
Author: Brit Long, MD (@long_brit, EM Attending Physician, San Antonio, TX) // Edited by: Alex Koyfman, MD (@EMHighAK)
Welcome to EM@3AM, an emDOCs series designed to foster your working knowledge by providing an expedited review of clinical basics. We’ll keep it short, while you keep that EM brain sharp.
A 53-year-old male presents with nausea, vomiting, decreased appetite, and complaints of turning “yellow”. He states this has worsened over 2 weeks, and his family asked him to be evaluated today. He denies history of abdominal pain, fever, alcohol use, or acetaminophen intake.
His vital signs are normal, and physical exam reveals icteric sclerae, jaundice of his face and chest, and hepatomegaly. He has no tenderness to abdominal palpation. Exam is otherwise normal.
What’s going on, and what’s your next step in evaluation and treatment?
Answer: Jaundice in an adult
Background: Jaundice is due to elevated serum bilirubin and yellow bilirubin pigment deposition. Patients often present with symptoms due to the underlying cause of the jaundice.
- Frequency and etiology of the condition varies, with over 52,000 ED visits per year for jaundice.
- Literature suggests the most frequent causes are ischemic liver injury, pancreatic/biliary carcinoma, gallstones, and alcoholic cirrhosis.
- Viral-induced and drug-related causes (acetaminophen) also account for a significant number.
- Normal serum bilirubin concentration is < 1 mg/dL, and jaundice is not usually detectable until 2.5 mg/dL.
Pathophysiology:
- 80% of bilirubin is due to RBC breakdown in the liver and spleen, which releases unconjugated bilirubin into the serum. This is bound to albumin and enters the liver, where it is conjugated.
- Conjugated bilirubin is stored in the gallbladder as bile, where it empties in the duodenum. Once in the colon, it is metabolized into stercobilin (excreted in the stool) or urobilinogen (excreted in the urine). Some of the conjugated bilirubin in the intestine is reabsorbed and returns to the liver.
- Conjugated bilirubin can also enter the serum through direct diffusion out of hepatocytes, most commonly occurring with obstruction.
- In normal circumstances, no bilirubin is excreted in the urine. If the renal system is overwhelmed with conjugated bilirubin, it will be present in the urine.
Etiologies
- Indirect hyperbilirubinemia: Due to bilirubin overproduction (hemolysis), decreased bilirubin uptake (CHF, portosystemic shunts, medications), and/or impaired conjugation (hyperthyroid, neonates, Crigler-Najjar or Gilbert syndrome, liver disease).
- Direct hyperbilirubinemia: Due to extrahepatic cholestasis/obstruction vs. intrahepatic causes.
- Extrahepatic: tumors, infection, cholangiopathy, pancreatitis
- Intrahepatic: chronic liver injury (cholangitis, medications, hepatitis, cirrhosis), multifactorial (TPN, infection, after surgery, sickle cell disease, transplantation), inherited/endocrine (pregnancy, thyrotoxicosis, benign recurrent cholestasis), infiltrative (amyloidosis, lymphoma, TB, sarcoidosis), and other (hypotension, CHF, Budd-Chiari syndrome)
History and Exam
- Life-threatening conditions with jaundice include cholangitis, hemolysis (massive), hepatic failure, acute fatty liver of pregnancy, acetaminophen overdose.
- Accurate history and exam are essential components of patient evaluation, as history and exam display an 86% sensitivity for determining intrahepatic versus extrahepatic disease.
- Patients may complain of nausea/vomiting, malaise, pruritis, weight changes, edema, and/or ascites.
- Ask about pain, fever, prior surgeries, time of onset, medications, herbal medications, alcohol/drug use, HIV history, travel, work, and family history.
- Exam must include vital signs (fever/hypotension – cholangitis), mental status, neurologic exam, presence of asterixis, lungs (crackles, pleural effusions), CV (evidence of heart failure), presence of ascites, abdominal tenderness (Murphy’s sign), hepatosplenomegaly, and skin.
- Jaundice is best seen in natural light, rather than fluorescent light. Predicting bilirubin level based on jaundice is inaccurate with poor interrater reliability. Evaluate the sclerae, conjunctiva, and intraoral region, which typically demonstrate jaundice before other sites.
Laboratory Assessment
- Obtain direct and indirect bilirubin. Unconjugated bilirubin is reported as indirect bilirubin, and conjugated as direct bilirubin. These are not exactly equivalent, as indirect bilirubin underestimates the actual unconjugated form, while direct bilirubin tends to overestimate the conjugated form.
- Other labs include CBC, liver function, ALP, albumin, GGT, coagulation panel, acetaminophen, lipase, albumin, and urinalysis.
- Elevation of ALP and GGT together suggest hepatobiliary disease.
- Elevation of liver function enzymes relative to ALP and GGT suggest intrahepatic etiology. Elevation of ALP and bilirubin relative to liver function suggest intrahepatic or extrahepatic disease.
- CBC is warranted to assess for abnormal WBC, Hgb/Hct, thrombocytopenia, and reticulocyte index.
