Ultrasound-Guided Thoracentesis: a clinical case
By Stephen Alerhand MD
(Resident Physician, Icahn School of Medicine at Mount Sinai)
Edited by Alex Koyfman MD (@EMHighAK)
Featured on #FOAMED REVIEW 33RD EDITION – Thank you to Michael Macias from emCurious (@EMedCurious) for the shout out!
Presenting a Common ED Patient Conundrum
How often has a young female patient presented with the prospect of a CT scan expressed her reservations over the associated radiation and its “effect on her viable ovaries” or “ability to become pregnant”? This is a rhetorical question — it happens often. And frankly, it is a legitimate question for a patient to pose to her physician in taking ownership over her care. Every emergency physician has had this risks-and-benefits conversation with a female patient at one point or another, hopefully arriving at a decision together.
But what would you do (and what else in your toolbox would you access) if a young female patient threatened to “knock you out” if you exposed her to CT radiation for evaluating a suspected exudative pleural effusion? This happened to my colleagues and me during one shift in the pediatric emergency department. These are their stories (cue the Law-and-Order music).

History
21 year-old G1P1 female, admitted 1 week ago for a perforated appendix s/p abdominal drain, now presents to the pediatric ED with 3 days of new LUQ and L upper back pain. It is constant, worse with movement, not located at the site of her drain, with a quality difficult to describe. Her mother describes subjective fevers, nausea, and vomiting.
The patient’s vital signs are notable for a T 101 and O2 sat 94% on room air.
On exam, she is extremely uncomfortable due to the pain. There are decreased breath sounds on the L side. Physical exam is otherwise non-contributory.
Considering the recent perforated appendix with intra-abdominal contents requiring surgical drain placement, it was thought that this new pain could be 2/2 continued intra-abdominal infectious contents or even migration into a pleural effusion.
The Initial Ultrasound Application
My attending and I used bedside ultrasonography (details below), which demonstrated a significant L-sided pleural effusion. We debated draining the effusion right then and there. The Surgical consult told me that his team would need a CT scan to confirm our US-assessed pleural effusion while also delineating its margins for drainage.
The Present Dilemma
I brought these plans to the patient, and she erupted like a previously dormant volcano: “Not a chance in hell are you shooting my ovaries with more radiation.” I reassured her for a little while about the risks of CT radiation paling in comparison to the benefits of evaluating this new fluid collection. Nonetheless, she steadfastly refused and even threatened to “knock me out” if I insisted on going through with the CT.
The patient may have been only 21 years old, but her sweet Hello Kitty t-shirt and backpack belied the fierce warrior within. I did not feel like getting my butt kicked by a girl again, which left us with one other option available…
Ultrasound-Guided Thoracentesis with a Jerry-Rigged Apparatus
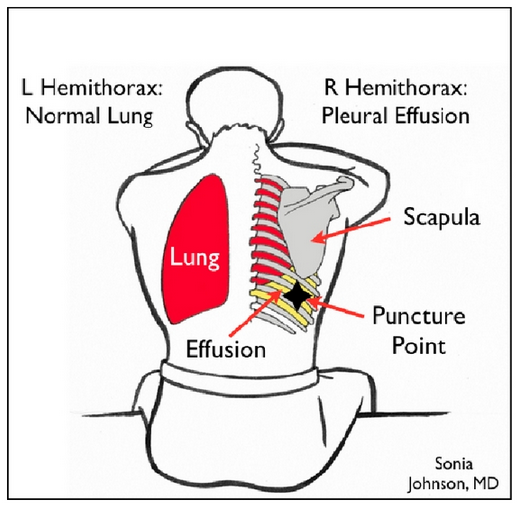
- Have patient sit upright. Visualize pleural effusion from posterior with linear probe. Mark the two ribs and interspace.

- To construct the apparatus, connect an 18-gauge needle to a large syringe. Connect the syringe to a 3-way stopcock. Connect the other end of the stopcock to tubing from a foley catheter drainage kit.
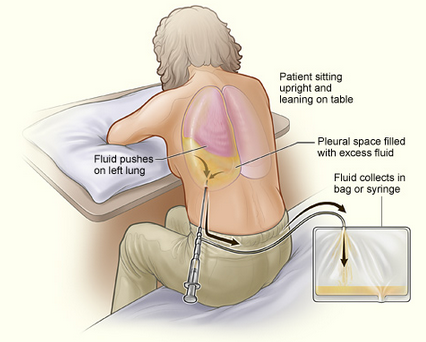
- Use centimeter markings on the ultrasound screen to determine the precise distance between skin and lung (from surface to visceral pleura). This way, the physician knows exactly how far he/she can insert the needle without risk of puncturing lung.
- Pull back on syringe to draw back pleural effusion contents.

- Adjust stopcock and push syringe contents into foley tubing toward drainage bag for collection/analysis.

- Repeat until pleural effusion almost completely drained.

