Ultrasound for Pneumonia in the ED
By Stephen Alerhand (@SAlerhand)
EM Resident Physician, Icahn School of Medicine at Mount Sinai
Edited by Alex Koyfman MD (@EMHighAK)
Patient Case
A 62 year-old obese male with a past medical history of diabetes and hypertension, is brought in by EMS at 3 AM complaining of subjective fever and weakness for 3 days. The patient appears fatigued, so his wife communicates on his behalf. He had been in is his usual state of health until demonstrating a marked decrease in energy 3 days ago of unclear origin. He denies cough, chest pain/palpitations, nausea/vomiting/diarrhea, or lower-extremity swelling. He denies recent travel, sick contacts, or a change in medications.
ED vitals: T 100.2, HR 80, BP 105/80, O2 sat 96% on room air.
Exam: Fatigued-appearing obese male, lung sounds unremarkable though diminished 2/2 body habitus, otherwise unremarkable.
Despite his overtly fatigued appearance, the patient’s vital signs do not meet SIRS criteria, and the nurses happen to triage him to one of the regular areas of the emergency department, where he will likely wait a little awhile before being seen by a resident.
Shortly thereafter, on her routine check of patients in the corner pocket of the ED, a nurse documents new vitals and presents them to the attending:
T 101.2, HR 90, BP 95/60, O2 sat 90% on room air
Along with his fatigued appearance (now critically assessed without the anchoring bias of ‘normal’ vital signs), the patient meets SIRS criteria and is transferred to the critical care/resuscitation area of the ED. Oxygen is administered, the patient is put on a monitor, and another peripheral IV line is obtained.
The resident suspects infection and considers pneumonia due to the fever and oxygen requirement. Unfortunately, the patient’s obesity contributes to suboptimal assessment. Specifically, lung sounds are again difficult to auscultate through the soft tissue, his weight makes him difficult to turn, and the STAT portable chest x-ray provides minimal diagnostic information.
Ultrasound Application
The resident grabs the ultrasound, sticks the probe on the patient’s right flank, and within 20 seconds reveals a lung consolidation to the rest of the team, promptly initiating antibiotic treatment specifically geared towards pneumonia. His attending physician, having practiced for 30 years in the community setting, cannot help but be impressed with his resident’s use of point-of-care ultrasound to diagnose pneumonia when “everybody knows that chest x-ray is the diagnostic imaging modality of choice.”
The Literature
Citation: Cortellaro, F. et al. Lung ultrasound is an accurate diagnostic tool for the diagnosis of pneumonia in the emergency department. Emerg Med J 2012;29:19-23.
Type of Study: Prospective (n=81)
Objective: To evaluate diagnostic accuracy of US
Results: US sensitivity 98%, specificity 85%. Exam always performed in < 5 min. CXR sensitivity 67%, specificity 85%.
Conclusion: US reliable for diagnosing PNA in ED, probably superior to CXR. Faster diagnosis. More timely therapy.
Citation: Parlamento, S. Copetti, R. di Bartolomeo, S. Evaluation of lung ultrasound for the diagnosis of pneumonia in the ED. Amer Journ EM 2009; 27:379-384.
Type of Study: Prospective (n=49)
Objective: Assess ability of US to confirm PNA and feasibility of integration into common ED practice
Results: US confirmed PNA in 32 of 49 (65.3%). In this group, 31 positive US (96.9% sensitivity), 24 positive CXR (75% sensitivity). Thus, 8 w/ positive US and negative CXR. Follow-up was consistent with diagnoses.
Conclusion: Bedside, reliable, rapid, noninvasive. Could have significant role in ED.
Citation: Reissig, A. Kroegel, C. Sonographic diagnosis and follow-up of pneumonia: a prospective study. Respiration 2007;74:537-547.
Type of Study: Prospective
Objective: To evaluate sonographic features of PNA at admission and during course of treatment
Results: Most characteristic feature of PNA was a positive bronchoaerogram. During follow-up, it decreased in size/number and disappeared quite often.
Conclusion: US well-suited for follow-up of PNA.
Citation: Chavez, M. Shams, N. Ellington, L. Lung ultrasound for the diagnosis of pneumonia in adults: a systematic review and meta-analysis. Respiratory Research 2014; 15:50.
Type of Study: Meta-analysis (n=1172)
Objective: Summarize existing evidence of diagnostic accuracy of US for PNA
Results: US took maximum of 13 min to conduct. Sensitivity and specificity of 94% and 96%, respectively.
Conclusion: US by highly-skilled sonographers performs well for diagnosing PNA.
Citation: Hu, J. et al. Diagnostic performance of lung ultrasound in the diagnosis of pneumonia: a bivariate meta-analysis. Int J Clin Med 2014;7(1):115-121.
Type of Study: Meta-analysis (n=1080)
Objective: To establish diagnostic accuracy of US for PNA
Results: Sensitivity 97%, specificity 94%, positive likelihood ratio 15.62, negative likelihood ratio 0.03.
Conclusion: High accuracy. Promising attractive alternative.
