hypertonic saline 3% can be provided through a peripheral line, with 100cc provided over 10 minutes, followed by a second 100cc over 1 hour.6,7,14-17
Infectious causes include viral encephalitis, especially herpes encephalitis. This disease may present with new psychiatric symptoms, cognitive deficit, seizures, focal deficit, or movement disorder. CT head with lumbar puncture should be obtained with HSV PCR sent. Provide acyclovir at 10mg/kg IV every 8 hours. 4,6,7
Seizure/Postictal State
Seizures often cause neuronal dysfunction that may manifest as weakness, aphasia, confusion, or sensory symptoms. Postictal hemiparesis, or Todd’s Paralysis, is focal weakness localized to one side that can occur in 13% of seizures. It can also affect vision and speech. These deficits usually last up to 20 minutes, but may last 48 hours. Unfortunately, seizures may present in the setting of acute stroke or in patients with a stroke history due to neuronal damage. 6,7,12,13
Systemic Conditions and Infections
Sepsis from any source can result in delirium, weakness, altered speech/dysphagia, and other stroke-like symptoms. Infections account for up to 17% of mimics. Meningitis, encephalopathy (infectious source), and abscess can also present with focal deficits, but other symptoms will usually be present such as neck stiffness, fever, and vital sign abnormalities.6,7
Functional or Psychiatric
Functional causes are diagnoses of exclusion, and likely should not be diagnosed in the ED. Patients with conversion disorder may present with paresis, paralysis, movement disorder, or sensory symptoms. Testing is required for these symptoms including imaging and laboratory studies. Subtle disparities in the physical exam may be found, such as give-way weakness, Hoover’s sign, and “la belle indifference.”6,7,18,19
Mass lesions
These include hematomas, abscesses, and tumors. Typically these present with slowly worsening symptoms over days to months.6,7,20 However, one study demonstrated that 6% of patients with brain tumor presented with symptoms of less than one day in duration, likely due to development of tumor hemorrhage or obstructive hydrocephalus.20 These masses may also affect cerebral vasculature, which can cause focal deficits or seizures.6,7,20
Migraine
Migraines can actually precipitate stroke, but a migraine variant exists called hemiplegic migraine, or migraine with unilateral motor symptoms (MUMS). This may cause unilateral hemiparesis that may precede the migraine, or it may last longer than the migraine. Two thirds of patients with MUMS have ipsilateral weakness to the headache, with most patients demonstrating a “march” of this weakness.23 Other symptoms include vision changes, aphasia, or vertigo. The diagnosis requires a history of recurrent, stereotypical attacks. Do not diagnose this disease at first presentation. These migraine variants usually develop before age 40 years, while the usual age for stroke is approximately 70 years.6,7,21-23
Transient Global Amnesia
This condition is defined by a sudden development of anterograde amnesia with no loss of consciousness, seizures, or other focal deficits. Thus, your neurologic exam is normal except for the memory deficit. Unfortunately, etiology is uncertain. Triggers include severe stress, physical activity, and headaches.24
Where does this leave the emergency physician?
