Author: Desiree Brooks, MD (Senior EM Resident Physician, UTSW / Parkland Memorial Hospital) // Edited by: Alex Koyfman, MD (@EMHighAK, EM Attending Physician, UTSW / Parkland Memorial Hospital) and Brit Long, MD (@long_brit, EM Chief Resident at SAUSHEC, USAF)
1) A 46-year-old male that reports he is otherwise healthy except for a childhood history of asthma presents to your emergency department with a 3-day history of fever, cough productive of green sputum, and shortness of breath. He has a temperature of 101.2 degrees Fahrenheit, he is tachycardic to 122 beats per minute, his respiratory rate is 22, he is hypoxic to 89% on room air, and he has a normal blood pressure. On physical exam, he appears mildly ill and you hear some scattered wheezes and has decreased breath sounds in his right middle and lower lobes. Your workup confirms your suspicion of pneumonia, and he has had mild improvement (wheezing, fever, and heart rate improve, but he remains tachypneic and hypoxic) with your treatments. You decide to admit for IV antibiotics. The inpatient team asks for blood cultures, and you wonder if this will benefit your patient.
2) A 68-year-old Hispanic female presents to your emergency department with fatigue, fever, and rash. She reports that she does not take any medications. Her vital signs are normal. She looks well. You see the following rash:
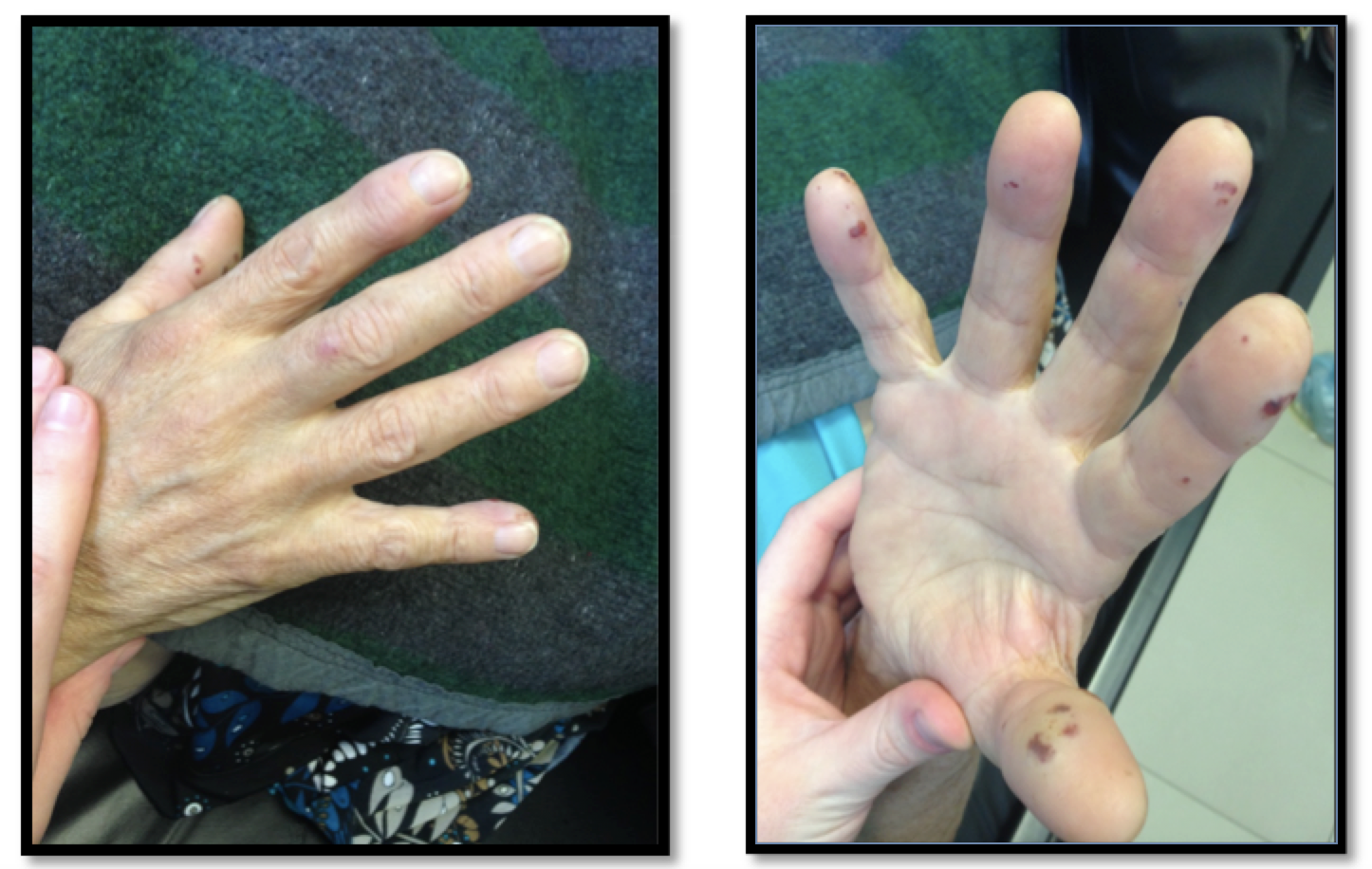
You diagnose her with bacterial endocarditis and admit her for IV antibiotics. You ordered two blood cultures in the emergency department to be drawn at separate venipuncture sites and wonder if you should have ordered a third.
Discussion
Blood cultures are commonly ordered in the emergency department for patients with suspected infection. They are generally considered to be the most sensitive method for detection of bacteremia or fungemia1 and are generally thought to be useful in certain diagnoses and critically ill patients; however, it appears as though rising trends in obtaining blood cultures over the past decade in low-risk patients have been tied to core measures and payments (introduced by the Joint Commission on Accreditation of healthcare Organizations and Centers for Medicaid and Medicare Services).2 As a result, their utility has been a focus of controversy prompting ample research in recent years all conveying the same information: blood cultures ordered from the emergency department rarely alter patient management and can at times cause harm to patients. Not only is the harm financial, false-positive results can lead to inappropriate antimicrobial use and longer hospital stays.3
