Authors: Armand Tadjali, MD (Emergency Medicine Resident, Carolinas Medical Center); Ann-Jeannette Geib, MD (EM Attending Physician, Medical Toxicologist, Carolinas Medical Center, Charlotte, NC) // Reviewed by: Tony Spadaro, MD (Medical Toxicology Fellow, Rutgers New Jersey Medical School, Newark, NJ); Alex Koyfman, MD (@EMHighAK); Brit Long, MD (@long_brit)

Case:
A 54-year-old male with past medical history significant for schizophrenia is presenting to the emergency department for psychiatric evaluation. He states that he is hearing voices that others cannot hear and seeing “shadowy figures” despite taking his prescribed haloperidol. During your interview, you note that in between answering your questions, he is protruding his tongue, puckering his mouth, and smacking his lips together. He denies any somatic symptoms and vital signs are within normal limits. Physical exam is otherwise unremarkable.
Questions:
- How does tardive dyskinesia (TD) present?
- What medications/risk factors are present for TD?
- Are there any preventative measures for TD that can be taken?
- What is the treatment for TD?
Background:
- TD is typically seen with first generation antipsychotic (FGA) medications, but may be seen with second generation antipsychotics (SGA), or any other dopamine blocking agents
- FGAs are associated with a greater risk of TD than SGAs.1
- Higher doses of antipsychotics are associated with a greater risk of TD1
- Generally, the lowest dose is started in antipsychotics to avoid TD, as well as many other possible side effects.
- This also functions in a cumulative fashion as well. Those who are on antipsychotics for prolonged periods of time have a higher risk of developing TD.1
- The mean prevalence of TD is 25% of people on antipsychotics globally1
- This is about 30% in those who use FGA, 25% in those who use SGA
- TD is particularly distressing to patients
- Studies have demonstrated that patients feel social isolation and have difficulties participating in daily activities secondary to their TD.1
- Pathophysiology
- Not fully understood, but two theories do exist:
- Dopamine supersensitivity hypothesis2
- Due to long-term blockage of dopamine receptors, specifically D2, in the striatal area, receptors become more sensitive (supersensitive) to dopamine and will bind dopamine at lower concentrations leading to dyskinesia.
- This is backed by the observation that higher doses of antipsychotics confer a greater risk for developing TD.1
- This is also backed by evidence that those with primary parkinsonism have a higher risk of developing TD.
- Counterarguments to this hypothesis include: dopamine receptors become supersensitive after a few weeks, but TD takes much longer to develop; while most patients develop supersensitivity most do not develop TD; and after antipsychotic cessation supersensitivity will diminish, but TD persists.
- Neurotoxicity hypothesis2
- It is believed that free radicals are produced through increased metabolization of dopamine into its products, 3,4-dihydroxyphenlacetic acid and homovanillic acid, with the release of hydrogen peroxide as a byproduct.
- This can lead to permanent damage, which explains why TD persists despite medication cessation.
- This is further supported by TD being more prevalent in older age when patients are more susceptible to damage from these effects
- There may also be a genetic basis for the development of TD, those with certain polymorphisms in the dopamine receptor may be more susceptible.1
- Demographic factors such as older age, female sex, and Black ethnicity confer a higher risk (see Table 1 for a comprehensive list).1

Adapted from: Daneshvari, N. O., MD. (2024). Tardive Dyskinesia: Etiology, Prevention, and management. Psychiatrist.com. https://www.psychiatrist.com/pcc/tardive-dyskinesia-etiology-prevention-management/
Clinical Presentation:
- Rhythmic involuntary movements, characterized classically by movements of the face, but can include movements in the trunk, that do not fade with distraction.
- Movements may involve the tongue, facial muscles, lips, or eyes.
- Movements may be choreiform, athetoid, or semirhythmic3
- Do not confuse these movements for medication induced parkinsonism, which is more tremulous in nature.4
- In patients suspected to have medication induced parkinsonism, the treatment, benztropine, may actually worsen the symptoms of tardive dyskinesia.4,5
- Severity can be assessed using the Abnormal Involuntary Movement Scale (AIMS)6
- Mild movements in two areas, or moderate movements in one area, are sufficient for diagnosis of TD.