If the neurologic deficit was sudden, try to figure out the onset of symptoms and patient’s baseline. These aspects of the history are essential. Use of a rapid stroke screening tool (Cincinnati Prehospital Stroke Scale, Face Arms Speech Time test, or the Los Angeles Prehospital Stroke Screen) is helpful in rapid evaluation. These tests have a high positive predictive value (87-89%), but there is a large variation in negative predictive value (55%-75%).25
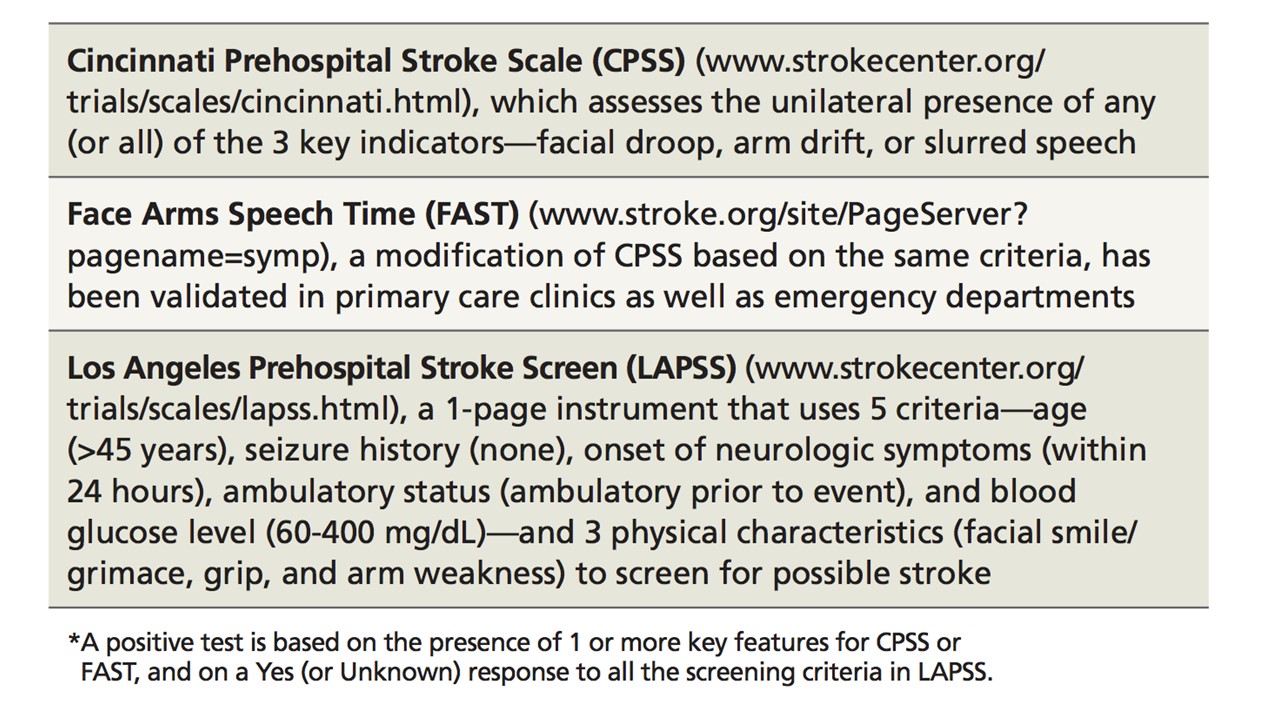
From Konrad CN, Crocco T, Biola J, Larrabee H. Is it stroke, or something else? The Journal of Family Practice. 2010 Jan;59(1):26-31.
Always beware of a stroke mimic and obtain rapid bedside glucose, but ultimately, these patients will require imaging with noncontrast head CT. Time is of the essence, as guidelines call for noncontrast head CT to be completed within 25 minutes of patient arrival to the ED and interpretation within 45 minutes.2,3,25,26 MRI has the advantage of detecting early ischemic changes, diffusion/perfusion mismatch, and posterior fossa abnormalities.27,28 Use of the National Institutes of Health Stroke Scale (NIHSS) can assist providers in recording and focusing the neurologic examination. Neurology consultation if possible is often warranted in these patients, especially with thrombolytic consideration.2,3,25,26
What are strokes that can be missed?