Yield of Blood Cultures
The yield of blood cultures has been evaluated in multiple studies in several different patient populations. A study published in 2006 showed a useful culture rate of 2.8% (6/218) – meaning clinical management was influenced by culture result – and suggested that blood cultures should be eliminated in immunocompetent patients with common illnesses such as urinary tract infection, community acquire pneumonia, and cellulitis.4 Another study published in 2007 showed that of 2,210 blood cultures, only 132 (6%) yielded growth, and 4 (0.18%) resulted in altered patient management.5
For patients with pneumonia, a NNT approaching 150 has been found in regards to blood cultures affecting patient care (such as cultures causing modification of the antibiotic regimen). This is based on 0.18% and 1.6% of blood cultures actually affecting patient management.6 Another study from 2007 found a true positive rate of 3.4% and false positive rate of 7.8%.7 Of these true positive cultures, 3 out of 23 patients had management changed based on cultures. These authors recommended eliminating use of blood cultures for community-acquired pneumonia.7 In 2005, another article was published also supporting decreased use of blood cultures and concluded “blood cultures rarely altered therapy for patients presenting to the ED with pneumonia. More discriminatory blood culture use may potentially reduce resource utilization.”8
Cellulitis is a common condition and is broken into simple and complicated, which is defined by an immunocompromised state such as HIV/AIDS, chemotherapy, organ transplantation, diabetes, and vascular insufficiency. Simple cellulitis is defined by absence of these conditions. Mills et al. examined five other studies, finding blood cultures did not alter treatment in immunocompetent patients with cellulitis.9 Paolo et al. examined the yield of blood cultures and found contaminated cultures in 4% of complicated and 3% of uncomplicated cellulitis cases. A change in management occurred in 6 of 314 cases in complicated cellulitis and in 4 of 325 uncomplicated cases. True positive cultures occurred more commonly in patients with fever and diabetes.10
Are there any factors associated with true positive cultures?