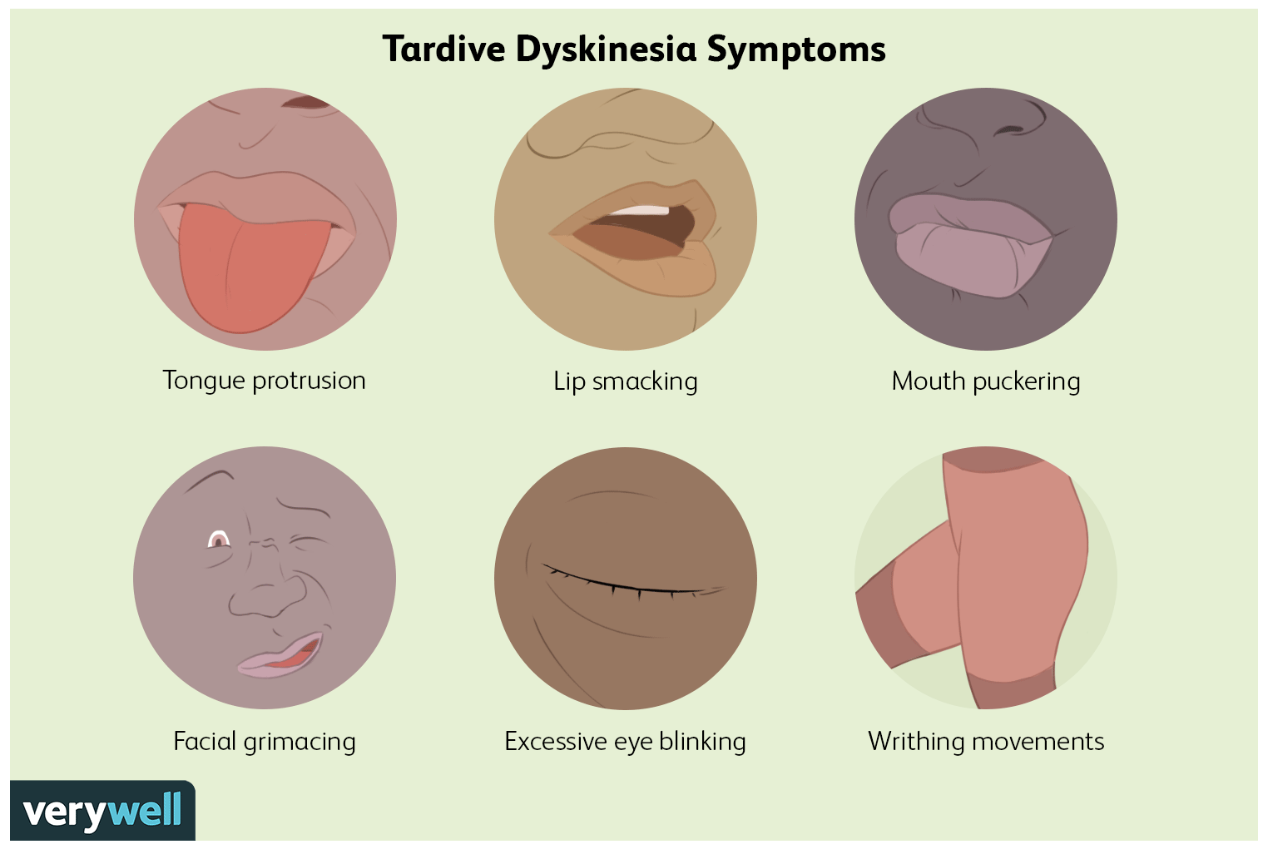
Adapted from: Jividen, S., RN. (2024, June 14). Early signs of tardive dyskinesia. Verywell Health. https://www.verywellhealth.com/early-signs-of-tardive-dyskinesia-5203050
Diagnosis:
- DSM-V diagnosis requires3:
- At least 4 weeks of typical dyskinetic movements
- Development of symptoms following anti-dopaminergic medication administration
- Classically this would be first- or second-generation antipsychotics but may be expanded to any medication that has a postsynaptic dopamine inhibition, such as metoclopramide.