There are several forms of stroke that may present atypically, leaving physicians with a diagnostic dilemma, potentially misdiagnosing stroke as another disease. The majority of strokes present with an acute focal deficit. Several atypical presentations include movement disorders, confusional states, and lacunar strokes. Acute hemiballismus can result from an infarct of the subthalamic nucleus.29,30 One review article found that any dyskinesia, hypokinetic or hyperkinetic, can be found with ischemic lesions at motor cortical or subcortical regions.30 Confusion, agitation, and delirium may present if a lesion in the limbic cortex or orbitofrontal regions occurs.31 Sensory deficits with paresthesias or loss of sensation can occur with parietal and thalamic insults.32
Lacunar strokes are caused by occlusion of a small branch of a larger blood vessel. These smaller vessels are deeper within the central nervous system. There are five categories of lacunar stroke: pure motor, pure sensory, sensorimotor lacunar, ataxic hemiparesis, and dysarthria clumsy-hand syndrome. Due to lack of cortical involvement, these strokes present atypically with specific findings.4,6,7
Summary
Stroke mimics are common, accounting for 5% to 31% of patients with focal neurologic deficit. Diagnosis is not always straightforward, but abnormal eye movements, increased diastolic blood pressure greater than 90mm Hg, and a history of atrial fibrillation or angina are more commonly found in stroke, and decreased level of consciousness, cognitive dysfunction, and normal eye movements are more common with stroke mimic. These are not definitive, and patients will require rapid bedside glucose check and noncontrast head CT. Use of a stroke scale can be beneficial. Common mimics include hypoglycemia, toxins, encephalopathy, postictal state, migraine, functional/psychotic state, and intracranial mass.
References/Further Reading
- Lloyd-Jones D, Adams R, Carnethon M, et al. American Heart Association Statistics Committee and Stroke Statistics Subcommittee. Heart disease and stroke statistics—2009 update: a report from the American Heart Association Statistics Committee and Stroke Statistics Subcommittee. Circulation. 2009;119:480-486.
- Jauch EC, Saver JL, Adams HP Jr, and American Heart Association Stroke Council; Council on Cardiovascular Nursing; Council on Peripheral Vascular Disease; Council on Clinical Cardiology. Guidelines for the early management of patients with acute ischemic stroke: a guideline for healthcare professionals from the American Heart Association/American Stroke Association. Stroke. 2013;44:870–947.
- Adams HP, del Zoppo G, Alberts MJ, et al. Guidelines for early management of adults with ischemic stroke. Circulation. 2007;115:e478-e534.
- Hand PJ, et al, Distinguishing between stroke and mimic at the bedside: the brain attack study. Stroke. March 2006;37:769.
- Merino JG, Luby M, Benson RT, et al. Predictors of acute stroke mimics in 8187 patients referred to a stroke service. J Stroke Cerebrovasc Dis. 2013;22:e397–e403
- Libman RB, Wirkowski E, Alvir J, et al. Conditions that mimic stroke in the emergency department. Implications for acute stroke trials. Arch Neurol. 1995;52:1119-1122.
- Huff JS. Stroke mimics and chameleons. Emerg Med Clin N Am. 2002;20:583-595.
- Tsivgoulis G, Zand R, Katsanos AH, et al. Safety of intravenous thrombolysis in stroke mimics: prospective 5-year study and comprehensive meta-analysis. Stroke. 2015;46:1281-1287.
- Zinkstok SM, Engelter ST, Gensicke H, et al. Safety of thrombolysis in stroke mimics: results from a multicenter cohort study. Stroke. 2013;44:1080–1084.
- Wallis WE, Donaldson I, Scott RS, Wilson J. Hypoglycemia masquerading as cerebrovascular disease (hypoglycemic hemiplegia). Ann Neurol. 1985;18:510-512.
- Malouf R, Brust JC. Hypoglycemia: causes, neurological manifestations, and outcome. Ann Neurol. 1985;17:421-430.
- Blume WT. Focal motor seizures and epilepsia partialis continua. In: Wyllie E, ed. The Treatment of Epilepsy: Principles and Practice. Philadelphia: Lea & Febiger; 1993:393-400.
- Maccario M. Neurological dysfunction associated with nonketotic hyperglycemia. Arch Neurol. 1968;19:525-534.
- Berkovic SF, Bladin PF, Darby DG. Metabolic disorders presenting as stroke. Med J Aust. 1984;140:421-424.
- Atchison JW, Pellegrino M, Herbers P, Tipton B, Matkovic V. Hepatic encephalopathy mimicking stroke. Am J Phys Med Rehabil. 1992;71:114-118.
- Abbot AL, Bladin PF, Donnan GA. Seizures and stroke. In: Bogousslavsky J, Caplan LR, eds. Stroke Syndromes (ed second). Cambridge: Cambridge University Press; 2001:182-191.
