Author: Anthony DeVivo, DO (@anthony_devivo, EM Resident Physician, Mount Sinai St. Luke’s-West) // Edited by: Alex Koyfman, MD (@EMHighAK); Brit Long, MD (@long_brit); and Manpreet Singh, MD (@MprizzleER)
Welcome back to Unlocking Common ED Procedures! Today, we look at tube thoracostomy.

Check out our new downloadable procedure card with QR code link to the article. Print them out and be ready to go over it with your learners!
Case
A 19-year-old male with no past medical history presents to the ED for sudden onset chest pain and shortness of breath which has progressively worsened over the past 24 hours. He denies trauma, infectious symptoms, or ever having any similar pain in the past. He has no history of recent travel, lower extremity swelling, or syncope. On exam, he is nontoxic appearing, but is in mild respiratory distress with a respiratory rate of 24, a blood pressure of 110/60, and an oxygen saturation of 91% on room air. He also has notable discomfort upon deep inspiration. Upon auscultation of the posterior chest, he is noted to have markedly decreased breath sounds on the left in comparison to the right. There is no jugular vein distention or obvious tracheal deviation. A chest x-ray is ordered and is below:

What is your next step for this patient? Does he need an emergent needle thoracostomy? Will he require a 40Fr thoracostomy tube? Perhaps something smaller would suffice? What about a pigtail catheter? Why not just leave him on supplemental oxygenation and repeat the chest x-ray? All this and more will be discussed below with emphasis on the evidence behind procedure site preference and tube size, as well as troubleshooting chest tube complications, should they arise.
Placement of a thoracostomy tube, more frequently referred to as a chest tube in the ED, is one of the most common invasive surgical procedures performed by emergency physicians. While this classic procedure has undergone several stages of evolution over the years, its principle is still centered around the placement of a tube or catheter within the pleural cavity with the intent of draining either air or fluid that has collected within the intrapleural space.1 The collection of air or fluid between the parietal and visceral pleura can lead to significant restriction of lung compliance, leading to decreased ventilation, increased work of breathing, and hypoxia.2-3 If left without intervention, the pressure within the pleural space can lead to compression of the lung parenchyma, mediastinal shift, and compression of the great vessels, causing hemodynamic compromise, also known as a tension pneumothorax.3 Hence, chest tube placement is a procedure that emergency physicians should be comfortable performing and managing potential complications.
Indications:3-5
- Pneumothorax
- Spontaneous
- Traumatic
- Malignant
- Iatrogenic
- Hemothorax
- Pleural Effusion
- Malignant Effusion
- Empyema/Abscess
Contraindications:
As it is often an emergent, life-saving procedure, there are no absolute contraindications. However, there are certainly circumstances in which a patient has a clear indication for the placement of a chest tube, but is hemodynamically stable or even asymptomatic. In these situations, there may be time to assess the patient for several relative contraindications and possibly mitigate the risk of complications by choosing a different method or procedure site.
-
Signs of overlying infection at the procedure site
- While the placement of a chest tube in the ED is generally an emergent procedure, it is preferable to avoid placement through any region of cellulitis due to concern for seeding infection into the pleural space. Even under ideal conditions, rates of infection and empyema formation secondary to tube thoracostomy ranges between 1-25%.6-8 Thus, any means of mitigating this would be best for the patient.
-
Coagulopathy
- There is no literature to support that any specific degree of coagulopathy or anticoagulant medication use places patients at a higher risk for postprocedural bleeding.9-10 One study assessed a population of patients with mild coagulopathy requiring chest tube placement and compared the rates of bleeding with and without prophylactic FFP administration and found no significant difference.11 This is an isolated study, and there is need for more evidence to appropriately assess bleeding risk in the setting of varying degrees of coagulopathy. In addition, the British Thoracic Society recommends non-urgent chest tube placement be delayed if INR > 1.5.12 However, coagulopathy and anticoagulation should not delay the placement of a chest tube if emergently indicated.
-
Pleural Adhesions
- Pleural adhesions are a consequence of prior chest tube placement, thoracic surgery, or infection. These adhesions can complicate chest tube placement by distorting anatomy and obstructing tube insertion. It can also potentially increase the risk of lung parenchymal injury. Pleural adhesions can be explored during the procedure by a finger sweep of the pleural space prior to tube placement, as will be discussed later in this article. If there is concern for pleural adhesions, it can also be explored prior to the procedure with CT of the chest depending upon urgency of placement.3,6-7
Technique
Conventional Tube Thoracostomy
The placement of a conventional chest tube is a surgical procedure, which involves making an incision through the chest wall into the pleural space and placement of a tube in order to facilitate air and/or fluid drainage.
Pigtail Catheter
The placement of a pigtail catheter, generally of 14Fr or smaller, involves the use of the Seldinger technique during which a needle is placed into the intrapleural space, followed by a guidewire over which a curved tip catheter is ultimately inserted into the space. The overall procedure is similar to the placement of a central venous catheter, given the same technique is being utilized.
Both of these techniques will be discussed in detail below.
