Thromboelastography (TEG®) for Trauma
By Zachary Radwine MD (Senior EM Resident, UICOMP / OSF St. Francis Medical Center)
Edited by Alex Koyfman MD and Stephen Alerhand MD
General Info
Thromboelastography (TEG®) and rotation thromboelastometry (ROTEM®) are types of viscoelastic hemostatic assays (VHA) that measure the physical properties of blood as it clots. Here we will refer to TEG® as it is the primary test used in the United States. ROTEM® is manufactured in Europe and essentially uses the same technology with slightly different technique and terminology.
Recap Basics
The way it works is elegantly simple: a cup full of blood rotates back and forth around a pin immersed in the blood (Figure 1). An activator is added to accelerate the clotting process. As the blood clots and becomes more viscous it begins to rotate the pin and the device measures the rotational amplitude as this occurs. The readings are then displayed as a tracing (Figure 2,3). This can ideally be done as a POC test and should take the same or less time than conventional coagulations tests.
Each variable corresponds to a physical part of the clotting process:
| Variable | Derangement caused by… | Corresponds to… |
| R=Reaction time |
|
Time to clot formation |
| K=Clot kinetics: time to amplitude of 20mm |
|
Speed of clot formation |
| α=Slope of tangent line at K |
|
Speed of clot propagation |
| MA=Max amplitude |
|
Maximum clot strength |
| Ly30=Percent decrease in amplitude 30min after MA |
|
Speed of clot destruction |
Also keep in mind that shortened R or K/α indicates hypercoagulability.
Dr. Mark Walsh, one of the leading experts on TEG®, proposed using this table to guide transfusion therapy2,3: 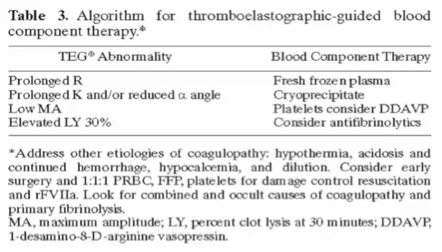
One can quickly see that TEG® offers a much more comprehensive picture of the entire clotting process than routine plasma-based tests, and can be used to tailor transfusion therapy to each individual patient. This is a major shift from the old paradigm.
In the cardiac surgery literature, VHA has been shown to decrease the need for blood products, improve outcomes, and to predict hemorrhage better than conventional tests. More recently, there is emerging evidence in the trauma literature that goal-directed therapy via TEG® leads to a decrease in use of blood products4,5.
There are limitations to VHA:
- Requires daily calibration, up to 3 times per day
- Requires trained personnel
- Susceptible to technical variations
- Does not account for hypothermia (yet)
- May not recognize platelet inhibiting drugs
- Does not account for endothelial effects
- May be inaccurate in blood disorders (e.g. vWD)
What’s New
- Rapid TEG®, or r-TEG®, is a newer method that speeds up the clotting process for faster results. In 2012 Holcomb published a study of 1,974 trauma patients which concluded that conventional coagulation tests could be completely replaced by r-TEG® without a significant increase in cost6.
- A new assay called functional fibrinogen (FF) may help direct treatment more accurately by determining the percent contributions of fibrinogen and platelets to overall clot strength. TEG® is run in the presence of a platelet inhibitor which essentially measures the strength of the fibrin clot without platelets. A recent study showed that in trauma patients, low FF levels are predictive of coagulopathy and increased transfusion needs and high FF levels are predictive of reduced mortality7.
- Measuring the amplitude at 5 (A5) and 10 (A10) minutes after R time both correlate with maximal clot strength (MA) and may give an even more rapid assessment of the need for blood products8.
- LY30 >8% is an independent predictor of mortality at 24 hours in trauma patients and may support early use of antifibrinolytics9.
Bottom Line/Pearls & Pitfalls
- TEG® measures the viscoelastic properties of whole blood and can be used for goal-directed transfusion therapy.
- Direct transfusion therapy at correcting the four main variables:
- FFP for prolonged R
- Cryoprecipitate for prolonged K or reduced α
- Platelets and/or DDAVP for low MA
- Antifibrinolytics (e.g. tranexamic acid) for elevated LY30
- Beware of special circumstances: e.g. platelet inhibitors, hypothermia, bleeding disorders
- r-TEG® and A5/A10 are faster methods of obtaining information needed to direct transfusion therapy.
