Author: Lap Woon Cheung, MB ChB, FHKCEM (@lawrche, International Emergency Ultrasound Fellow, Icahn School of Medicine at Mount Sinai) // Edited by: Stephen Alerhand MD (@SAlerhand, Instructor of Emergency Medicine and Ultrasound Fellow, Icahn School of Medicine at Mount Sinai) and Manpreet Singh, MD (@MPrizzleER – Assistant Professor in Emergency Medicine / Department of Emergency Medicine – Harbor-UCLA Medical Center)
Case
A 58 year-old male with history of intravenous (IV) drug use, cervical stenosis with myelopathy, and hypertension presented to the Emergency Department with fever and right thigh pain for 3 days. He admitted to IV heroin injection over the right groin region 1 week ago.
Vital signs were: BP 89/45, Pulse 110, SpO2 98%, RR 14, Temperature 102 F.
On physical exam, he looked generally weak and malnourished. The rest of the exam was notable for needle marks over the groins bilaterally and cellulitic changes over the right upper thigh.
A quick bedside ultrasound showed a hyperdynamic left ventricle and an inferior vena cava with significant respiratory variation. There was also no sign of groin abscess or pseudoaneurysm, nor any non-compressible vein in the femoropopliteal region suggestive of deep vein thrombosis. In view of his sepsis and dehydration, the plan for antibiotics and aggressive fluid resuscitation was initiated.
Peripheral IV access attempts by nursing colleagues failed due to thrombosing veins. Central venous access via the femoral vein (overlying cellulitis) and internal jugular vein (limited neck mobility due to cervical stenosis with myelopathy) were deemed inappropriate or challenging. Subclavian/axillary vein catheterization — a not commonly performed ED procedure — using ultrasound guidance was next proposed.
Anatomy and Clinical Relevance
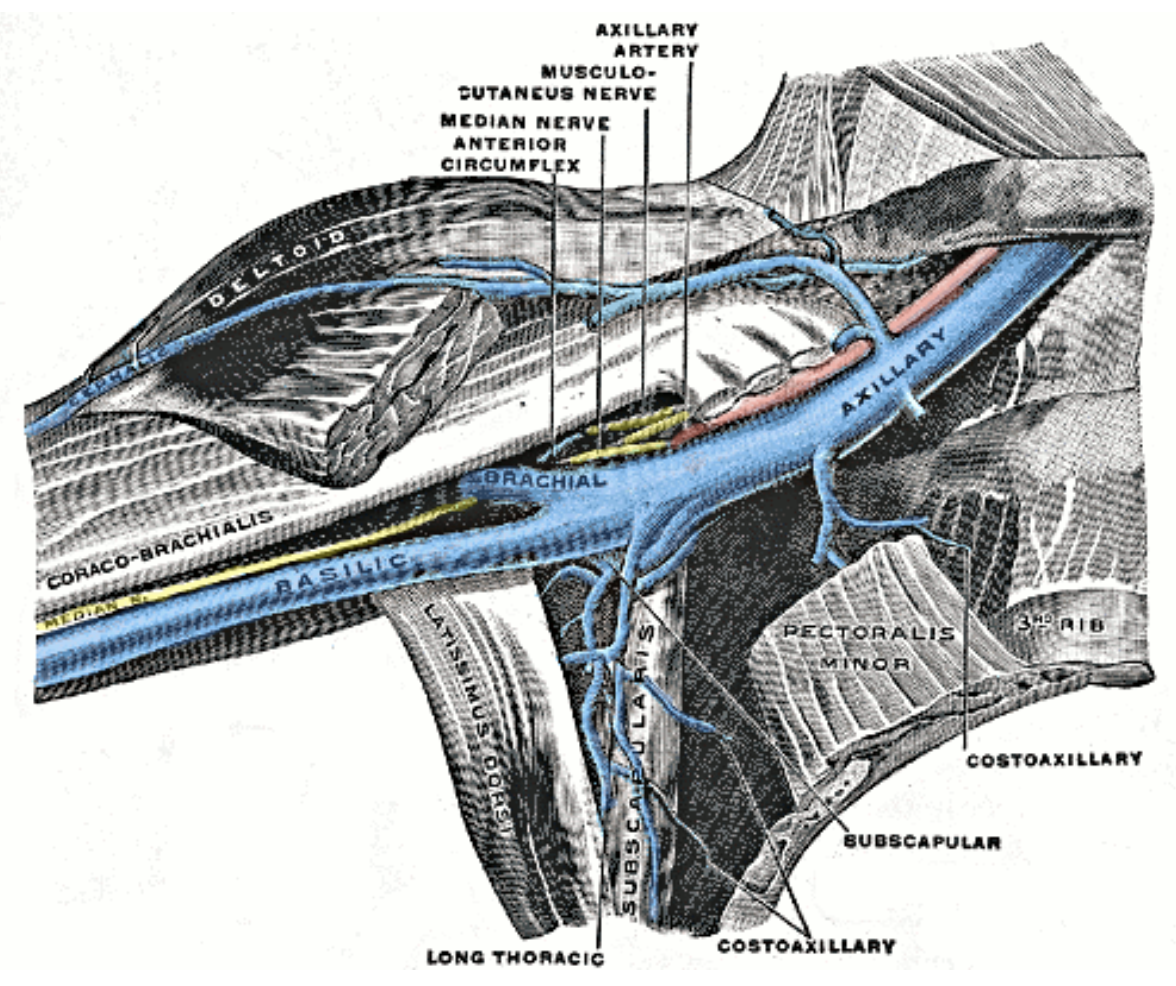
After passing the lower border of the teres major, the basilic vein becomes the axillary vein. Once it passes the lateral border of the first rib, the axillary vein then becomes the subclavian vein posterior to the clavicle (1) (Figure 1). It tracks medially and inferiorly to join the internal jugular vein as they merge into the brachiocephalic vein. The axillary vein and subclavian vein accompany their corresponding arteries along their course with some variation in anatomical relationship (2), so the traditional landmark approaches may not be reliable.