Size
Thoracostomy tubes are available in a wide range of sizes, and their diameter is most commonly described in the French (Fr) measurement scale. The conversion of the diameter of a 14 Fr tube is equivalent to 0.33 mm. The classification of chest tube sizing is poorly defined with no formal consensus on the definition of small, medium, and large-bore chest tubes. While some literature and academic societies support three sizing classifications, others define only small and large-bore sizing. A study published in the Journal of Trauma and Acute Care Surgery defined small-bore chest tubes as 28-32Fr and large-bore as > 32Fr.13 For comparison, below is one of the classifications utilized by the American College of Chest Physicians (CHEST).14
- Small-bore: 7-14 Fr
- Moderate: 16-22 Fr
- Large-bore: > 24 Fr
Choosing the Right Tube and Technique For The Job
The technique and size chosen for pleural cavity drainage is traditionally based on the specific indication for chest tube placement.13-14 Since the rate of drainage or fluid flow from the intrapleural cavity to the drainage system is based partially on luminal diameter, larger tubes are chosen for viscous fluid drainage, while smaller diameter tubes are utilized for the removal of air in the setting of an uncomplicated pneumothorax.3,13-16 However, there is substantial recent literature supporting the use of smaller diameter chest tubes for both pneumo and hemothoraces. In addition, literature now supports the use of small-bore pigtail catheters in place of traditional chest tubes in certain clinical circumstances, as will be discussed below.
-
Primary Pneumothorax
- In the setting of an uncomplicated primary pneumothorax with no evidence of pleural fluid collection, regardless of size, a small-moderate bore chest tube ranging from 16-22Fr is indicated. In addition, recent literature, as well as the American College of Chest Physicians, support the use of small-bore catheters such as pigtail catheters of sizes <14Fr.14 In fact, one retrospective follow-up study showed that primary spontaneous pneumothoraces managed with surgical chest tubes had longer chest tube durations when compared to those managed with small-bore pleural catheters.15
- Patients who have recurrent primary pneumothoraces, in whom there is concern for pleural adhesions, multiple previous thoracostomy tube placements, bronchopleural fistulas, or the development of pleural fluid, a moderate-sized surgical chest tube ranging from 24-28Fr should be considered in order to avoid tube lumen obstruction.15
- In the setting of questionable or clear hemodynamic compromise secondary to a pneumothorax, small-bore catheters may be utilized, as this will not affect duration or complexity of drainage and resolution. However, clinical gestalt should be utilized in assessing the degree of instability and to determine what method of intervention will be the safest and most expeditious for the physician performing the procedure.15
-
Secondary Pneumothorax
- Traumatic secondary pneumothoraces have also traditionally been managed with conventional, moderate-large bore chest tubes. However, similar to primary pneumothoraces, recent literature has provided the emergency medicine and surgical communities with evidence for the use of small-bore chest tubes and catheters in the appropriate clinical setting.16-18 Patients with traumatic pneumothoraces without evidence of effusion on imaging can be effectively managed with small-bore traditional tubes or <14Fr catheters.17,18 In the setting of a traumatic pneumothorax with signs of an effusion, there is some literature to suggest that there is no clinical difference between small-bore catheters and traditional moderate-large bore chest tubes.19 However, this is not yet a universally accepted practice and should be discussed with the surgical or trauma service who may be managing the patient upon admission.
- Iatrogenic pneumothoraces without evidence of a hemothorax or other complicating factors previously discussed may be managed similarly to spontaneous pneumothoraces with small-bore catheters.
-
Hemothorax
- Traditionally, hemothoraces are managed with large-bore chest tubes ranging from 36-40Fr in order to appropriately facilitate fluid drainage while avoiding luminal obstruction. However, recent literature has progressed to the use of smaller diameter chest tubes for hemothorax management. A recent prospective observational study at a level 1 trauma center assessing hemothorax drainage using large (36-40Fr) vs small (28-32Fr) chest tubes concluded that there was no statistically significant difference in efficacy of drainage or rate of complications.13 Another study took this a step further, comparing hemothorax drainage using 20-22Fr chest tubes versus 28Fr chest tube, and again showed no difference in efficacy of drainage.20 While current literature supports the utilization of smaller diameter chest tubes for traumatic hemothorax drainage, the American College of Surgeons currently endorses the use of 28-32Fr chest tubes.21 In addition, multiple trials have now begun to assess the use of small-bore pigtail catheters as small as 14Fr for the drainage of traumatic hemothoraces with outcomes supporting no clinical difference in drainage and complication rates.22-23 However, the data on the use of small-bore pigtail catheters are still limited and not yet the standard of care. At this point in time, hemodynamically unstable patients in the setting of a hemothorax should be managed with an emergent large-bore chest tube of 28-32Fr, as per ATLS guidelines. The management of hemodynamically stable traumatic hemothoraces should be a joint discussion between the Emergency Physicians and surgical team that will be managing the patient, as there is literature to support the use of smaller diameter and even pigtail catheters for management.
Anatomy
Regardless of whether a chest tube or pigtail catheter is being placed, there are multiple anatomical structures to consider during placement to avoid complications and adverse injuries. A chest tube or catheter should generally be placed at or just above the 5th intercostal space in the midaxillary line in order to avoid damaging the diaphragm, liver, or spleen inferiorly, as well as the axillary vascular structures superiorly. In addition, placement in the mid-axillary region is the thinnest area of muscle and allows for avoidance of the breast parenchyma, as well as large muscles such as the pectoralis major.1,3-7 A simplified way to recall the ideal procedure site is the “ triangle of safety”, formed anteriorly by the lateral border of pectoralis major, posteriorly by the lateral border of the latissimus dorsi, and inferiorly by the 5th intercostal space, which is commonly identified at the level of the nipple. Once the intercostal space is chosen, there is additional anatomy to be taken into consideration, as there is a neurovascular bundle along the inferior border of each rib. The procedure should be performed along the superior aspect of the rib within the intercostal space of choice.

