Ultrasound-Guided Hematoma Block
By Stephen Alerhand MD
Resident Physician, Icahn School of Medicine at Mount Sinai
Edited by Alex Koyfman MD
Your fantasy football team is dominating its opponent in your residency league’s semi-finals, and you’re bragging loudly to anybody on shift who will listen. Suddenly, the ESPN App alert pops up on your phone stating that your starting running back left the game early with a wrist injury. One hour and several towels’ worth of sweat later, you learn that the running back suffered a mildly displaced distal radius fracture and is listed as questionable for the NFL’s slate of Week 16 games – your fantasy football championship.


You take out a loan, board a short flight, and find yourself alongside the team’s physician evaluating the running back’s wrist. The team physician prepares to reduce the fracture and splint it. However, to the surprise of all, this otherwise tough-as-nails running back is apparently deathly afraid of needles. You also note the significant soft tissue swelling in the running back’s already freakishly muscular forearm. You know that the longer it takes to reduce the fracture, the less easy the procedure will be and the less likely it will heal adequately.
Everybody in the room is anxious: the running back in pain and fearful of the needle, the coach hoping to have his star player in the lineup, the team owner regretting the huge contract recently doled out… but most of all, you, the resident physician and fantasy football owner set to face that annoying gunner intern in the fantasy football championship next weekend for residency bragging rights.

You take out your hand-held ultrasound probe and reach out for the running back’s wrist. Just when the police are about to arrest you, you flash your medical badge and take out a set of journal articles describing ultrasound-guided hematoma block.
Fathi, M. et al. Ultrasound-guided hematoma block in distal radius fracture reduction: a randomized clinical trial. Emerg Med J. 2014 Jul 12.
Comparison: US-guided (10 mL of 1% Lidocaine) versus procedural sedation and analgesia (Versed/Fentanyl). N=143.
Outcome Measure: Self-reported pain on numeric rating scale
Results: No significant differences in pain scores before, during, 5 min after, and 15 min after reduction. Similar patient and physician overall satisfaction. Significantly decreased time to discharge in US-guided hematoma block group.
Conclusion: US-guided hematoma block is safe and effective.
Compared to PSA:
– No difference in pain
– Faster
– Less use of resources (no respiratory/circulatory monitoring)
– No prolonged recovery
– Safer
Gottlieb, Michael. Cosby, Karen. Ultrasound-guided hematoma block for distal radial and ulnar fractures. J Emerg Med. 2014 Dec 9.
Advantages:
– More effective than landmark approach
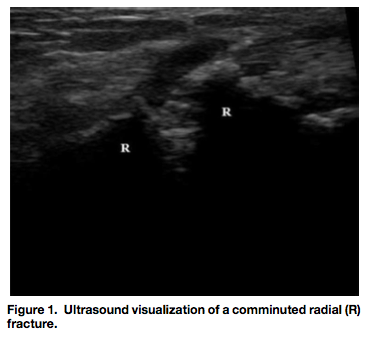
– Body habitus and soft tissue swelling can obscure step-off
– Step-off is otherwise hard to find in impacted and comminuted fractures
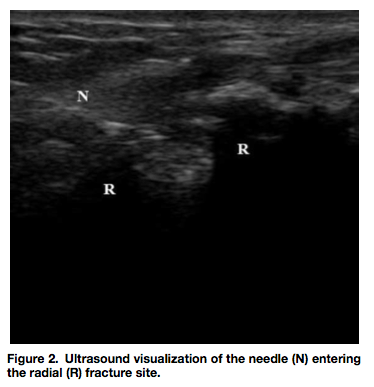
– Direct visualization of needle
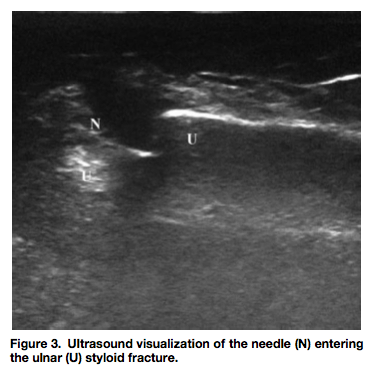
– Concomitant ulnar styloid fracture can interfere with reduction due to incomplete anesthesia of ulnar styloid site
How to Perform:
– Use linear transducer
– Trace bone longitudinally
– Note interruption in cortex

Myderrizi, N. Mema, B. The hematoma block: an effective alternative for fracture reduction in distal radius fractures. Med Arh. 2011;65(4):239-242.
Type of study: Double-blind, randomized clinical trial, n=96
Comparison: A) hematoma block (10 ml of 2% Lidocaine) versus B) general anesthesia (Propofol IV)
Results: Comparable pain during and after reduction. Significantly decreased time.
Contraindications: high bleeding risk, open or contaminated fractures
Taken in Elmhurst Hospital ED