- The liver is responsible for production of clotting factors, and PT/INR will elevate with significant hepatic dysfunction.
- Albumin serves as a marker of liver synthetic function.
- Lactate is warranted in toxic appearing patients; however, lactate is cleared through the liver.
- Acetaminophen level is warranted to assess for overdose.
- If hemolysis is a concern, obtain LDH, haptoglobin, peripheral smear, Coombs test.
- Hepatitis panel may be needed based on history and exam (Hep A/B/C, CMV, EBV, HSV, VZV).
Imaging:
- US: Warranted to assess gallbladder and biliary system. Evaluate common bile duct (CBD), as > 5 mm in patients < 50 years suggests obstruction. This measurement changes in the elderly and in patients post cholecystectomy or with liver transplant. A negative US cannot exclude choledocholithiasis (sensitivity 75%). If dilated CBD is present, further imaging is recommended.
- CT: Sensitivity 80% and specificity 99% for CBD stones. CT allows for evaluation of other abdominal organs, as well for the presence of a mass and staging of any tumors. CT can evaluate liver parenchyma, vasculature, and mass.
- HIDA: Useful in detection of cholelithiasis or cholecystitis if US is negative but clinical concern is present. However, it cannot diagnose complications of cholecystitis or evaluate for hepatic dysfunction.
- ERCP: Invasive procedure that visualizes the biliary tree and pancreatic ducts. Superior to CT and US for extrahepatic dysfunction and provides therapeutic options during the procedure.
- MRCP: Most sensitive noninvasive method for detecting biliary stones. Can be an alternative to ERCP in certain conditions (ductal tumor, periductal compression, choledocholithiasis).
- Which should you use? Concern for malignant obstruction = CT, gallstones or other benign obstruction = US. US is inconclusive = CT. CBD stone on imaging = ERCP. Sclerosing cholangitis or biliary stricture = MRCP.
Treatment: Dependent on underlying condition
- Transfer early to liver transplant center once diagnosis is made and the patient meets transplant criteria.
- Resuscitate first if patient is critically ill with IV fluids and antibiotics.
- Provide antiemetics and analgesics.
- Hemolysis: Transfusion for those with low Hbg/Hct and symptoms due to anemia. HUS/TTP = plasma exchange and corticosteroids.
- Extrahepatic obstruction: If cholangitis is present, provide antibiotics and consult for ERCP. For other conditions such as gallstone/stricture, obtain ERCP. For those with malignant mass, discuss with GI and surgery.
- Hepatocellular injury:
- Encephalopathy: Grade encephalopathy and treat based on this grade (lactulose, rifaximin)
- Coagulopathy: FFP for active bleeding. If not bleeding, no FFP is required. PCC should be considered for severe bleeding. Platelets may be needed for those with levels < 20,000/mm3.
- Antibiotics: Provide broad-spectrum antibiotics if toxic.
- Fluid resuscitate if in shock or hypotensive.
- Consider transplant: Use MELD score or King’s Criteria (https://www.mdcalc.com/meld-score-model-end-stage-liver-disease-12-older and https://www.mdcalc.com/kings-college-criteria-acetaminophen-toxicity).
- Acetaminophen overdose: Use Matthew-Rumack nomogram. If over toxic level/line, provide NAC (oral or IV). May require charcoal (< 1-2 hours from ingestion) and/or dialysis.
Special Situations in Adults
-
- Pregnancy: Jaundice can occur due to the previously mentioned conditions and several others such as hyperemesis gravidarum, intrahepatic cholestasis of pregnancy (3rd trimester, pruritis, cholestatic lab findings), infection (Hep E, HSV), acute fatty liver of pregnancy (3rd trimester, microvesicular fat in hepatocytes, N/V, RUQ pain, presents similar to HELLP).
- Post liver transplant: Discuss with transplant physician. Jaundice can be due to mechanical obstruction, infection, graft malfunction, rejection, drug toxicity, hepatic artery thrombosis.
From Dr. Katelyn Hanson and Hanson’s Anatomy:


A 68-year-old woman presents to the ED with complaint of fever and malaise. Her vital signs in triage are 39.2°C, HR 130, RR 32, and BP 92/60 mm Hg. On examination, she has notable jaundice of the frenulum of the tongue as well as scleral icterus. She is extremely tender to palpation in the right upper quadrant and is notably confused. Laboratory workup is remarkable for leukocytosis, transaminitis, and hyperbilirubinemia. What is the most likely diagnosis in this patient?