The Procedure – Chest Tube
The following procedure review is meant for a patient who is relatively hemodynamically stable and not in extremis. If the indication for a chest tube is significantly affecting the patient’s hemodynamics, a more expedited placement may be necessitated.
-
Positioning
- Whether the patient is awake, sedated, or intubated, positioning is vital to the proper placement of a chest tube both in terms of the appropriate anatomical location as well as the directionality and position of the tube within the pleural cavity. The patient should be lying supine with the ipsilateral arm flexed and abducted above or behind the patient’s head.
- The anatomical site should then be chosen and marked with a marking pen.
- Of note, the procedure laterality should be checked and rechecked with the diagnostic imaging modality that has provided the diagnosis to assure the procedure is being performed on the correct side.
-
Preparation
- Discuss the procedure with the nurses and/or techs for appropriate set up and preparation of the drainage system. Prepare a sterile area on a table or mayo stand where your supplies, cleansing materials, drape, gown, and sterile gloves are set aside. The end of the drainage system that will connect to the chest tube should be maintained sterilely. Depending on the institution, it may be the physician’s responsibility to organize the drainage system as well.
- Using chlorhexidine or betadine, sterilize the procedure site previously identified. It is advisable to prepare a large sterile area for the procedure to allow for sterile space to maneuver.
- Drape the patient in sterile manner with landmarks and demarcated procedure site clearly visibly. At this point, the proceduralist should be sterile in cap, mask, gown, and gloves.
- This is a painful procedure. Local anesthetic is advised if possible. While local anesthetic is often adequate pain control for this procedure, additional intravenous medications for pain control may be necessary. As this procedure is performed in close proximity to multiple vital anatomic structures, patient comfort and cooperation is vital to its success. As such, adequate pain control should be maintained throughout the procedure.
-
Procedure
- Using a small gauge needle with 1% or 2% lidocaine with epinephrine, make a superficial wheel of anesthetic at the entry site followed by insertion of the needle into the deep tissues down to the rib, including the periosteum of the rib. Be sure to draw back before introducing anesthetic.
- Premeasure the chest tube from the intended incision site to the ipsilateral clavicle to estimate how deep to advance the chest tube within the pleural cavity.
- If performing this procedure without an assistant, it is important to prepare the chest tube before beginning the procedure by clamping the distal end to avoid a rush of fluid from the pleural space. A curved clamp can also be applied to the proximal end in preparation for guiding the tube through the incision into the pleural space.
- Using a #11 blade, make a 3-4 cm incision along the superior aspect of the inferior rib of the intended intercostal space. This space should be large enough so that it is suitable for both the proceduralist’s finger and the chest tube. This is so the tube may be more easily guided into the pleural cavity at the appropriate direction as well as to ensure the tract is not lost while attempting to insert the tube. While there may be some apprehension in making too large an incision, the procedure requires appropriate room to maneuver in order to safely and effectively place the tube. The incision can be easily sutured once the tube is successfully placed.
- Once the incision has been made, a curved/Kelly clamp may be utilized to bluntly dissect through the subcutaneous tissues, while intermittently opening the clamp to assure the space within the tissues beneath the incision is adequate for the remainder of the procedure. Continue this until the intercostal space and inferior rib can be palpated.
- Using a finger along the curved edge of the clamp, guide the tip of the clamp over the superior border of the inferior rib and puncture through into the pleural space. Depending on the indication for the chest tube placement, a rush of fluid or air may flow out of the pleural space upon entry.
- As done with the subcutaneous tissues, spread the opening into the pleural space by opening the curved clamp within the initial puncture site so that both a finger and the tube may enter simultaneously.
- Place a finger into the space and sweep 360 degrees along the inner aspect of the chest wall to assure no adhesions are present. The lung may or may not be palpable at this point.
- Do not remove the curved clamp before inserting a finger into the tract within the pleural space, or the tract may be lost.
- If the chest tube is not yet clamped proximally, grab the proximal end of the chest tube with the curved clamp and guide the tube into the pleural cavity along with the finger that is maintaining the location and patency of the tract. Advance the tube until, at minimum, all tube fenestrations have entered the pleural space. The directionality of the tube insertion is traditionally dependent on the indication for the chest tube.
- If the chest tube is being placed for a pneumothorax, it should be directed anteriorly and towards the apex.
- If the chest tube is being placed for a fluid collection, whether infectious or bloody, direct the tube posteriorly.