- FF may be used at some point for even more specific therapy with regards to fibrinogen or platelets to increase clot strength.
- Elevated LY30 is an independent predictor of mortality in trauma patients and supports the early use of antifibrinolytics in these patients.
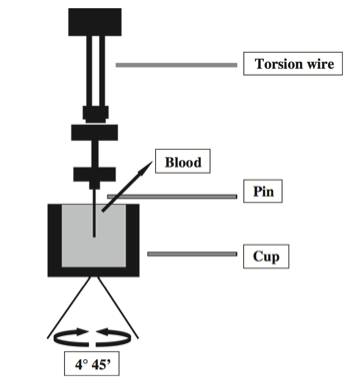 Figure 1: Schematic of TEG® Apparatus10
Figure 1: Schematic of TEG® Apparatus10

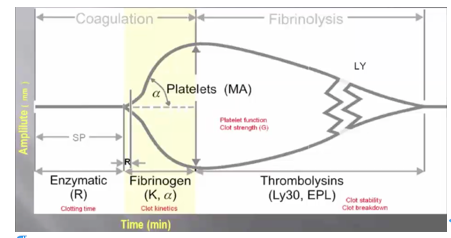 Figure 2: TEG® Tracing with measured variables3
Figure 2: TEG® Tracing with measured variables3
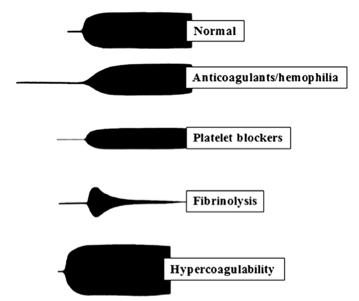 Figure 3: Important TEG® Tracings10
Figure 3: Important TEG® Tracings10
Further Reading
- Bollinger D, Seeberger M, Tanaka K. Principles and practice of thromboelastography in clinical coagulation management and transfusion practice. Transfusion Medicine Review. 2012;26(1):1-13.
- Walsh M, Thomas SG, Howard JC, et al. Blood component therapy in trauma guided with the utilization of the perfusionist and thromboelastography. Journal of Extra-Corporeal Technology. 2011 Sep; 43(3):162-7.
- http://marylandccproject.org/core-content/utility-teg-blood-component-therapy/
- Johansson P. Coagulation monitoring of the bleeding traumatized patient. Curr Opin Anesthesiol. 2012;25:235-41.
- Yin J, et al. Goal-directed transfusion protocol via thromboelastography in patients with abdominal trauma: a retrospective study. World Journal of Emergency Surgery. 2014;9:28
- Holcomb JB, et al. Admission rapid thromboelastography can replace conventional coagulation tests in the emergency department. Annals of Surgery. 2012;256(3):476-86.
- Kornblith LZ, et al. Fibrinogen and platelet contributions to clot formation: implications for trauma resuscitation and thromboprophylaxis. J Trauma Acute Care Surg. 2014;72(2):255-6.
- Meyer AS, et al. Thromboelastography and rotational thromboelastography early amplitudes in 182 trauma patients with clinical suspicion of severe injury. J Trauma Acute Care Surg. 2014;76(3):682-90.
- Hampton DA, et al. A predictive model of early mortality in trauma patients. Am J Surg. 2014;207:642-47
- da Luz LT, Nascimento B, Rizoli S. Thromboelastography (TEG®): practical considerations on its clinical use in trauma resuscitation. Scand J Trauma Resusc Emerg Med. 2013;16:21-29.
- Brazzel C. Thromboelastography-guided transfusion therapy in the trauma patient. AANA J. 2013;81(2):127-32
- Durila M, Malosek M. Rotational thromboelastometry along with thromboelastography plays a critical role in the management of traumatic bleeding. Am J Emerg Med. 2014;32:288.e1-288.e3.
- Kashuk JL, et al. Initial experiences with point-of-care rapid thromboelastography for management of life-threatening postinjury coagulopathy. Transfusion. 2012;52:23-33.
- http://www.ncbi.nlm.nih.gov/pubmed/22046550
- http://www.ncbi.nlm.nih.gov/pubmed/24317351





2 thoughts on “Thromboelastography (TEG®) for Trauma”
Pingback: ROTEM in Trauma: Blood is thicker with Wine - Part 1 - EMOttawa
Pingback: ROTEM in Trauma: Blood is thicker with Wine - Part 2 - EMOttawa