- Gallmetzer P, Leutmezer F, Serles W, et al. Postictal paresis in focal epilepsies: incidence, duration, and causes. Neurology. 2004;12:2160-2164.
- Stone J, Zeman A, Sharpe M. Functional weakness and sensory disturbance. J Neurol Neurosurg Psychiatr. 2002;73:241-245.
- Phoebe SC, Tobiano PS, Wang HE, et al. Case of conversion disorder presenting as a severe acute stroke. J Emerg Med. 2006;30:283–286.
- Snyder H, Robinson K, Shah D, Brennan R, Handrigan M. Signs and symptoms of patients with brain tumors presenting to the emergency department. Journ Emerg Med. 1993;11:253-258.
- Bousser MG, Welch KM. Relation between migraine and stroke. Lancet Neurol. 2005;4:533-542.
- Bigal ME, Kurth T, Hu H, et al. Migraine and cardiovascular disease: possible mechanisms of interaction. Neurology. 2009;72:1864-1871.
- Young WB, et al. Migraine with unilateral motor symptoms: a case-control study. J Neurol Neurosurg Psych. June 2007;78:600.
- Quinette P, Guillery-Girard B, Dayan J, et al. What does transient global amnesia really mean? Review of the literature and thorough study of 142 cases. Brain. 2006;129:1640-1658.
- Nor AM, Davis J, Sen B, et al. The recognition of stroke in the emergency room scale: development and validation of a stroke recognition scale. Lancet Neurol. 2005;4:727-734.
- Bock BF. Response system for patients presenting with acute stroke. In: Marler JR, Jones PM, Emr M, ed. Proceeding of a National Symposium on Rapid Identification and Treatment of Acute Stroke: 1997. Bethesda, MD: National Institute of Neurological Disorders and Stroke, National Institutes of Health; 1997.
- Chalela JA, Kidwell CS, Nentwich LM, et al. Magnetic resonance imaging and computerized tomography in emergency assessment of patients with suspected acute stroke—a prospective comparison. Lancet. 2007;369:293-298.
- Kohrmann M, Jüttler E, Huttner HB, et al. Acute stroke imaging for thrombolytic therapy—an update. Cerebrovasc Dis. 2007;24:161-169.
- Klawans HL, Moses H, 3rd, Nausieda PA, Bergen D, Weiner WJ. Treatment and prognosis of hemiballismus. N Engl J Med. 1976;295:1348-1350.
- Ghika J, Bogousslavsky J. Abnormal movements. In: Bogousslavsky J, Caplan LR, eds. Stroke Syndromes (ed second). Cambridge: Cambridge University Press; 2001:162-181.
- Brust JC, Caplan LR. Agitation and delirium. In: Bogousslavsky J, Caplan LR, eds. Stroke Syndromes (ed second). Cambridge: Cambridge University Press; 2001:222-231.
- Kim JS. Sensory abnormality. In: Bogousslavsky J, Caplan LR, eds. Stroke Syndromes (ed second). Cambridge: Cambridge University Press; 2001:34-47.
- Long, B. J., and A. Koyfman. “What Is the Risk of Symptomatic Intracerebral Hemorrhage in Patients With Stroke Mimics Who Receive Intravenous Thrombolytics?.” Annals of emergency medicine 66.6 (2015): 611.
- Alonso, Joaquín Valle, et al. “Varicella zoster encephalitis mimicking stroke.”The American journal of emergency medicine 32.6 (2014): 687-e5.
- Magauran, Brendan G., and Meaghan Nitka. “Stroke mimics.” Emergency medicine clinics of North America 30.3 (2012): 795-804.





4 thoughts on “Stroke Mimics: Pearls and Pitfalls”
Pingback: Global Intensive Care | Stroke Mimics: Pearls and Pitfalls
Pingback: Länkar v13 | Internmedicin
Pingback: Casos em ME 001: AVC isquêmico agudo: Manejo no Departamento de Emergência – Emergência Rules
Pingback: MCQ #16 – M E C C S I G