
Originally published at CoreEM.net, dedicated to bringing Emergency Providers all things core content Emergency Medicine available to anyone, anywhere, anytime. Reposted with permission.
Follow Dr. Swaminathan and CORE EM on twitter at @EMSwami and @Core_EM
Written by Ryland Peace, MD and Edited by Anand Swaminathan, MD
Definition: Twisting of an ovary around its vascular supply
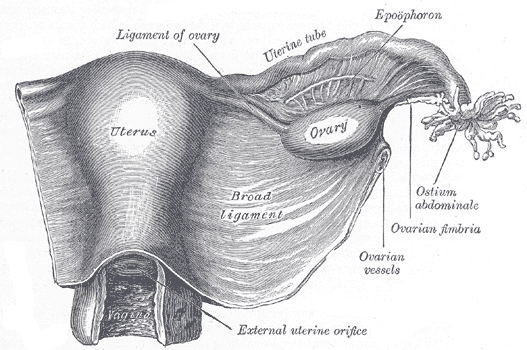
Pelvic Anatomy – wikimedia
Epidemiology
- Most common in reproductive-aged females but is found in females of any age
- 20-25% of cases found in pregnant females
- Risk factors: 1) ovary >4cm, 2) pregnancy, 3) patients undergoing IVF, 4) patients after tubal ligation
- Protective factors: 1) ovary >10cm, 2) intra-abdominal malignancy or adhesions
Mechanism
- Anatomy: Torsion is a mechanical disorder. Each ovary is supported by two ligaments, the suspensory ligament of the ovary (laterally) and the ligament of the ovary (medially). Each ligament contains its own arterial, venous, and lymphatic system.
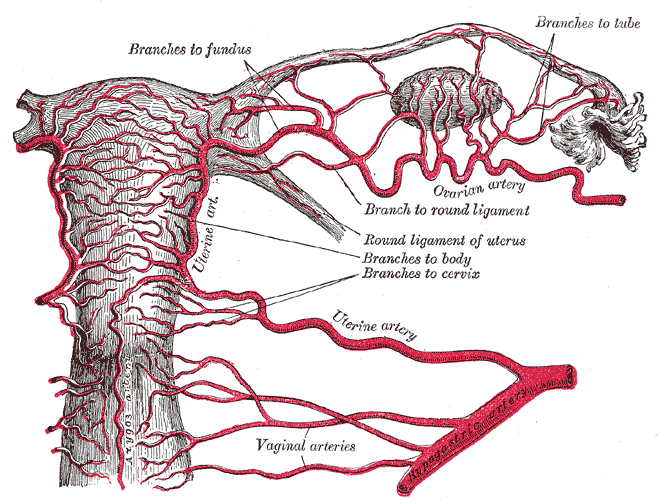
Pelvic Vascular Supply – Wikimedia
- Most cases involve an enlarged ovary (i.e. a cyst, mass, multiple ovarian follicles). This enlarged ovary then rotates on the axis of the ligaments. The twisting of the ligaments restricts lymphatic outflow resulting in congestion and further swelling. The swelling inhibits venous return, which results in additional congestion. Finally, arterial supply is compromised.
- Right ovary torsion is more common because the right utero-ovarian ligament is longer than the left and the sigmoid colon in the left side of the colon physically limits left ovarian movement.
Presentation
- Pain is the most common symptom (Houry 2001, Hasson 2010, White 2005)
- 90% report pelvic pain. Back and flank pain are common as well.
- 60-90% report sudden-onset of pain
- 80% of pain described as moderate or severe
- No consistent description of pain quality or radiation
- 40-70% report nausea and vomiting (Ashwal 2015)
- 2-20% have low-grade fever
- Abnormal vaginal bleeding is uncommon
- Infants present with vague symptoms, i.e. feeding intolerance, vomiting, abdominal distention, fussiness, or irritability.
- Premenarchal girls often have a longer duration of symptoms and commonly present with diffuse pain, fever or restlessness
Physical Exam
- Patients often look uncomfortable but otherwise, exam is inconsistent.