Tips/Tricks/Notes for Performing US to Evaluate for PNA
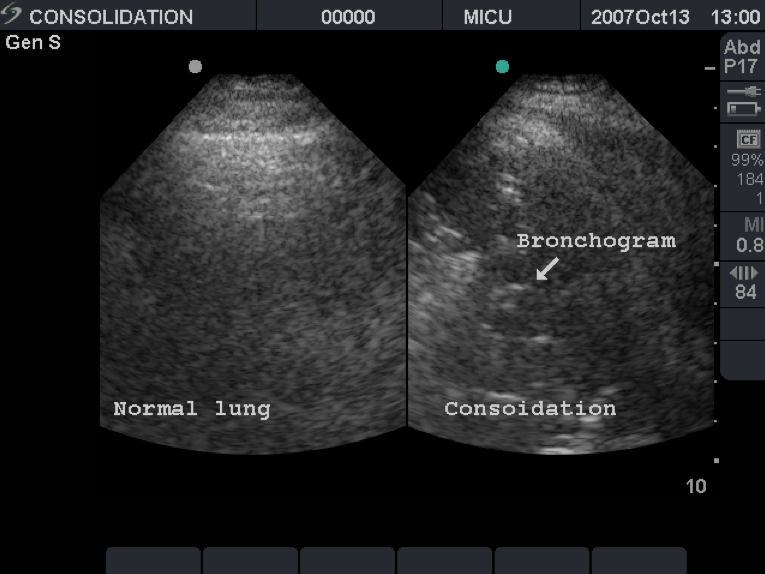
- In pneumonia, alveoli accumulate with infectious contents. Sound waves travel through this matter as they would for soft tissue organs, such as the liver. The image on screen becomes solid and homogenous. Unsurprisingly, this concept is called “hepatization.”
- Low-frequency probe preferred for imaging of deep lung tissues
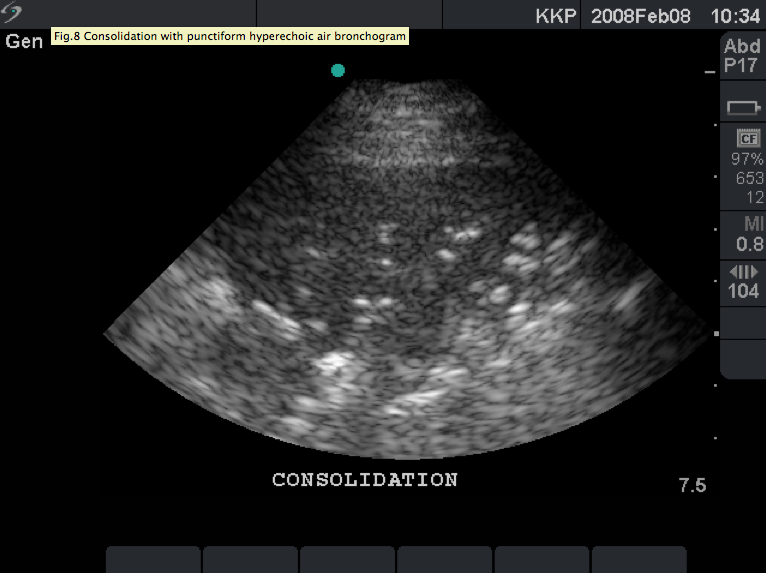
- Within a consolidation, hyperechoic air bronchograms correspond to air in the bronchi. These air bubbles within the consolidation move with respiration, whereas the consolidation size does not change (unlike with a pleural effusion)
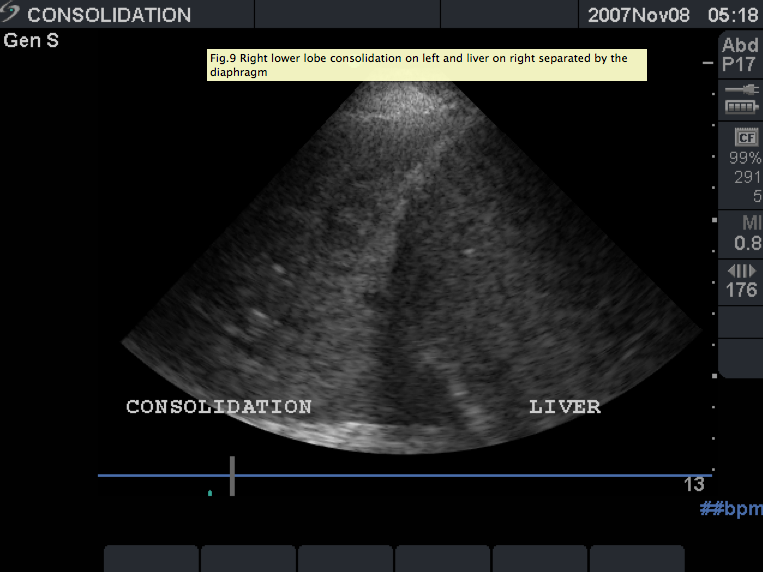
- Locate the diaphragm within the picture, as the liver and consolidation can appear similar.
- Look along posterior axillary line in obese patients.

Advantages of Ultrasound versus X-ray
- Real-time assessment of deterioration and/or response to treatment. Conversely, chest x-ray findings lag behind actual clinical lung exam.
- Excellent for serial monitoring
- Portable
- Earlier diagnosis, earlier therapy
- Less radiation
- Cheaper
- Better sensitivity/specificity as noted in several studies (see Literature above)
- Distinguishes between lung consolidation and atelectasis
- Air moving within bronchi will have bright and shimmery appearance of dynamic air bronchograms.
- In contrast, for atelectasis, the air within the consolidation is static.
- Also great for ICU care to follow dynamic lung changes for patients who can only get Portable films and not be transported for AP/Lateral films
Further References
–http://www.criticalecho.com/content/tutorial-9-lung-ultrasound (images)
–http://www.critcaresono.com/page.php?page=27
–Introduction to Ultrasound, by Matt Dawson and Mike Mallin
— http://www.ncbi.nlm.nih.gov/pubmed/25758182