- While not evidence based, for patients in whom there is concern for difficulty in chest tube insertion such as due to obesity, a bougie may be utilized to guide placement. The bougie can be used in a similar fashion for chest tube placement as it is for ET tube placement. Once the pleural cavity is punctured, a finger should remain within the space in order to avoid losing the tract, and the bougie may be inserted into the pleural space at the appropriate directionality. Once within the pleural space, the chest tube may be inserted over the bougie. The thought process behind this method is that since the bougie is semi-rigid, it may facilitate tube insertion through large amounts of subcutaneous tissue and possibly avoid subcutaneous placement of the chest tube. Caution should be taken as to not insert the bougie to deeply leading to pulmonary or mediastinal injury. This risk may be mitigated by measuring the bougie against the chest wall to approximate depth on insertion. While this method of insertion is certainly the standard, it may have a place in assisting with the placement of difficult chest tubes.
- Once the chest tube has been successfully advanced into the pleural cavity, attach the distal end of the tube to the drainage system and release the clamp occluding the distal aspect of the chest tube.
- Using a 0 or 1-0 Nylon or Silk stitch, secure the chest tube to the skin by placing a simple interrupted suture above the tube insertion site, anchoring it to the skin, wrapping it around the tube multiple times, and then tying it off. You can repeat this again with an anchor suture below the chest tube as well to help prevent accidental dislodgement.
- If there is a significant gap between the chest tube and the end of the incision site, this may also be closed with the same size and type of suture using a simple interrupted stitch.
- Be sure the suture sites are adequately anesthetized before placement. If not, inject additional lidocaine.
- Apply a dry, occlusive dressing.
- Take 3 layers of 4×4 gauze, cut a line through them to the midpoint, and insert them over the chest tube so that the tube lies within the middle of the gauze. You may choose to apply petroleum gauze directly to the where the tube rests on the skin prior to 4×4 occlusive dressing.
- Using 3-4 inch adhesive tape or tegaderm adhesive dressings, seal each corner of the gauze.
- Once the occlusive dressing is applied, you may further utilize either adhesive tape or tegaderm to secure the more distal tubing to the anterolateral chest wall and flank. The adhesive tape or tegaderm should be applied horizontally across the tubing as it runs down the chest wall.
- Auscultate the bilateral anterior and posterior lung fields for appropriate, equal breath sounds.
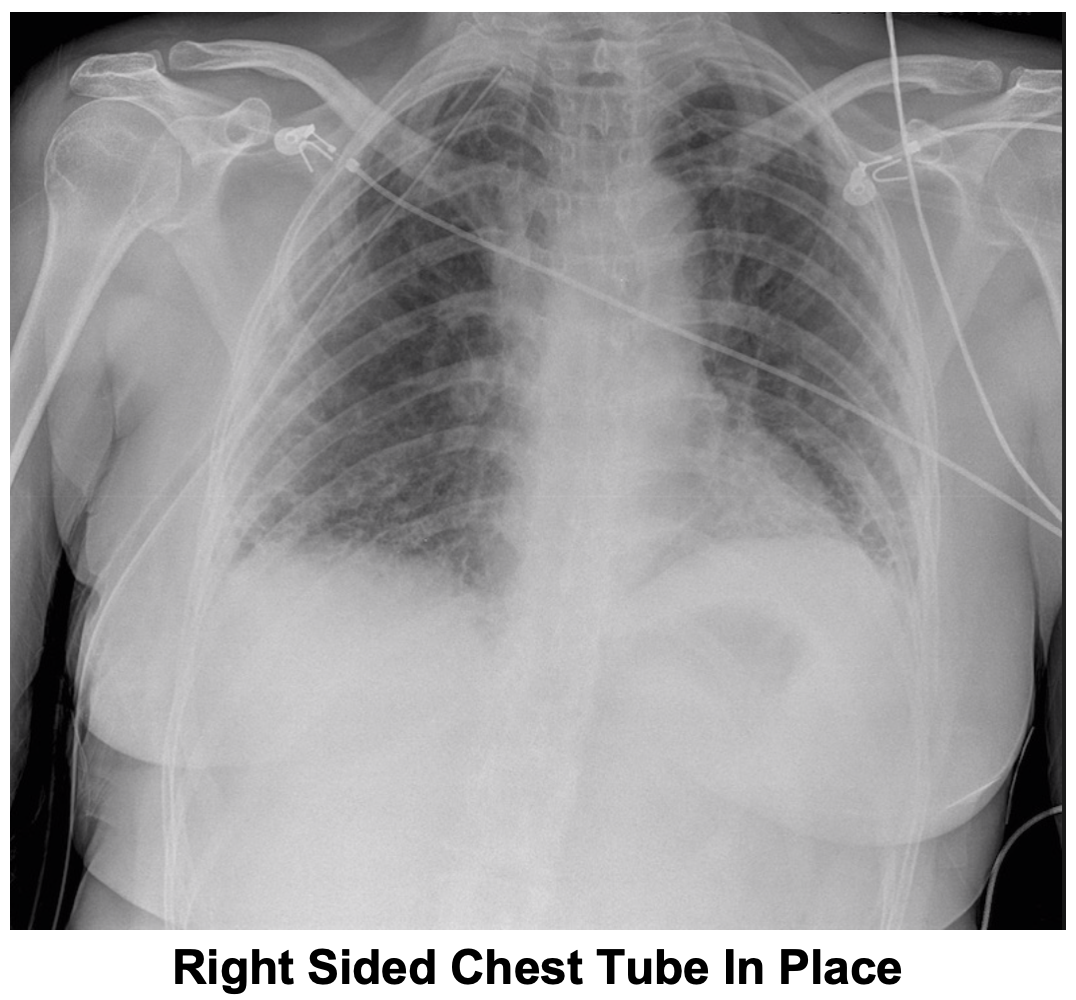
- Obtain a post-procedure chest x-ray to confirm appropriate placement and assess improvement of the indication for which the chest tube was placed.