- Absence of abdominal tenderness is common
- Pelvic exams
- Limited utility
- 85-95% of patients have an adnexal mass but GYN attendings and residents had a poor sensitivity (21-36%) for detecting masses during pelvic exams under anesthesia (Padilla 2000).
- Emergency Physicians had poor inter-examiner reliability for detection of pelvic masses (23%) and the presence of adnexal tenderness (32%) (Close 2001).
- Regardless of expertise, the pelvic exam does not appear likely to be particularly useful in diagnosing, or ruling out, torsion.
Pelvic Ultrasound
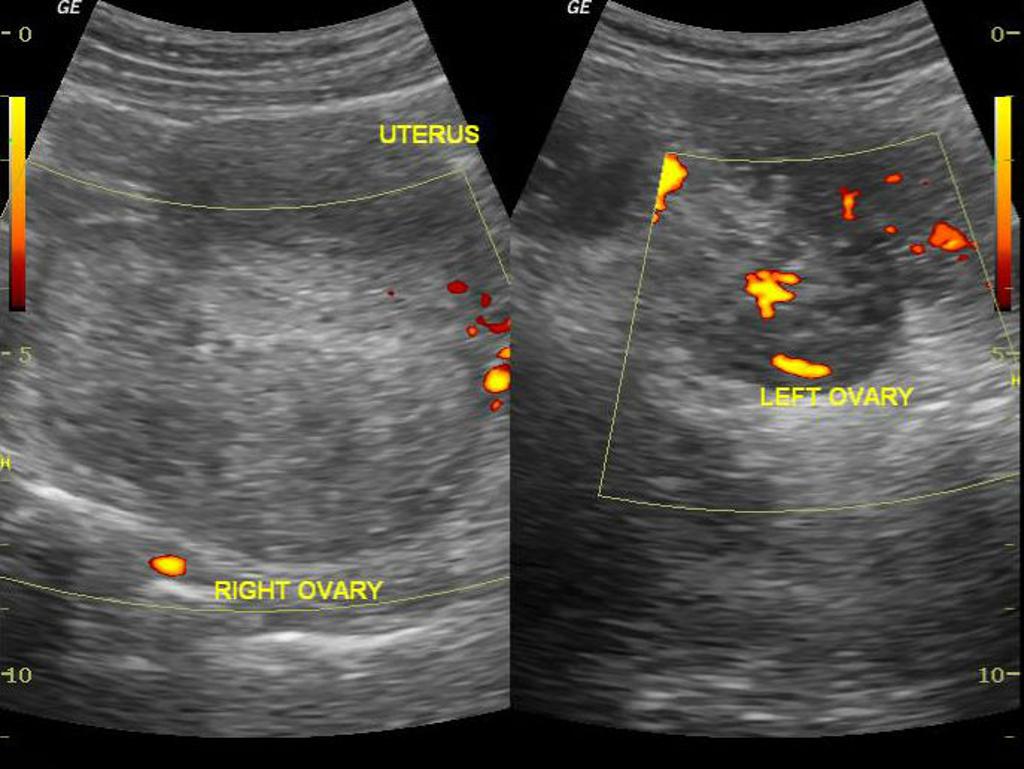
Ovarian Torsion US (Case courtesy of Dr Maulik S Patel, Radiopaedia.org. From the case rID: 30458)
- Most common initial imaging modality
- Ultrasound has high specificity but inadequate sensitivity
- Studies have not assessed the role of ED POCUS for the diagnosis of ovarian torsion
- Both transvaginal and transabdominal images should be obtained if possible as these views provide better resolution of the ovaries and its vessels as well as an appreciation for its spatial location in the abdomen, respectively
- Do NOT be reassured by the presence of arterial and venous flow on Doppler as one study found that 60% of torsion cases had normal flow (Peña 2010)
- Unilateral ovary measuring > 4cm is most common finding. Additionally, ovaries located close to midline are suggestive of torsion in the correct setting
- “String of Pearls” Sign
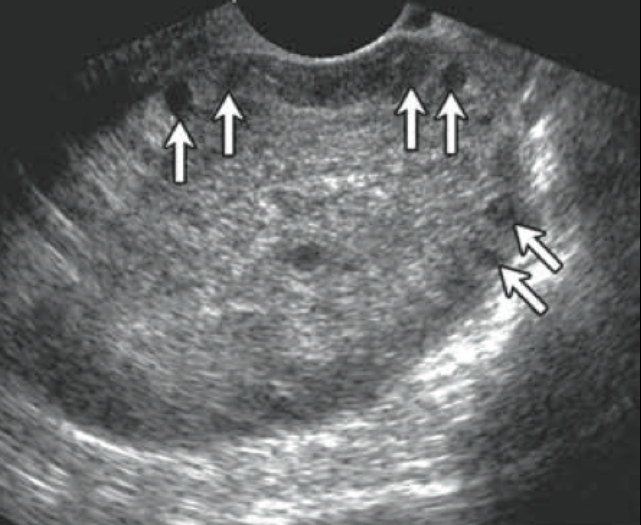
US with “String of Pearls” (Chang 2008)
- Multiple small, uniform cysts lined around the periphery of engorged ovary
- Highly specific for ovarian torsion
- CT