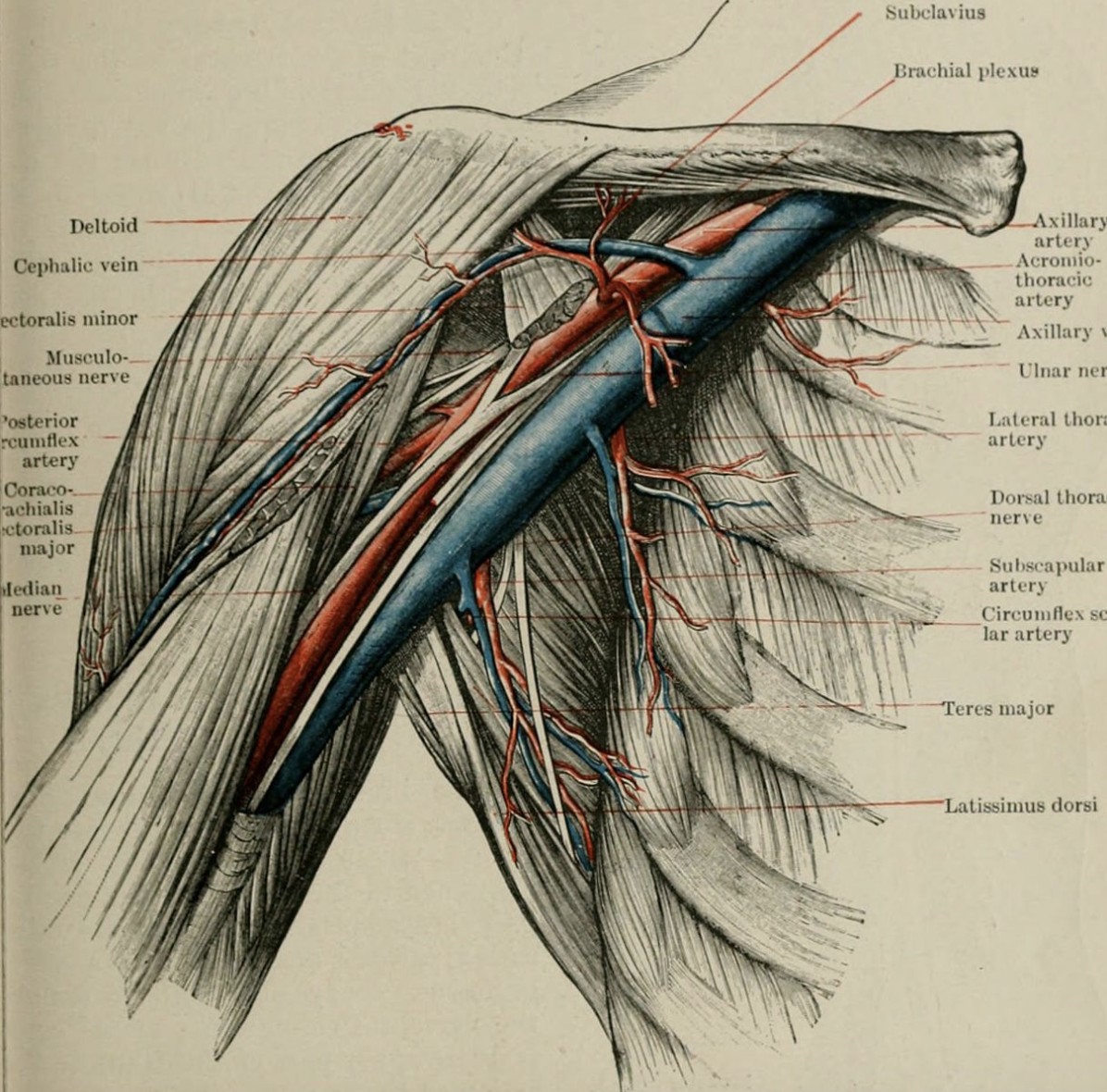
In the traditional infraclavicular landmark approach to subclavian vein access, the needle is directed posterior to the clavicle, just underneath the midclavicular line, and toward the suprasternal notch. This access site is typically incompressible. It carries the potential risk of pneumothorax due to its close proximity to the pleura. In moving the ultrasound probe laterally, the vein (now the axillary vein) emerges from behind the clavicle along with its accompanying artery. Here, it is further from the pleura, becomes more compressible, and importantly, is better visualized with ultrasound (3). (Figure 2)
Technical Infraclavicular Approach
1.Use the high-frequency (5.0-10.0 MHz) linear transducer, which offers the the highest resolution for this relatively superficial structure.
2. Start by placing the transducer in the sagittal plane over the middle third of the clavicle, with the transducer marker facing cephalad (Figure 3). Visualize the clavicle and pleural line as landmarks (Figures 4 & 5).

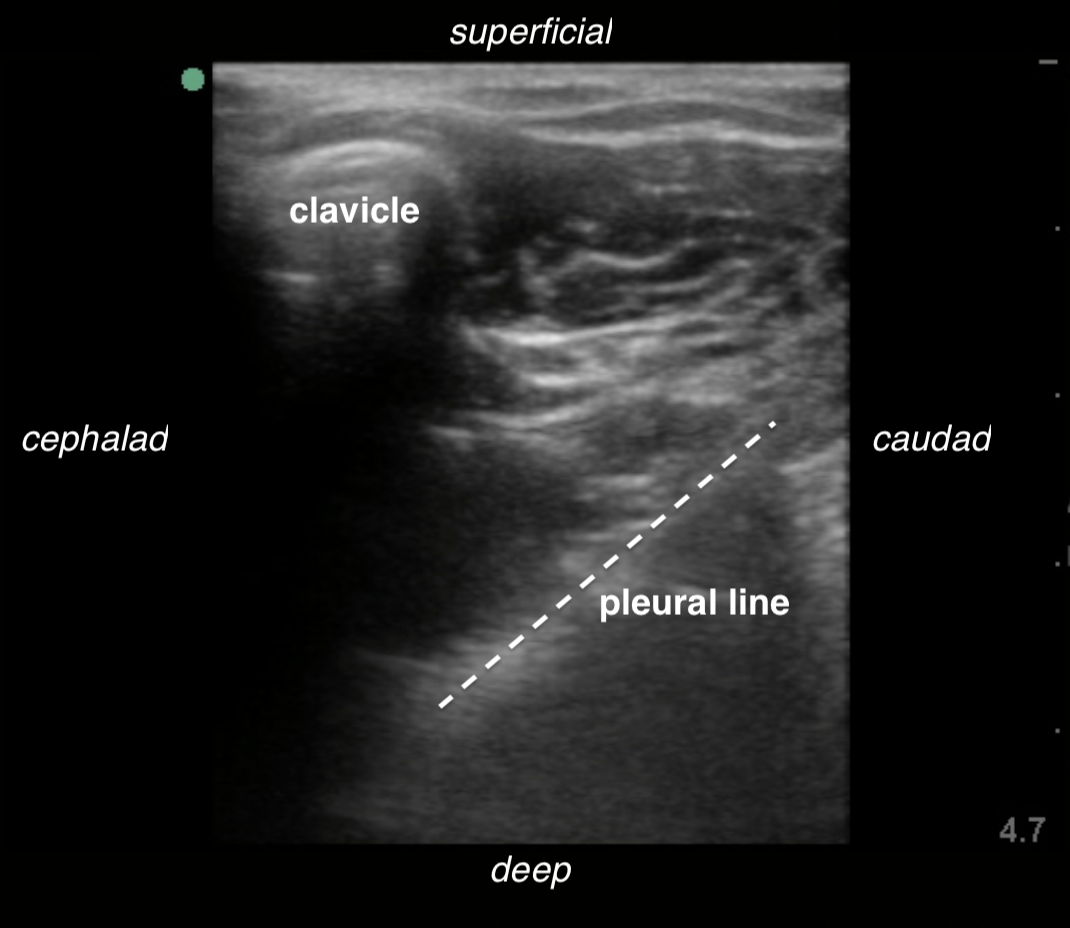