The Procedure – Pigtail Catheter
Indications for the placement of a pigtail, or curved end catheter, are discussed above. The positioning and preparation for the placement of a pleural catheter such as a pigtail catheter are the same as a conventional chest tube. The stepwise review of the placement of a pigtail catheter will be the same until the procedure portion. While preparing for the procedure, the suction system should be assessed to assure it is compatible with a pigtail or small-bore chest tube. This is generally not an issue, but some suction systems require adapters for different chest tube sizes.
-
Procedure
- Using a small gauge needle with 1% or 2% lidocaine with epinephrine, make a superficial wheel of anesthetic at the entry site followed by insertion of the needle into the deep tissues down to the rib, including the periosteum of the rib. Be sure to draw back before introducing anesthetic.
- Using an introducer needle attached to a 5 cc syringe, insert the needle into the anesthetized area directed just superior to the superior margin of the inferior rib of the desired intercostal space. Aspirate until air or fluid can be obtained. To assist in assessing whether air can be aspirated, the syringe can contain a small amount of sterile water or normal saline so that bubbles can be visualized upon aspiration of air.
- Once air or fluid is readily aspirated the syringe can be removed while being sure not to dislodge the introducer needle from the pleural space.
- Insert the guidewire into the pleural space. If resistance is met, withdraw the guidewire, reattach the syringe, and aspirate to reconfirm the needle is within the pleural space.
- Direct the guidewire superior and towards the apex for a pneumothorax.
- Direct the guidewire inferior and posteriorly for a fluid collection.
- Once the guidewire has been inserted, remove the introducer needle and make a small incision at the guidewire site of entry so that the dilator and pigtail catheter may pass.
- Insert the dilator enough to dilate the tract.
- Some kits may have a dilator/chest tube apparatus in one piece or may have a separate dilator. It is always advantageous to be familiar with the specific kits stocked at your institution.
- If the dilator is separate, remove the dilator from the guidewire and insert the chest tube over the wire. Be sure the chest tube is adequately positioning with all the fenestrations with the pleural cavity before removing the guidewire.
- Attached the distal end of the pigtail catheter to the suction system.
- In a similar manner as described above, secure the pigtail catheter via suture and apply a dressing. Some pigtail catheter kits may come with a specific tube holder and securing device. If this is not available, simply suture the catheter to the anterior chest wall in a similar manner to the method discussed previously for a traditional chest tube.
- Obtain chest x-ray to confirm pigtail catheter placement.
Chest Tube Drainage System Review1-3,24
There are multiple types of chest tube drainage systems available once a thoracostomy tube is appropriately placed. One of the most commonly utilized mechanisms for drainage within the emergency department is the three compartment system. This system involves the utilization of three chambers in sequence to allow for drainage while creating a one-way system so that air or fluid does not reenter the pleural space. The purpose of the first chamber is collection of either fluid or air from the pleural space. The water-seal chamber follows the collecting chamber in sequence and contains 2 cm of water that acts as a one-way valve to create a closed system that prevents air or fluid moving back into the pleural space. The suction chamber is the final in sequence and utilizes either a wet or dry suction apparatus. The wet suction mechanism is commonly seen in the ED, and the baseline suction pressure is based on the amount of water within the column. This column is generally filled with enough water to start at -20 mm H2O of suction. This drainage system can be left on a strict water-seal or it can be hooked up to wall suction for added force. In addition to the wet-seal 3 chamber drainage system, there are now also dry seal systems available, which use a suction apparatus within the third chamber instead of water to set the degree of suction desired.
Post-procedural Complications26-28
-
Chest Tube Malposition
- One of the most common complications of chest tube placement is inappropriate positioning. If the malposition is isolated to the tube’s directionality not being ideal for treatment of the underlying condition but it is appropriately draining, the position should be discussed with the team who will be managing the patient upon admission. It is important to remember that the tube cannot be removed and reinserted into the chest cavity, as it is no longer sterile and can potentially seed infection. Thus, significant alteration in a chest tube’s directionality post-placement may require complete removal and reinsertion of a new tube.
- Malpositioning of a chest tube can be more complicated if the initial insertion of the tube is not within the pleural space. Instead, the tube may end up within the subcutaneous tissue of the anterolateral chest wall, within the lung parenchyma, or in the intrafissural space. In the case of subcutaneous placement, the malposition will likely be visualized on chest x-ray. In addition, the suction system is unlikely to function upon insertion. If this occurs, the tube should be removed and replaced immediately. Risk factors for subcutaneous placement include thoracic trauma and multiple rib fractures, which can distort the anatomy.28
- Malpositioning of the tube within the pleural cavity can involve the tube residing within the lung parenchyma or the intrafissural space. These malpositions can be identified on x-ray or CT of the chest. If the chest tube is functioning appropriately and the patient is hemodynamically stable, the chest tube should be left in place and should be discussed with the surgical service before attempting removal.