Coburn et al. in JAMA 2012 conducted a meta-analysis investigating true positive blood cultures in a population of immunocompetent adults.11 Predictors of true positive cultures included shaking chills, hypotension, vasopressor use, neutrophil to lymphocyte ratio > 10, and presence of SIRS. However, risk factors including subjective fever, tachycardia alone, elevated WBC, and documented fever were not found to be sensitive. Blood cultures were recommended in patients with pyelonephritis, severe sepsis, septic shock, and meningitis. Cultures in pneumonia and cellulitis were not recommended.11
A clinical predication rule has been created and validated for use in predicting true blood cultures.12 A prospective analysis in 2008 evaluated 3,370 patients. The study found several criteria increasing the predictive value of blood cultures. The major criteria includes suspected endocarditis, temperature > 103F, and indwelling vascular catheter. Minor criteria include temperature > 101F, age > 65 years, chills, vomiting, SBP < 90 mm Hg, WBC > 18,000, band count > 5%, platelets < 150,000, and creatinine > 2 mg/dL. The negative predictive value for true positive blood culture was 99.4% in the derivation group and 99.1% in the validation group.12
A second study in 2011 evaluated multiple predictors associated with bacteremia. This study conducted in an urban ED found a 90.9% probability of a negative blood culture if the following were negative: no chemotherapy within past 6 moths, heart rate < 100, and normal or elevated electrolytes to predict a negative blood culture.13 This rule has not been validated.
When (and how) to order blood cultures in the ER
UpToDate suggests that diagnoses in which blood cultures are considered important include sepsis, meningitis, osteomyelitis, septic arthritis, endocarditis, peritonitis, pneumonia, and fever of unknown origin. 1 In general, patients who are acutely ill or have high likelihood of continuous bacteremia should have blood cultures drawn in the emergency department.11
At least two sets of blood cultures should be drawn prior to initiation of antimicrobial therapy. A single blood culture lacks sensitivity as well as precludes the ability to distinguish contaminants from true bacteremia.17 It is reasonable to obtain four blood cultures when the probability of bacteremia is high and the anticipated pathogen is likely to be a common contaminant (ex: infected internal hardware is suspected).1
An article published in 2008 demonstrated that fever at the time of blood culture collection is neither sensitive nor specific for the presence of bacteremia.18 Blood cultures therefore do not need to be rapidly drawn when a patient is noted to be febrile.
Antiseptic technique is essential. The skin should be cleaned first with an alcohol swab followed by chlorhexidine from two separate venipuncture sites.14 An IV catheter line at the time of IV insertion should not be used.15 Volume does matter when obtaining a culture, as there is a 3% increase in positive culture per milliliter blood obtained. At least 7 ml per bottle are recommended.16
Cases
1) Blood cultures are still recommended in this patient because he has evidence of sepsis on arrival to the emergency department.
2) The Duke diagnostic criteria are widely used to diagnose endocarditis and require at least 2 positive blood cultures either persistently positive for the same organism from cultures drawn more than 12 hours apart OR 3 or more separate blood cultures drawn at least 1 hour apart.11, 19
Summary
- In general, patients who are acutely ill or have high likelihood of continuous bacteremia should have blood cultures drawn in the emergency department.
- Blood cultures should not be taken from routinely stable, immunocompetent patients with common or typical infections such as cellulitis, orchitis, and community acquired pneumonia.12
- Blood cultures should be obtained prior to initiation of antibiotic therapy to maximize possibility of being useful clinically
- When you have high suspicion for endocarditis, you may order 3 blood cultures from different venipuncture sites in the ED, each drawn 1 hour apart, OR 2 blood cultures from different venipuncture sites with a third to be ordered >12 hours later by your inpatient team.11,19
- Fever at the time of blood culture collection is neither sensitive nor specific for the presence of bacteremia.10
- An IV catheter line at the time of IV insertion should not be used.8
References / Further Reading
- Doern, Gary. Blood cultures for the detection of bacteremia. UpToDate. Accessed April 1, 2016. http://www.uptodate.com/contents/blood-cultures-for-the-detection-of-bacteremia/.
- Makam AN, Auerbach AD, Steinman MA. Blood Culture Use in the Emergency Department in Patients Hospitalized for Community-Acquired Pneumonia. JAMA Intern Med. 2014;174(5):803-806. doi:10.1001/jamainternmed.2013.13808.