Figures 4 & 5. The subclavian vein (blue) and artery (red) can be identified. The clavicle and pleura serve as landmarks.
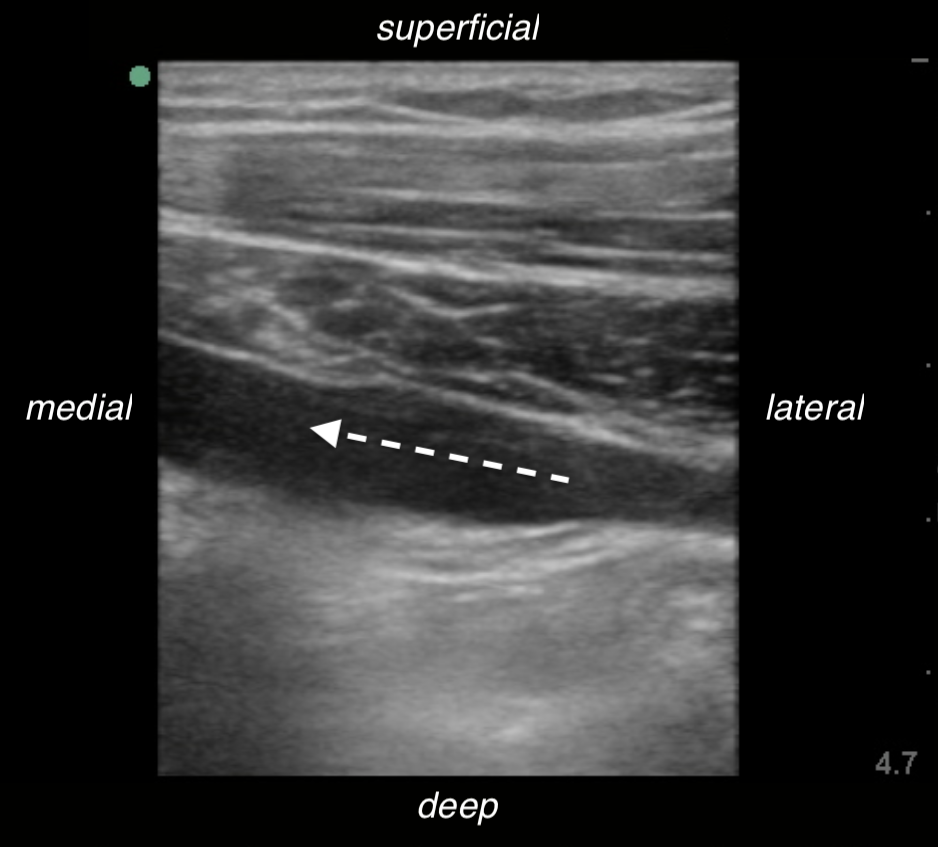
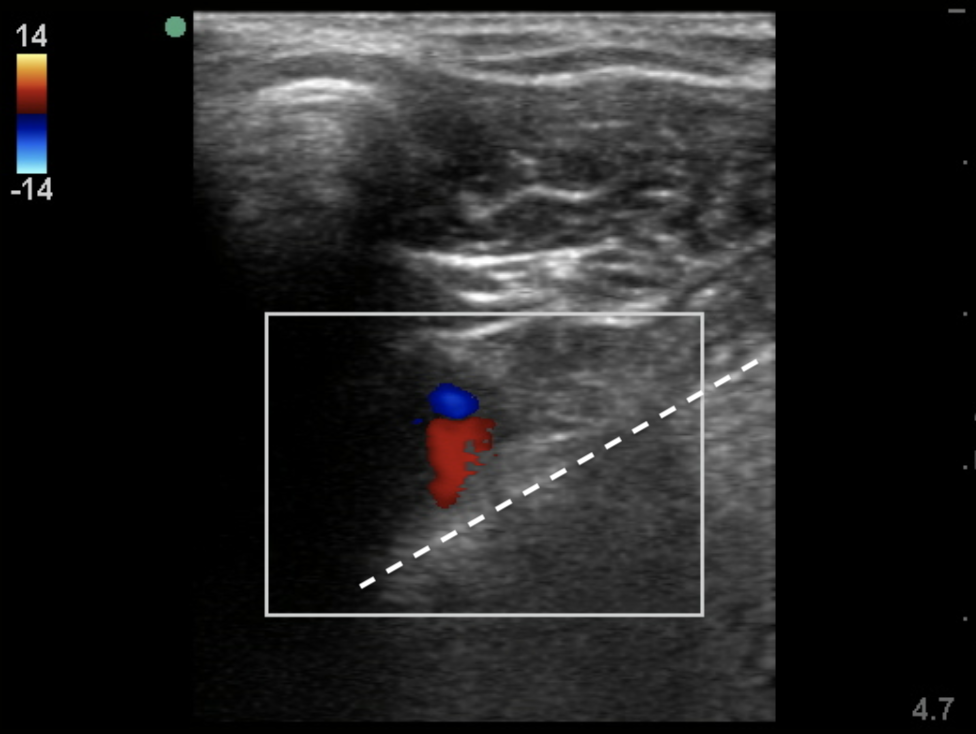
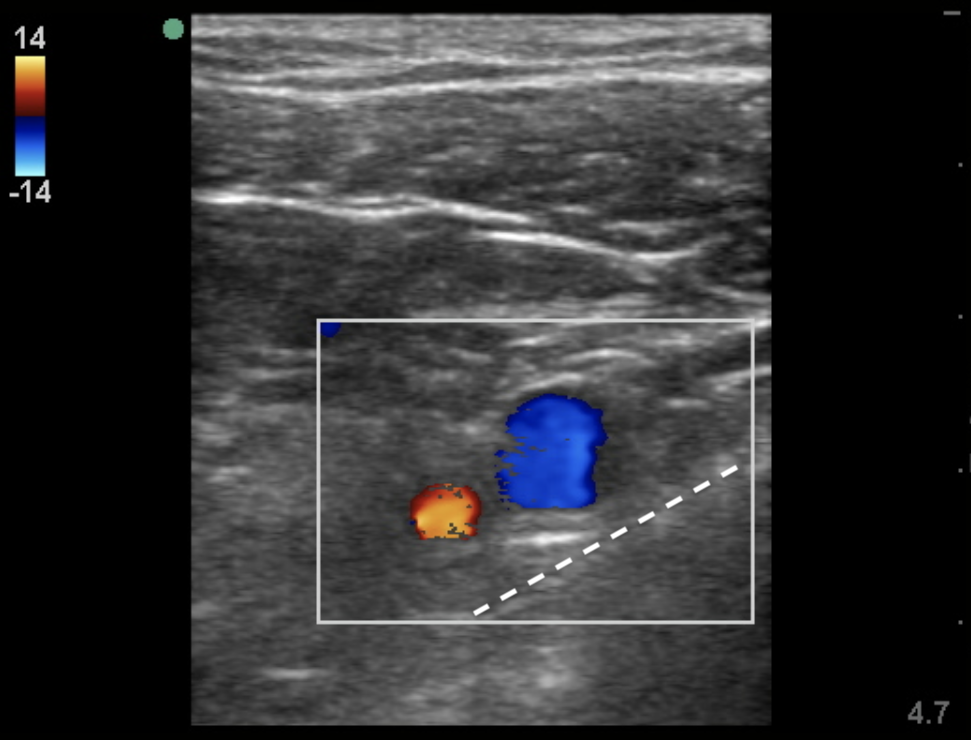
3. Slide laterally until the acoustic shadowing of the clavicle is no longer obscuring the underlying structures. Identify the axillary vein and artery in short-axis, as well as the pleural line. Differentiate the vein from artery with the help of color Doppler (Figure 6).
4. Follow the axillary vein laterally until it is not longer overlapping the artery, and the pleura remains at a distance.
5. Rotate the probe 90 degrees into the long-axis view and direct the needle safely, as with other central venous catheterizations (Figures 7 & 8).
![]()

Figures 7 & 8. Longitudinal view of the axillary vein.
Technical Points to Note
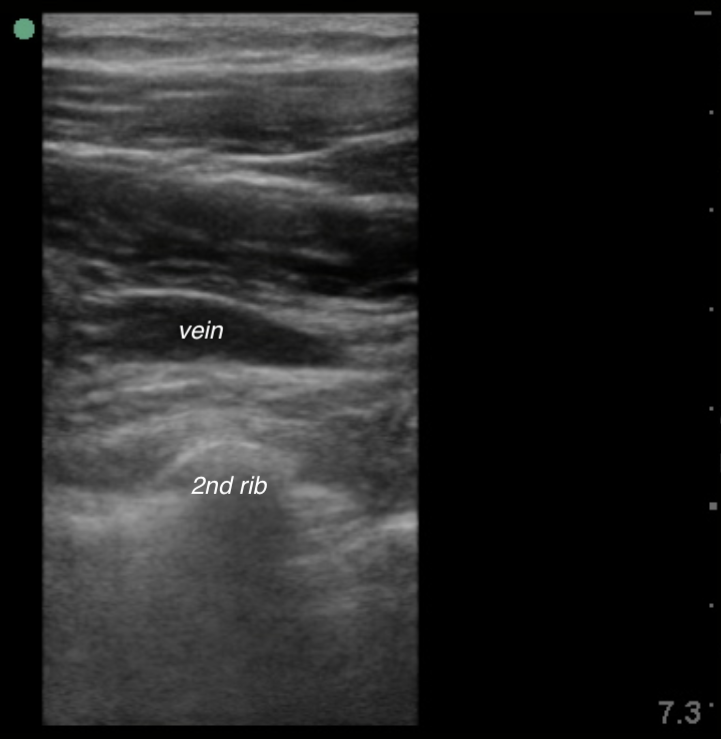
The above technique describes the infraclavicular approach of axillary vein catheterization. Different approaches have also been described. For instance, the supraclavicular approach enables visualization of the subclavian vein with the linear or