Originally published on Ultrasound G.E.L. on 11/21/16 – Visit HERE to listen to accompanying PODCAST! Reposted with permission.
Follow Dr. Michael Prats, MD (@PratsEM), Dr. Creagh Bougler, MD (@CreaghB), and Dr. Jacob Avila, MD (@UltrasoundMD) from Ultrasound G.E.L. team!
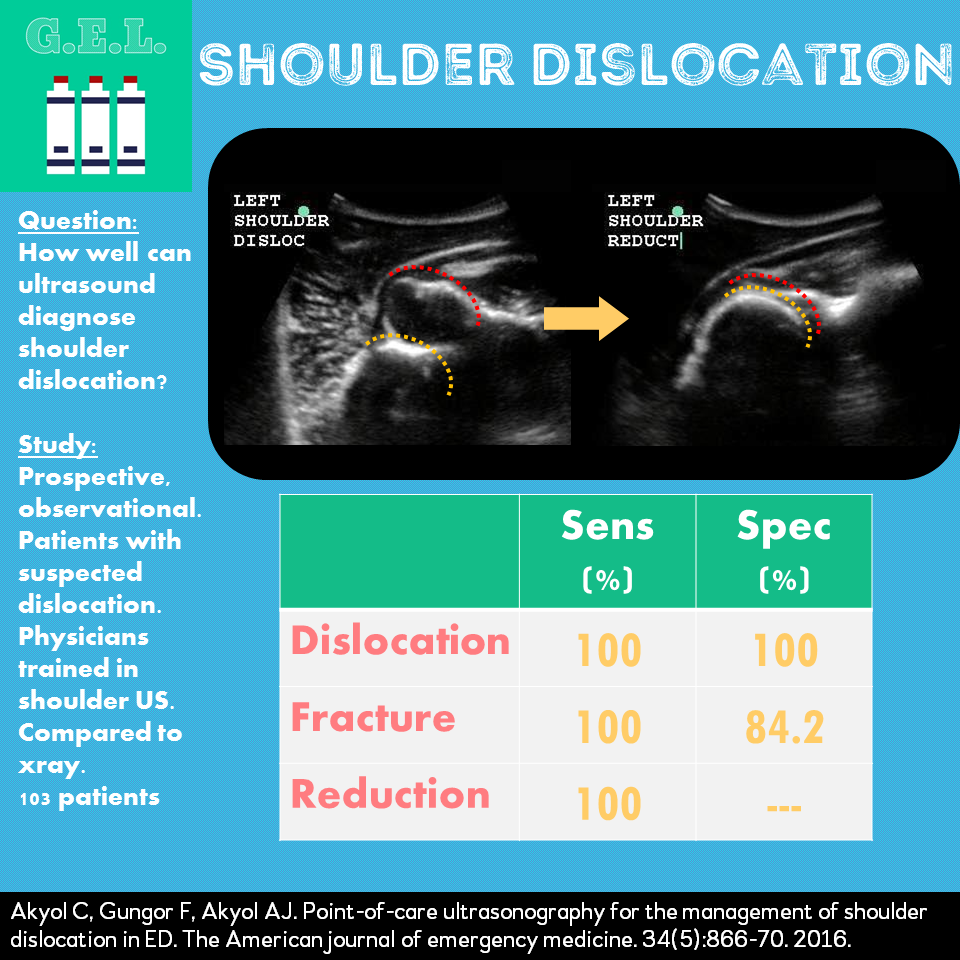
Point-of-care ultrasonography for the management of shoulder dislocation in ED
American Journal of Emergency Medicine May 2016 – Pubmed Link
Background
Joint dislocations are common, and the shoulder is half of all joint dislocations. In the emergency department, we traditionally confirm the diagnosis on xray, reduce the shoulder (interscalene block anyone?), and then confirm reduction on post reduction xray films. The usual downsides of xray compared to ultrasound apply here – more time, more radiation, and having only a static image. Ultrasound potentially offers a way to diagnose shoulder dislocation, but how well does it perform in doing so?
Questions
How does POCUS compare with xray in diagnosing shoulder xray?
How does POCUS compare with xray in diagnosing fractures and verifying reduction?
Population
Prospective, observational, convenience sample
2 hospitals, one academic
Inclusion:
- greater than 15 years old with suspected dislocation on exam
- Only enrolled during shifts that attendings trained were working
Exclusion:
- younger than 15 (unclear what would happen if they arrived on their 15th birthday)
- multiple trauma
- unstable vital signs
- refused to consent
- fracture diagnosis prior to POCUS
- open dislocation
- those in whom reduction was not accomplished
Who did the scans?
8 emergency physicians
Given special training for the study
- 30 min lecture
- 2 hours of practicing including diagnosing fracture in greater and lesser tubercles, humeral head, humeral neck, and glenoid rim. Also identifying hill sachs and bankart fractures.
Design
Prospective convenience sample when any of 8 study physicians available
No blinding
No Randomization
Intervention
Study patients received POCUS of the shoulder prior to xray and then again after reduction attempt.
Scan
Probe choice: In this study a high frequency linear probe was used. You can also use a curvilinear probe.
Step 1: view shaft of humerus in short axis, posteriorly.
Step 2: slide up to find humeral head
Step 3: slide laterally to view GH joint and posterior glenoid labrum
Step 4: evaluate humeral head, tuberosities and intertubercular groove by sliding around anteriorly
One Minute Ultrasound Video – Shoulder dislocation
Results
103 Patients
98 (95.1%) had dislocation
Primary Findings
POCUS for dislocation: 100% sens and 100% specific for dislocation
Secondary Findings
POCUS for fracture: 100% sensitive, 84.2% specific (only 9 fractures overall)
POCUS for reduction: 100% sensitive (*incorrectly reported in paper as 100% specific – because there were no negative xrays, there were no true negatives, can’t calculate specificity)
In this study, sonologists could not accurately determine anterior versus posterior dislocation.
Limitations
Convenience sample
High incidence of dislocation in this population
Extensive shoulder US use of study sonologists
If unsure if pathology present – instructed to rate as “pathology” –> likely attributed to high sensitivities
Take Home Points
1. Ultrasound can be used to diagnose shoulder dislocation and reduction. In this study 100% sensitive and specific.
2. With training, ultrasound can also recognize shoulder fractures with high sensitivity.
Our score