-
Obstruction
- When using a 3-chamber collecting system, the water-seal chamber may be utilized to assess for both obstruction as well as an air leak. The water-seal chamber should fluctuate with respiration and coughing while the drainage system is set to gravity alone. If this does not occur, the lumen of the tube may be occluded or the lung has completely re-expanded.
- Chest tube lumen occlusion due to buildup of viscous materials or blood clot has been shown to often self-resolve. While the methods of chest tube stripping or milking have traditionally been utilized to assist in maintaining lumen patency, there is no evidence supporting its efficacy and can be potentially harmful as these methods can lead to sudden increases in negative pressure within the pleural cavity.
-
Air leak
- An air leak implies the presence of air within the pleural space. An air leak can be expected upon initial insertion of a chest tube, particularly with an actively resolving pneumothorax. However, a new or persistent air leak can be concerning and should be further investigated. This is more pertinent to the inpatient team that will be managing the chest tube long term, but as patients sometimes spend prolonged time periods in the emergency department, it is important to be aware of this issue.
- In addition to assessment of luminal obstruction, the water-seal chamber can also assist in identifying an air leak as persistent or constant bubbling within this chamber. Assuming the water-seal is functioning appropriately, there are several concerns that arise when a new or persistent air leak becomes apparent. The problem may be within the pleural cavity such as the formation of a new pneumothorax or an air leak due to bronchopulmonary injury or fistula formation. The leak may also be due to air entering through the insertion wound from outside the pleural cavity, such as in the instance of the chest tube insertion site being inadequately closed or bandaged leading to air entering the pleural cavity outside the closed system to which the tube is attached. If there is a persistent air leak post tube placement, the post-procedural chest x-ray should be reviewed to assure adequate placement. The incision site as well as the bandage should also be reassessed to ensure no air is re-entering the pleural cavity.
-
Subcutaneous Emphysema
- The development of post-procedural subcutaneous emphysema can be detected by crepitus on physical exam, as well as on chest x-ray. When this finding is evident either on exam or imaging, it is vital to assure the chest tube is within the pleural cavity and not the subcutaneous space. As long as the chest tube is appropriately positioned, subcutaneous emphysema is self-limited and should not lead to any further complication.
-
Lung Injury
- During the placement of a chest tube, it is possible that the lung may be injured leading to a pulmonary laceration, which may not become evident until long after the tube is placed, sometimes not even until it is removed. This can acutely lead to persistent bleeding and, long term, may cause the formation of a bronchopleural fistula. The post-procedural chest x-ray should be reviewed to assure the tube is not within the lung parenchyma and that a new effusion that may have resulted from a pulmonary laceration is not present. If there is concern for pulmonary injury, immediate discussion with cardiothoracic surgery should occur.
-
Reexpansion Pulmonary Edema
- Reexpansion pulmonary edema occurs when a large pneumothorax, hemothorax, or pleural effusion, either acute or chronic, leads to rapid re-expansion of the lung, which can cause the development of pulmonary edema. The pathophysiologic mechanism of this is not well understood, but is thought to be the consequence of an acute inflammatory response leading to increasing permeability of the alveolar-capillary membrane, thus causing the rapid development of pulmonary edema. There is not strong evidence for any particular means by which this adverse effect can be avoided, but the American College of Chest Physicians does not recommend more than 1L of fluid be drained from the pleural space before ceasing drainage. Additional studies are required for more evidence-based guidelines on how to avoid this rare but dangerous complication, which holds a mortality rate as high as 20%.28
-
Infection29-31
- The placement of a chest tube is an invasive procedure that can potentially introduce bacteria into the skin, deep tissue of the anterior chest wall, or thoracic cavity. The introduction of bacteria into these spaces can lead to cellulitis, chest wall abscesses, pneumonia, or empyema. The use of prophylactic antibiotics is a long standing point of contention among physicians. However, a large systematic review and meta-analysis assessing 12 randomized trials that sought to establish the utility of antibiotics in blunt and penetrating thoracic trauma concluded that prophylactic antibiotics reduce the risk of pneumonia and empyema development.31
Pearls and Pitfalls
- Recheck landmarks prior to beginning the procedure. The landmarks discussed above provide a margin of safety to avoid vascular, diaphragmatic, or intraperitoneal injury during tube placement. It is far easier to double check prior to insertion than it is to manage the repercussions of these injuries.
- In the setting of an awake, hemodynamically stable patient, consider both local and intravenous pain medication. This can be an uncomfortable and anxiety provoking procedure for the patient, and it is imperative for patient safety that he/she does not move during tube placement.
- When anticipating large fluid expulsion after tube placement, be sure to have the distal lumen of the chest tube clamped initially. Once the tube is successfully inserted, attached the distal portion of the tube to the drainage system and unclamp the tube.
- Prolonged clamping or luminal obstruction of a chest tube can lead to the formation of a tension pneumothorax and rapid hemodynamic collapse.
- Be sure to close the insertion site and carefully apply an occlusive dressing to avoid an air leak.
- Prophylactic antibiotics reduce the risk of empyema and pneumonia development in penetrating and blunt thoracic trauma requiring chest tube placement.
Rapid Procedure Guide – Tube Thoracostomy
- Set up chest tube drainage system.
- Position thepatient supine with the upper extremity of the side of the procedure flexed and abducted over the head.
- Assess landmarks and demarcate the procedure site at the 4th or 5th intercostal space in the mid-axillary line.