- The patient must have been on the offending agent for at least 1 month if age >60, or at least 3 months if below this age
- May also make the diagnosis if symptoms develop during first 4 weeks following medication cessation for oral medications or 8 weeks for long-acting injectable medications.
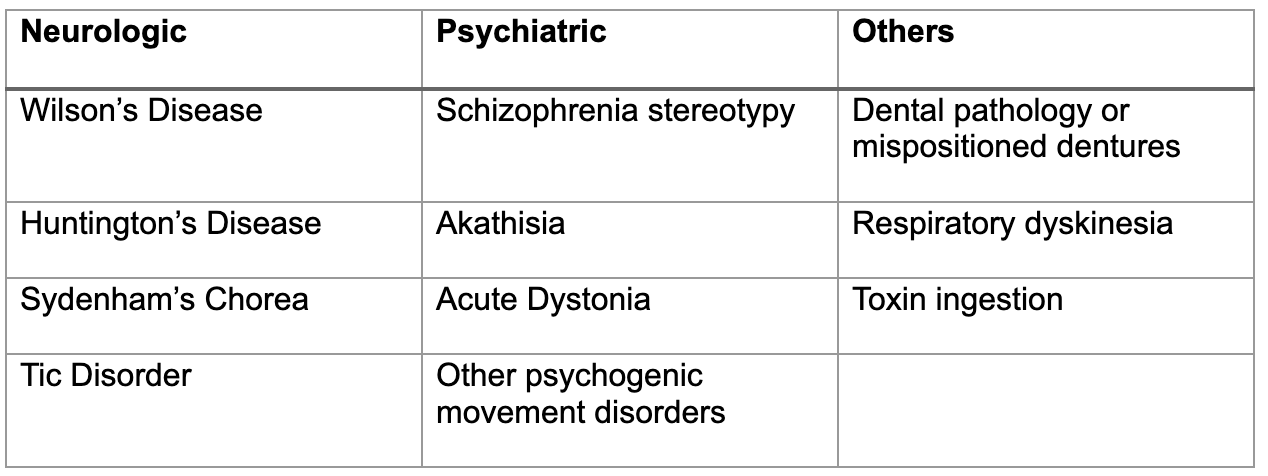
Table 2: Differential Diagnosis for TD
Management:
- Management is multifactorial, based on the patient’s response to the medications they are currently on and how many antipsychotic medications they have been on in the past.
- Regardless of treatment, patients may have TD permanently, based on the length of time, as well as the severity of their TD, which tend to correlate.2
- The first intervention to consider is whether antipsychotics can be weaned.
- If the dosage can be lowered safely, this can be done in the outpatient psychiatric setting, to monitor for development of any psychotic features.
- If the patient is currently on a higher risk medication (FGA), you may also consider changing this to a lower risk medication (SGA).
- Clozapine has one of the lowest risks amongst antipsychotic medications.2
- Vesicular Monoamine Transporter 2 (VMAT2) inhibitors
- This is the first class of FDA-approved medications to treat TD. Deutetrabenazine and valbenazine are approved specifically for TD; tetrabenazine is approved for Huntington’s chorea only but has been used off label for TD.
- Deutetrabenazine and valbenazine appear to have better efficacy and have a level A recommendation compared to tetrabenazine which has a level C recommendation.5
- VMAT2 inhibitors function by reducing presynaptic monoamines, especially dopamine in central neurons, as compared to VMAT1 which functions in both central and the periphery.5
- The most efficacious therapy for TD treatment, although can be cost prohibitive.
- Deutetrabenazine (Austedo™) and Valbenazine are currently exorbitantly expensive and is generally not covered by insurance. However, tetrabenazine, from which deutetrabenazine is derived, is more reasonably priced.
- Other medications have been shown to be effective, although not as much as VMAT2 inhibitors.
- Benzodiazepines
-
- Clonazepam has the most evidence to support its efficacy, with a level B recommendation.5
- Patients were noted to have a statistically significant reduction in symptoms after 12 weeks, but there are important safety concerns with using benzodiazepines, such as withdrawal when stopped suddenly, oversedation, delirium, and dementia.