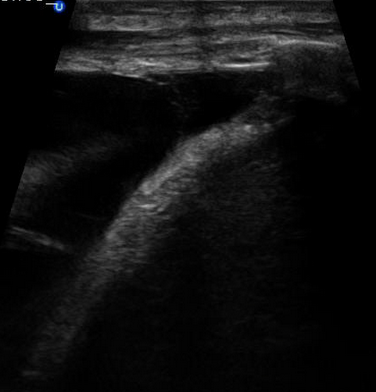
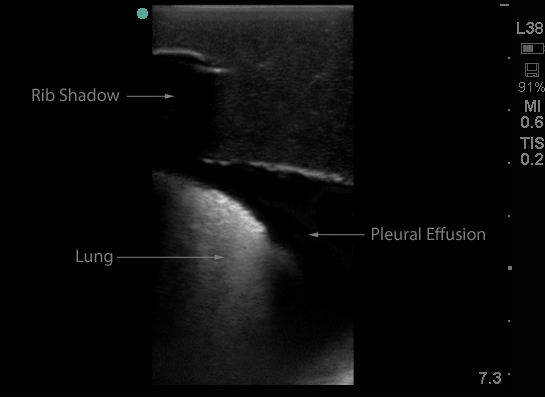
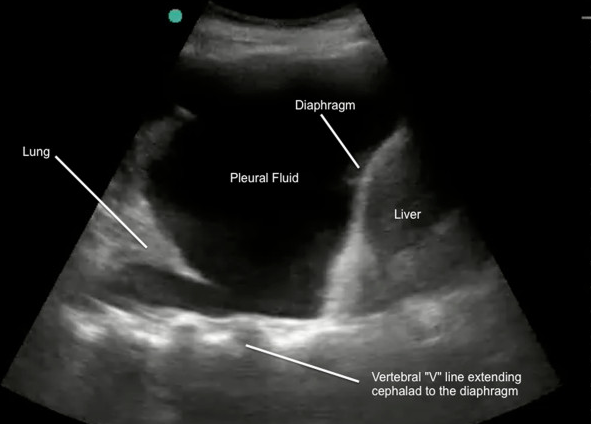
Just for fun, here is a FAST-view of a pleural effusion (as opposed to the views from posterior as above).
Back to the Story
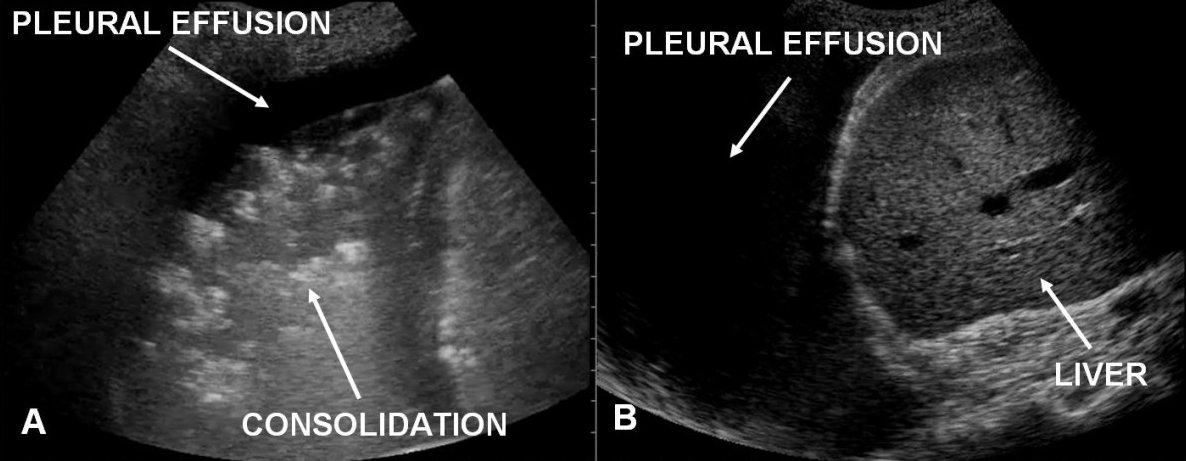
Almost 2 liters of pleural fluid were drained — initially serous, then serosanguineous, and then sanguineous. Drainage of pleural fluid ended up revealing an underlying pneumonia consolidation. The patient had already been started on broad-spectrum antibiotics and would stay in-hospital for another prolonged admission. Follow-up on the patient’s stay revealed that a CT scan had at some point been performed. No word on whether she knocked out the radiology technician exposing her to that radiation.
References/Further Reading
— Cavanna, L. Ultrasound guidance reduces pneumothorax rate and improves safety of thoracentesis in malignant pleural effusion: report on 445 consecutive patients with advanced cancer. World J Surg Oncol. 2014 May 2;12:139.
— Dawson, M. Mallin, M. Introduction to Bedside Ultrasound.
— Lobo, V. et al. Thoracic ultrasonography. Crit Care Clin. 2014 Jan;30(1):93-117.
— Perazzo, A. Can ultrasound guidance reduce the risk of pneumothorax following thoracentesis? J Bras Pneumol. 2014 Jan-Feb;40(1):6-12.
— Turner, JP. Dankoff, J. Thoracic ultrasound. Emerg Med Clin North Am. 2012 May;30(2):451-473.
— https://eresources.library.mssm.edu:3273/products/ejournals/html/10.1055/s-0034-1395794#N66540
— http://www.ncbi.nlm.nih.gov/pubmed/24786918
–– http://www.ncbi.nlm.nih.gov/pubmed/24606778





1 thought on “Ultrasound-Guided Thoracentesis”
Pingback: MANEJO DO DERRAME PLEURAL NO DEPARTAMENTO DE EMERGÊNCIA(DE) – Emergência Rules