- Mandell LA, Wunderink RG, Anzueto A, et al; Infectious Diseases Society of America; American Thoracic Society. Infectious Diseases Society of America/American Thoracic Society consensus guidelines on the management of community-acquired pneumonia in adults. Clin Infect Dis. 2007;44(suppl 2):S27-S72.
- Mountain D, Bailey PM, O’Brien D, Jelinek GA. Blood cultures ordered in the adult emergency department are rarely useful. Eur J Emerg Med. 2006;13(2):76–9. doi:10.1097/01.mej.0000188231.45109.ec.
- Howie N, Gerstenmaier JF, Munro PT. Do peripheral blood cultures taken in the emergency department influence clinical management? Emerg Med J. 2007;24(3):213–4. doi: 10.1136/emj.2006.039875.
- Kelly AM. Clinical impact of blood cultures taken in the emergency department. J Accid Emerg Med. 1998 Jul;15(4):254-6.
- Benenson RS, Kepner AM, Pyle DN 2nd, Cavanaugh S. Selective use of blood cultures in emergency department pneumonia patients. J Emerg Med. 2007 Jul;33(1):1-8.
- Kennedy, Maura et al. Do Emergency Department Blood Cultures Change Practice in Patients With Pneumonia? Annals of Emergency Medicine. 2005. Volume 46, Issue 5, 393 – 400.
- Mills AM, Chen EH. Are blood cultures necessary in adults with cellulitis? Ann Emerg Med. 2005 May;45(5):548-9.
- Paolo WF, Poreda AR, Grant W, Scordino D, Wojcik S. J Emerg Med. 2013 Aug;45(2):163-7.
- Coburn B, Morris AM, Tomlinson G, Detsky AS. Does this adult patient with suspected bacteremia require blood cultures? JAMA 2012; 308:502.
- Shapiro NI, Wolfe RE, Wright SB, Moore R, Bates DW. Who needs a blood culture? A prospectively derived and validated prediction rule. J Emerg Med. 2008;35(3):255–64. doi: 10.1016/j.jemermed.2008.04.001
- Roque PJ, Oliver B, Anderson L, et al. Blood culture prediction rule in an urban emergency department. Ann Emerg Med. 2011;58(4):S290.
- Little JR, Murray PR, Traynor PS, Spitznagel E. A randomized trial of povidone-iodine compared with iodine tincture for venipuncture site disinfection: effects on rates of blood culture contamination. Am J Med 1999; 107:119.
- Norberg A, Christopher NC, Ramundo ML, et al. Contamination rates of blood cultures obtained by dedicated phlebotomy vs intravenous catheter. JAMA 2003; 289:726.
- Mermel LA, Maki DG. Detection of bacteremia in adults: consequences of culturing an inadequate volume of blood. Ann Intern Med. 1993 Aug 15;119(4):270-2.
- Mirrett S, Weinstein MP, Reimer LG, et al. Relevance of the number of positive bottles in determining clinical significance of coagulase-negative staphylococci in blood cultures. J Clin Microbiol 2001; 39:3279.
- Riedel S, Bourbeau P, Swartz B, et al. Timing of specimen collection for blood cultures from febrile patients with bacteremia. J Clin Microbiol 2008; 46:1381.
- Durack DT, Lukes AS, Bright DK. New criteria for diagnosis of infective endocarditis: utilization of specific echocardiographic findings. Duke Endocarditis Service. Am J Med. 1994 Mar. 96(3):200-9.





3 thoughts on “Blood cultures: when do they make a meaningful impact on clinical care?”
I’m not convinced of your first case. Neither the new Feb 16 rules nor the old Ones fit for full-on sepsis here:
http://www.medscape.com/viewarticle/859281
Amazing post either way.
I’m not convinced of your first case. Neither the new Feb 16 rules nor the old Ones fit for full-on sepsis here:
http://www.medscape.com/viewarticle/859281
Amazing post either way.
Pingback: AIR Series: Infectious Disease Module (2016) – Global Intensive Care