-
- Ginkgo biloba5
-
-
-
- Level B recommendation for treatment of TD
- Functions as an antioxidant
- Patients had a statistically significant reduction in their AIMS scores following ginkgo use for 12 weeks at a dose of 240mg daily.
- However this is a non-prescription and non-FDA approved herbal supplement and lacks dose and ingredient standardization, which limits its use.
-
-
- Amantadine5
- Level C recommendation
- NMDA antagonist with anti-glutamatergic qualities, most often associated with treatment of dyskinesias created by treatments for parkinsonism
- Studies have demonstrated mixed results and have been overall limited but generally have been shown to be efficacious in short term use of amantadine.
- Botulinum toxin5
- Level U recommendation
- No controlled studies have been performed in the setting of TD yet.
- A single blind study has demonstrated decrease in severity of TD following injections every 3 months over a 3-treatment course. Injections are made in the muscle groups most severely affected by TD.
- This treatment modality requires frequent reinjection and office visits, which may be cost and/or time prohibitive to the patient.
- Non-pharmacologic treatment modalities
- Deep brain stimulation5
- Level C recommendation
- Generally used in those with severe, refractory cases
- Bilateral posteroventral globus pallidus internus is targeted most commonly
- Limited research with no controlled studies described in the literature yet
- Electroconvulsive therapy5
- Level U recommendation
- Generally limited to case reports and outdated literature
- Used as a treatment for depression or schizophrenia where the patients happened to have TD as well.
- There has been some evidence to suggest that free radical scavengers, including Vitamins E, D, and B6 have beneficial outcomes on patients with early TD (within the first 3 years of symptom development).2
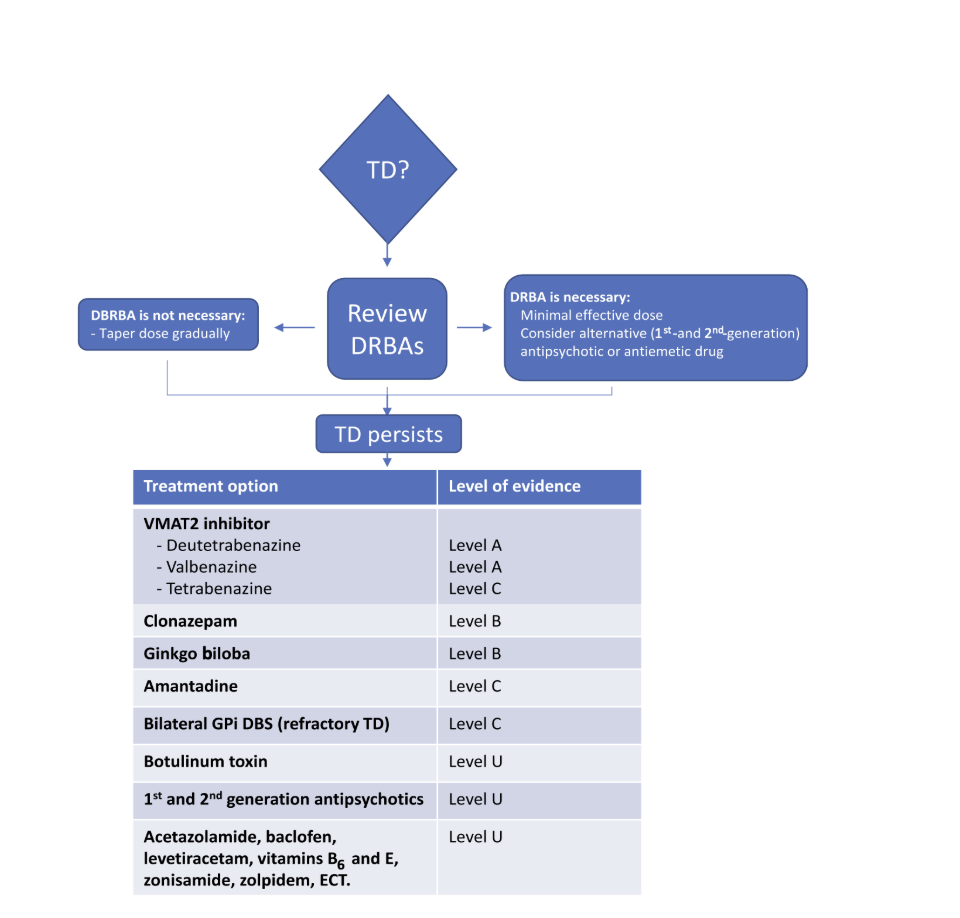
Adapted from: Bashir, H. H., & Jankovic, J. (2020). Treatment of Tardive Dyskinesia. Neurologic clinics, 38(2), 379–396. https://doi.org/10.1016/j.ncl.2020.01.004
Case Follow-up:
The patient was placed under involuntary commitment due to responding to internal stimuli and concern for threat of self-harm. While inpatient, he was weaned off of haloperidol and started on olanzapine with decrease in TD symptoms.