- Sterilely prepare procedure site.
- Anesthetize from the skin through the subcutaneous tissue and down to the periosteum of interior rib of the intercostal space that the chest tube will be placed.
- Using a #11 blade, make a 2-3 cm incision at the inferior border of the intercostal space so that the chest tube will enter the space over the superior border of the rib below the intercostal space.
- Using a curved or Kelly clamp, dissect through the subcutaneous tissue down to the superior border of the rib.
- Using the closed, blunt tip of the Kelly clamp, puncture through the pleura over the superior border of the rib and open the clamp to widen the space.
- Insert your index finger into the space to assure you are within the pleural cavity and sweep 306 degrees to assess for adhesions.
- Using the Kelly clamp, grasp the proximal end of the chest tube which has already clamped at the distal end and insert into pleural space using the finger which is still in the pleural space to guide insertion. The directionality of insertion will depend on the indication of the tube.
- Attach the distal end of the chest tube to the sterile end of the drainage system and unclamp tube.
- Secure chest tube, suture insertion site as necessary, and apply occlusive dressing.
- Obtain post-procedural chest x-ray.
Rapid Procedure Review – Pigtail Catheter
- Set up chest tube drainage system.
- Position thepatient supine with the upper extremity of the side of the procedure flexed and abducted over the head.
- Assess landmarks and demarcate the procedure site at the 4th or 5th intercostal space in the mid-axillary line.
- Sterilely prepare procedure site.
- Anesthetize from the skin through the subcutaneous tissue and down to the periosteum of interior rib of the intercostal space that the chest tube will be placed within.
- Insert the 18 gauge introducer needle into the anesthetized skin at the inferior border of the intercostal space that the chest tube will be placed within and aspirate until fluid or air can be returned.
- Leaving the needle in place, remove the syringe and advance the guidewire into the pleural space.
- Hold the guidewire in place and withdraw the needle over the wire.
- Using a #11 blade, make a small nick at the guidewire insertion site.
- Pass the dilator over the wire and dilate the catheter tract.
- Advance to pigtail catheter over the guidewire until it is at least 2 cm after the last hole is within the pleural cavity.
- Connect the catheter to the drainage system.
- Secure catheter and apply occlusive dressing.
- Obtain post-procedural chest x-ray.
References/Further Reading:
- Tintinalli, Judith E., et al. Tintinalli’s Emergency Medicine: a Comprehensive Study Guide. McGraw-Hill Education, 2016.
- Marino, Paul L. Marino’s the ICU Book. Wolters Kluwer Health, 2014.
- Parrillo, Joseph E. Critical Care Medicine: Principles of Diagnosis and Management in the Adult. Elsevier, 2019.
- Gilbert, Timothy B., et al. “Chest Tubes: Indications, Placement, Management, and Complications.” Journal of Intensive Care Medicine, vol. 8, no. 2, 1993, pp. 73–86., doi:10.1177/088506669300800203.
- Baumann, Michael H. “What Size Chest Tube? What Drainage System Is Ideal? And Other Chest Tube Management Questions.” Current Opinion in Pulmonary Medicine, vol. 9, no. 4, 2003, pp. 276–281., doi:10.1097/00063198-200307000-00006.
- Kuhajda, Ivan, et al. “Tube Thoracostomy; Chest Tube Implantation and Follow Up.” Journal of Thoracic Disease,6 Oct. 2014, doi:10.3978/j.issn.2072-1439.2014.09.23.
- Stawicki, Stanislaw P., et al. “Thoracostomy Tubes: A Comprehensive Review of Complications and Related Topics.” International Journal of Critical Illness and Injury Science, vol. 4, no. 2, 2014, p. 142., doi:10.4103/2229-5151.134182.
- Maxwell, Robert A., et al. “Use of Presumptive Antibiotics Following Tube Thoracostomy for Traumatic Hemopneumothorax in the Prevention of Empyema and Pneumonia—A Multi-Center Trial.” The Journal of Trauma: Injury, Infection, and Critical Care, vol. 57, no. 4, 2004, pp. 742–749., doi:10.1097/01.ta.0000147481.42186.42.
- Pathak, Vikas, et al. “Management of Anticoagulant and Antiplatelet Therapy in Patients Undergoing Interventional Pulmonary Procedures.” European Respiratory Review, vol. 26, no. 145, 2017, p. 170020., doi:10.1183/16000617.0020-2017.
- Davidson, Bruce L. “Reducing Procedural Hemorrhage Risk.” Chest, vol. 150, no. 6, 2016, p. 1421., doi:10.1016/j.chest.2016.10.033.
- Müller, Marcella C., et al. “Transfusion of Fresh-Frozen Plasma in Critically Ill Patients with a Coagulopathy before Invasive Procedures: a Randomized Clinical Trial (CME).” Transfusion, vol. 55, no. 1, 2014, pp. 26–35., doi:10.1111/trf.12750.
- Havelock, T., et al. “Pleural Procedures and Thoracic Ultrasound: British Thoracic Society Pleural Disease Guideline 2010.” Thorax, vol. 65, no. Suppl 2, 2010, pp. i61–i76., doi:10.1136/thx.2010.137026.