- Good alternate imaging modality for evaluating for ovarian torsion.
- Like US, studies suggest that torsion is unlikely in patients with CT showing ovaries that appear normal in size, location and appearance (Bronstein 2015, Swenson 2014).
- Findings
- Twisted ovarian pedicle is pathognomonic for torsion
- Other common findings
- Enlarged ovary (> 4.0 cm)
- Underlying ovarian lesion
- Distended pedicle
- Lack of enhancement
CT Images
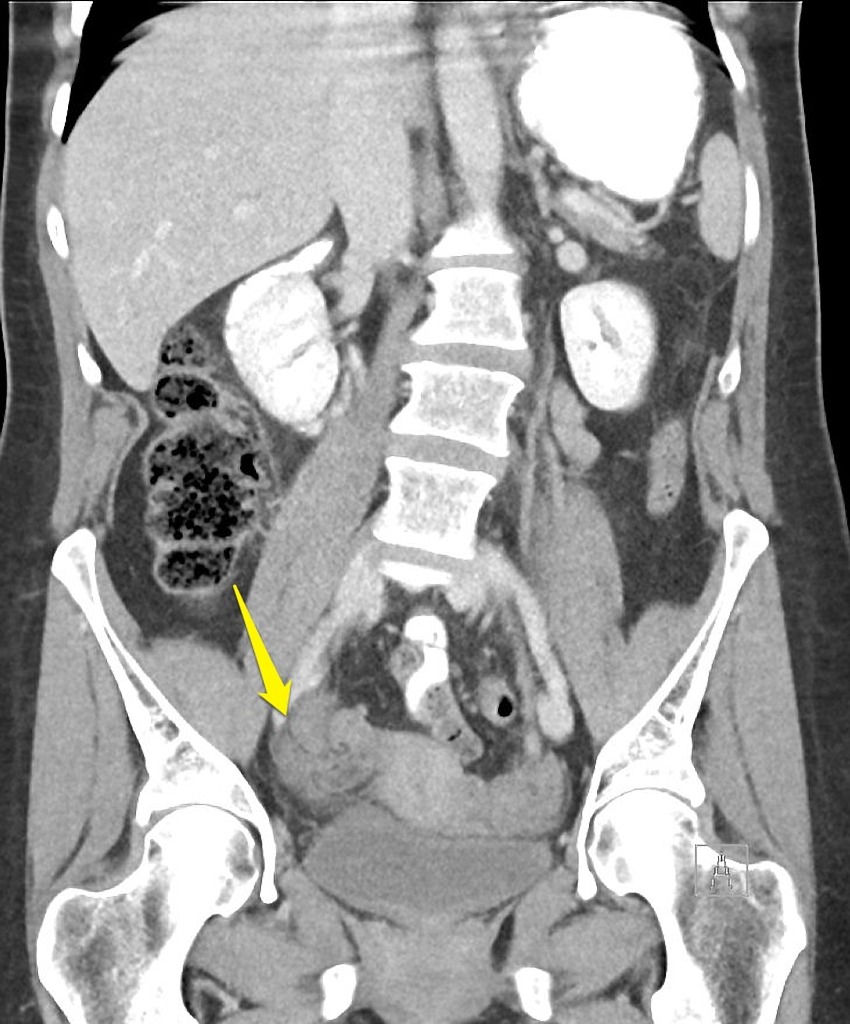
Ovarian Torsion CT – “Whirl Sign” (Case courtesy of RMH Core Conditions, Radiopaedia.org. From the case rID: 28265)

CT Ovarian Torsion (Case courtesy of Radiopaedia.org. From the case rID: 11724)

CT Ovarian Torsion (Case courtesy of Radiopaedia.org. From the case rID: 11723)
- Supportive Care
- Provide analgesia
- Provide antiemetics if necessary
- Emergent GYN consultation for exploratory surgery is required for possible ovarian salvage
Take Home Points
- Ovarian torsion rarely presents with classic symptoms. Always consider torsion when evaluating a female patient with abdominal pain, back pain, or flank pain.
- While US is a great first initial test for the evaluation of both ovarian torsion, do not be reassured by normal dopplers. The most common finding is an ovary > 4cm.
- CT may as sensitive as US. A CT in an adult female that shows normal sized and appearing ovaries likely excludes the diagnosis of torsion.
- Emergency GYN consult is required in all suspected ovarian torsion cases.
Read More
EM Lyceum: Ovarian Torsion
Radiopaedia: Ovarian Torsion
References
Ashwal E et al. Characteristics and Management of Ovarian Torsion in Premenarchal Compared With Postmenarchal Patients. Obstet Gynecol 2015; 126(3):514-20. PMID: 26244532