A) Cholangiocarcinoma
B) Cholangitis
C) Cholecystitis
D) Choledocholithiasis
Answer: B
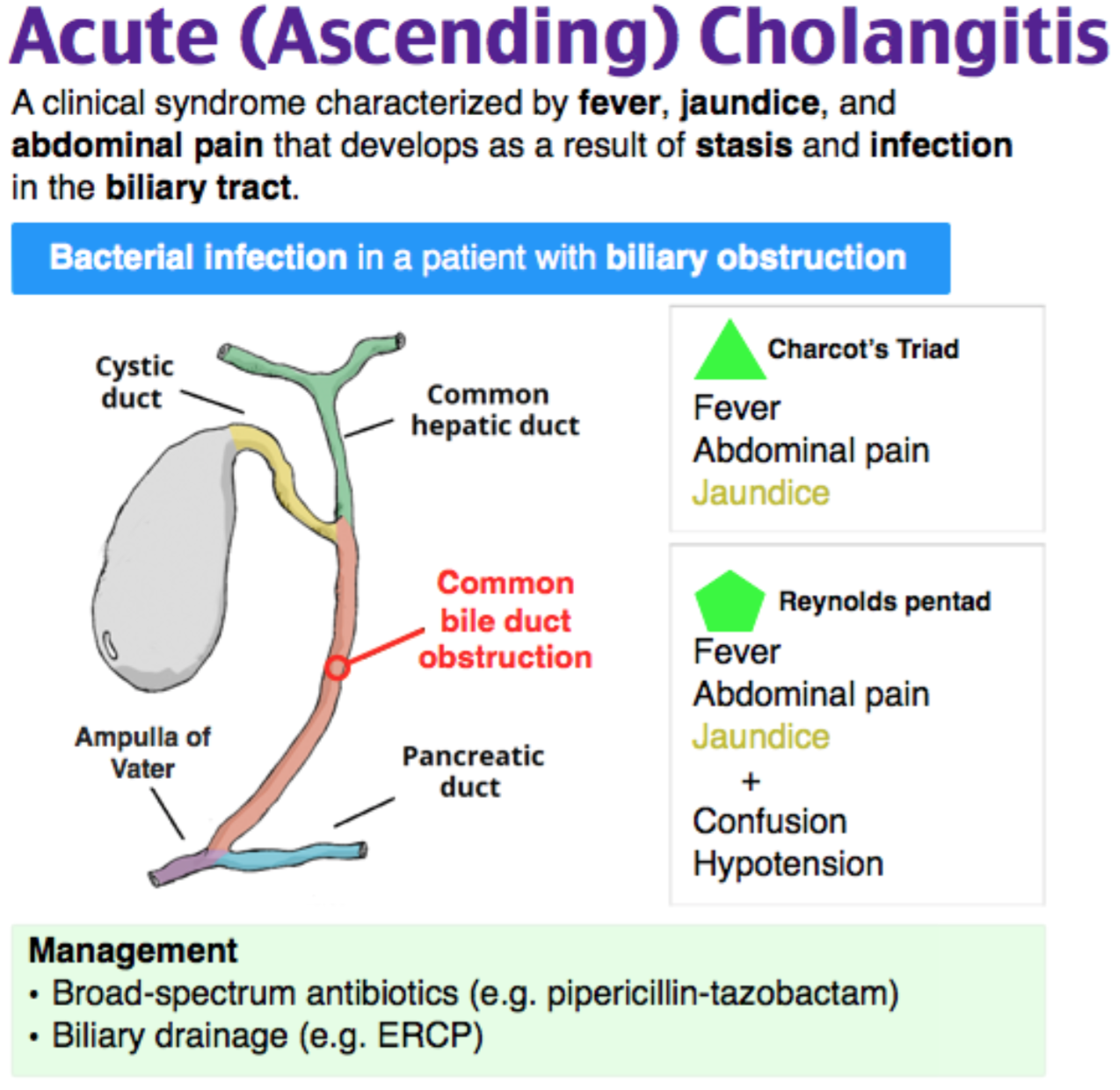
Cholangitis is a serious and often life-threatening infection of the biliary tree. It is typically caused by ascending infection from the gastrointestinal tract into the biliary tree in the setting of biliary stasis, such as in the case of an obstruction from a gallstone, stricture, or mass. More rarely, cholangitis can be seen in patients without an obstruction who develop biliary stasis secondary to total parenteral nutrition. Organisms commonly implicated in cholangitis include E. coli and enterococcus and bacteroides species. Charcot’s triad of fever, jaundice, and right upper quadrant abdominal pain is classically seen with cholangitis. In more severe disease, Reynolds’ pentad may be seen, with the addition of altered mental status and shock to the triad of symptoms named above. ED management of cholangitis includes prompt initiation of antibiotics and hemodynamic stabilization through fluid and vasopressor administration, as necessary. Surgical and gastrointestinal consultation are also important as emergent biliary decompression through ERCP or cholecystostomy placement may be necessary.
Cholangiocarcinoma (A) is a malignancy of the gallbladder. While it may cause obstruction leading to biliary stasis and ascending obstruction, in isolation, cholangiocarcinoma would not be expected to cause fever or hemodynamic compromise as seen in the patient above. Cholecystitis (C) is inflammation of the gallbladder, typically secondary to obstruction by a gallstone. Right upper quadrant pain and fever may be present as in cholangitis, but jaundice does not typically occur as seen in the patient above. Choledocholithiasis (D) refers to gallstones in the common bile duct. Transaminitis and pain are typically seen but fever, as in the patient above, is not.