endocavitary probe. This approach has the advantage of a more direct angle towards the superior vena cava (4). The long-axis method is superior to the short-axis method with regards to greater first-attempt success, fewer needle redirections, and fewer arterial punctures (5). Another approach called the Pleural Avoidance with Rib Trajectory (PART) technique targets the axillary vein at a point where it traverses over the second rib during needle advancement (Figure 9). It provides a protective rib shield between the vein and pleura (Figure 10). It has been shown to reduce the risk of pneumothorax and allows for compression in case of bleeding (Figure 9. PART method (6)
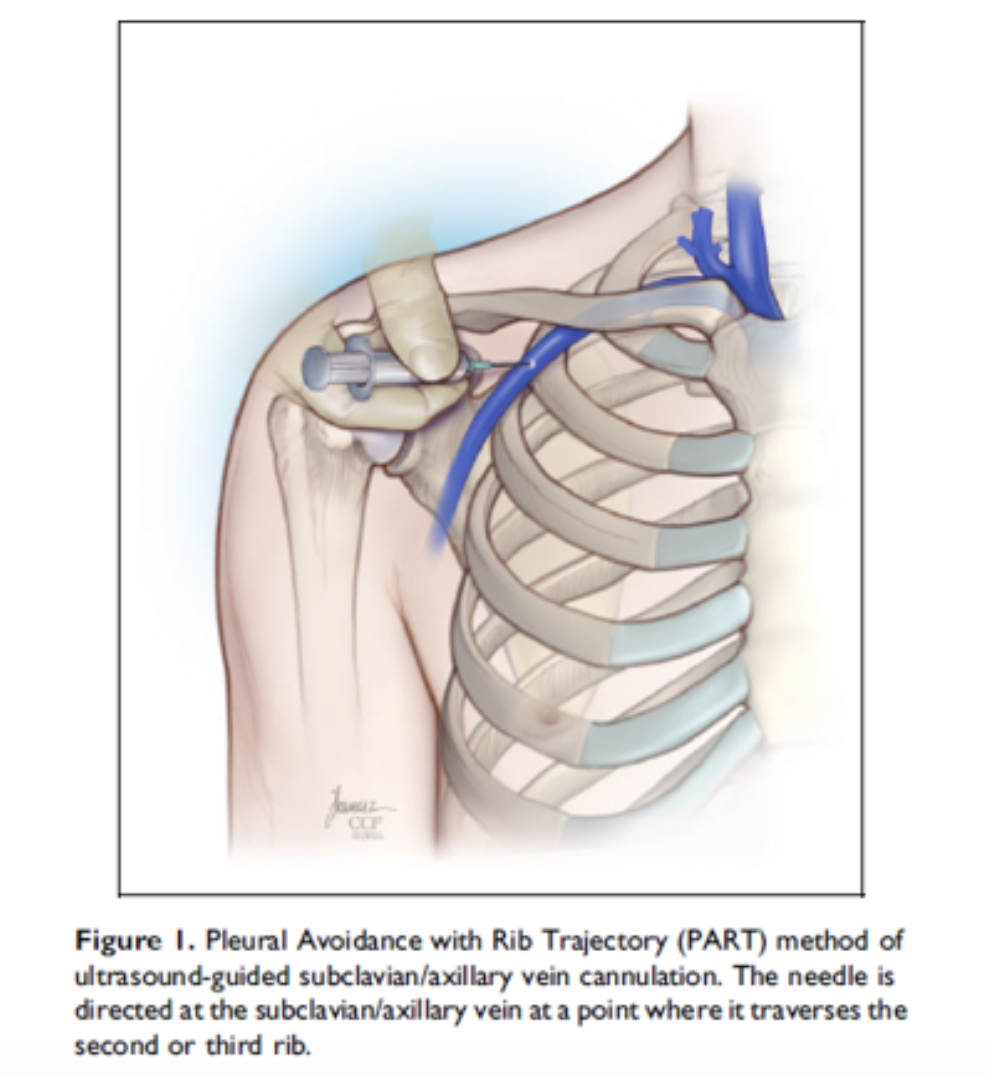
Figure 9: PART Method
Indications
- Emergency venous access for fluid and drug administration
- Central venous pressure and oxygenation monitoring
- Introduction of transvenous cardiac pacing and pulmonary artery catheter
- Long-term central venous access (preferable to internal jugular and femoral vein access as it allows for neck movement and ambulation without discomfort)
- Other central veins not accessible or contraindicated
Contraindications