- Inaba, Kenji, et al. “Does Size Matter? A Prospective Analysis of 28–32 versus 36–40 French Chest Tube Size in Trauma.” The Journal of Trauma and Acute Care Surgery, vol. 72, no. 2, 2012, pp. 422–427., doi:10.1097/ta.0b013e3182452444.
- Djenfi, Tarek, et al. “Management of Spontaneous Pneumothorax.” Chest, vol. 148, no. 4, 2015, doi:10.1378/chest.2280584.
- Riber, Sara S., et al. “The Influence of Chest Tube Size and Position in Primary Spontaneous Pneumothorax.” Journal of Thoracic Disease, vol. 9, no. 2, 2017, pp. 327–332., doi:10.21037/jtd.2017.02.18.
- Cooke, David T., and Elizabeth A. David. “Large-Bore and Small-Bore Chest Tubes.” Thoracic Surgery Clinics, vol. 23, no. 1, 2013, pp. 17–24., doi:10.1016/j.thorsurg.2012.10.006.
- Tsai, Wen-Kai, et al. “Pigtail Catheters vs Large-Bore Chest Tubes for Management of Secondary Spontaneous Pneumothoraces in Adults.” The American Journal of Emergency Medicine, vol. 24, no. 7, 2006, pp. 795–800., doi:10.1016/j.ajem.2006.04.006.
- Kulvatunyou, N., et al. “Randomized Clinical Trial of Pigtail Catheter versus Chest Tube in Injured Patients with Uncomplicated Traumatic Pneumothorax.” British Journal of Surgery, vol. 101, no. 2, 2013, pp. 17–22., doi:10.1002/bjs.9377.
- Kulvatunyou, Narong, et al. “14 French Pigtail Catheters Placed by Surgeons to Drain Blood on Trauma Patients.” Journal of Trauma and Acute Care Surgery, vol. 73, no. 6, 2012, pp. 1423–1427., doi:10.1097/ta.0b013e318271c1c7.
- Tanizaki, Shinsuke, et al. “Small Tube Thoracostomy (20–22 Fr) in Emergent Management of Chest Trauma.” Injury, vol. 48, no. 9, 2017, pp. 1884–1887., doi:10.1016/j.injury.2017.06.021.
- ATLS®: Advanced Trauma Life Support Student Course Manual. American College of Surgeons, 2018.
- Bauman, Zachary M., et al. “A Prospective Study of 7-Year Experience Using Percutaneous 14-French Pigtail Catheters for Traumatic Hemothorax/Hemopneumothorax at a Level-1 Trauma Center: Size Still Does Not Matter.” World Journal of Surgery, vol. 42, no. 1, 2017, pp. 107–113., doi:10.1007/s00268-017-4168-3.
- Lin, Hsing-Lin, and Yi-Pin Chou. “14-French Pigtail Catheters for Traumatic Hemothorax/Hemopneumothorax: Size Does Not Matter.” World Journal of Surgery, vol. 42, no. 8, 2017, pp. 2686–2686., doi:10.1007/s00268-017-4425-5.
- Durai, Rajaraman, et al. “Managing a Chest Tube and Drainage System.” AORN Journal, vol. 91, no. 2, 2010, pp. 275–283., doi:10.1016/j.aorn.2009.09.026.
- Hernandez, Matthew C., et al. “Complications in Tube Thoracostomy.” Journal of Trauma and Acute Care Surgery, vol. 85, no. 2, 2018, pp. 410–416., doi:10.1097/ta.0000000000001840.
- Sritharen, Yoginee, et al. “External Validation of a Tube Thoracostomy Complication Classification System.” World Journal of Surgery, vol. 42, no. 3, 2017, pp. 736–741., doi:10.1007/s00268-017-4260-8.
- Jones, Caleb W., et al. “Complications Associated With Placement of Chest Tubes: A Trauma System Perspective.” Journal of Surgical Research, vol. 239, 2019, pp. 98–102., doi:10.1016/j.jss.2019.01.012.
- Stawicki, Stanislawp. A., et al. “Thoracostomy Tubes: A Comprehensive Review of Complications and Related Topics.” International Journal of Critical Illness and Injury Science, vol. 4, no. 2, 2014, p. 142., doi:10.4103/2229-5151.134182.
- Maxwell, Robert A., et al. “Use of Presumptive Antibiotics Following Tube Thoracostomy for Traumatic Hemopneumothorax in the Prevention of Empyema and Pneumonia—A Multi-Center Trial.” The Journal of Trauma: Injury, Infection, and Critical Care, vol. 57, no. 4, 2004, pp. 742–749., doi:10.1097/01.ta.0000147481.42186.42.
- Luchette, Fred A., et al. “Practice Management Guidelines for Prophylactic Antibiotic Use in Tube Thoracostomy for Traumatic Hemopneumothorax: The EAST Practice Management Guidelines Work Group.” The Journal of Trauma: Injury, Infection, and Critical Care, vol. 48, no. 4, 2000, pp. 753–757., doi:10.1097/00005373-200004000-00027.
- Ayoub, Firas, et al. “Use of Prophylactic Antibiotic in Preventing Complications for Blunt and Penetrating Chest Trauma Requiring Chest Drain Insertion: a Systematic Review and Meta-Analysis.” Trauma Surgery & Acute Care Open, vol. 4, no. 1, 2019, doi:10.1136/tsaco-2018-000246.