Clinical Pearls:
- TD presents as a group of involuntary movements, typically of the lips, tongue, or face, following at least 3 months of antidopaminergic medication use in patients age < 60 or 1 month for patients age >60.
- Always attempt to minimize the dose of antidopaminergic medications used in patients, as well as the amount of time they are on these medications.
- TD may be a permanent outcome if not recognized early and treated accordingly. Patients require regular follow-up care, especially if adjustments are made to their antipsychotic medication management.
- To address TD, start with a complete history for the patient, and attempt to change FGAs to SGAs if the patient will tolerate. You may also attempt to lower medication doses, if applicable. Psychiatric consultation should be considered.
- VMAT2 inhibitor medications are a new class that have been shown to decrease TD symptoms but are unlikely to be accessible to most given cost barriers.
- The risk of TD generally does not outweigh the benefits that antidopaminergic medications may pose in an acute setting, such as an emergency department. Antipsychotic medications for agitation, or other antidopaminergic medications used for therapies such as an antiemetics, should be used in these settings if deemed clinically necessary.

Adapted from: Babadi, B., MD, PhD, & Lim, C., MD, MPH. (2025). Tardive Dyskinesia. In Ferri’s Clinical Advisor 2025 (1st ed., pp. 1053–1054). https://www-clinicalkey-com.wake.idm.oclc.org/#!/content/book/3-s2.0-B9780443117244009893?scrollTo=%23hl0000174
References:
- Daneshvari, N. O., MD. (2024). Tardive Dyskinesia: Etiology, Prevention, and management. Psychiatrist.com. https://www.psychiatrist.com/pcc/tardive-dyskinesia-etiology-prevention-management/
- Van Harten, P., MD, PhD, & Tenback, D., MD, PhD. (2011). Tardive Dyskinesia: Clinical Presentation and Treatment. International Review of Neurobiology, 98, 187–210. https://doi.org/10.1016/B978-0-12-381328-2.00008-0
- American Psychiatric Association. (2013). Tardive Dyskinesia. In Diagnostic and statistical manual of mental disorders (5th ed.). https://doi.org/10.1176/appi.books.9780890425596.
- Ward, K. M., & Citrome, L. (2018). Antipsychotic-Related Movement Disorders: Drug-Induced Parkinsonism vs. Tardive Dyskinesia-Key Differences in Pathophysiology and Clinical Management. Neurology and therapy, 7(2), 233–248. https://doi.org/10.1007/s40120-018-0105-0
- Bashir, H. H., & Jankovic, J. (2020). Treatment of Tardive Dyskinesia. Neurologic clinics, 38(2), 379–396. https://doi.org/10.1016/j.ncl.2020.01.004
- Public Health Service, Alcohol, Drug Abuse, and Mental Health Administration, & National Institute of Mental Health. (2000). ABNORMAL INVOLUNTARY MOVEMENT SCALE (AIMS). https://www.aacap.org/App_Themes/AACAP/docs/member_resources/toolbox_for_clinical_practice_and_outcomes/monitoring/AIMS.pdf