- Coagulopathy
- Combative or uncooperative patients
- Overlying infection, chest wall deformity or trauma
- Ipsilateral vein cannulation in the presence of an implantable pacemaker
- Ipsilateral vein cannulation in patients relying on a single lung
- Intraluminal thrombosis visualized by ultrasound
Bottom Line
Compared with internal jugular and femoral vein access, subclavian/axillary vein cannulation has the lowest infection rate (7). It is suggested as the central line access of choice by the Centers for Disease Control and Prevention guidelines for the prevention of catheter-related bloodstream infections (CRBSI) in adult patients (8). Though the practice may be hindered by the feared complication of pneumothorax (9), studies have shown an increased success rate, decreased time to achieve access, and decreased number of attempts with ultrasound guidance (10). There are also occasional situations where internal jugular and/or femoral vein approaches are contraindicated, e.g. anatomic distortions and suspected injuries of the respective structures. Subclavian/axillary vein catheterization has a role in emergency care, and emergency physicians should be familiar with the indications and proper technique.
FOAMed Resources
- Ultrasound-guided left subclavian central venous catheterisatio
- MGH Ultrasound Youtube Video – Tutorial Ultrasound Guided Subclavian Line
- Ultrasound-Guided Cannulation: Time to Bring Subclavian Central Lines Back
- PulmCrit- Shrug Technique for US-guided subclavian lines
- Changing Arm Position for Ultrasound Guided Subclavian Central Lines?
- The PART method for US-guided subclavian CVC’s with Mourad Senussi
References
- Snell RS. Clinical Anatomy by Regions. 9th Ed. Lippincott Williams & Wilkins; 2011.
- Yeow KM, Kaufman JA, Rieumont MJ, et al: Axillary vein puncture over the second rib. Am J Roentgenol 1998;170(4):924–926.
- Galloway S, Bodenham A: Ultrasound imaging of the axillary vein – anatomical basis for central venous access. Br J Anaesth 2003;90(5):589–595.
- Stachura MR, Socransky SJ, Wiss R, Betz M. A comparison of the supraclavicular and infraclavicular views for imaging the subclavian vein with ultrasound. Am J Emerg Med. 2014; 32(8):905-908.
- Sommerkamp, SK, Romaniuk, VM, Witting, MD, Ford, DR, Allison, MG, Euerle, BD. A comparison of longitudinal and transverse approaches to ultrasound-guided axillary vein cannulation. Am J Emerg Med. 2013;31(3):478–481.
- Senussi MH, Kantamneni PC, Omranian A et al. Revisiting Ultrasound-Guided Subclavian/Axillary Vein Cannulations: Importance of Pleural Avoidance With Rib Trajectory J Intensive Care Med. 2017; 32(6):396-399.
- Lorente L, Henry C, Martín MM, Jiménez A, Mora ML. Central venous catheter-related infection in a prospective and observational study of 2,595 catheters. Crit Care. 2005; 9(6):R631–5.
- Guidelines for the Prevention of Intravascular Catheter-Related Infections (2011) https://www.cdc.gov/infectioncontrol/guidelines/bsi/recommendations.html
- Parienti, JJ, Mongardon, N, Mégarbane, B. Intravascular complications of central venous catheterization by insertion site. N Engl J Med. 2015;373(13):1220–1229.
- Fragou M, Gravvanis A, Dimitriou V, et al. Real-time ultrasound-guided subclavian vein cannulation versus the landmark method in critical care patients: a prospective randomized study. Crit Care Med. 2011; 39(7):1607–1612.





1 thought on “US Probe: Ultrasound Guided Subclavian/Axillary Vein Catheterization”
Pingback: LITFL Review 332 | Edwin M. Thames