Bronstein M et al. Meta-analysis of B-mode ultrasound, Doppler ultrasound, and computed tomography to diagnose pediatric ovarian torsion. Eur J Pediatr Surg. 2015; 25(1):82-6. PMID: 25172980
Chang HC et. al. Pearls and Pitfalls in Diagnosis of Ovarian Torsion. RadioGraphics 2008; 28: 1335-1368. PMID: 18794312
Close RJ et al. Reliability of bimanual pelvic examinations performed in emergency departments. West J Med 2001; 175(4):240-4. PMID: 11577050
Hasson J et al. Comparison of adnexal torsion between pregnant and nonpregnant women. Am J Obstet Gynecol 2010; 202(6):536.e1-6. PMID: 20060090
Houry D, Abbott JT. Ovarian torsion: a fifteen-year review. Ann Emerg Med. 2001; 38(2):156. PMID: 11468611
Huchon, C., Fauconnier, A. Adnexal torsion: a literature review. Eur J Obstet Gynecol Reprod Biol 2010; 150(1):8-12. PMID: 20189289
Huchon C et al. Does this woman have adnexal torsion? Hum Reprod. 2012; 27(8):2359. PMID: 22674200
Kruszka PS, Kruska SJ. Evaluation of Acute Pelvic Pain in Women. Am Fam Physician. 2010; 82(2): 141-147. PMID: 20642266
Laufer MR (2015). Ovarian and fallopian tube torsion. In S.J. Falk (Ed.), UpToDate. Waltham, MA, 2015.
Pena J et al. Usefulness of Doppler sonography in the diagnosis of ovarian torsion. Fertil Steril 2000; 73(5):1047-50. PMID: 10785237
Swenson D et al. Ovarian torsion: Case-control study comparing the sensitivity and specificity of ultrasonography and computed tomography for diagnosis in the emergency department. Eur J Radiol. 2014; 83(4):733-8. PMID: 24480106
White M, Stella J. Ovarian torsion: 10-year perspective. Emerg Med Australas. 2005; 17(3):231-7. PMID: 15953224





