Originally published at CoreEM.net, dedicated to bringing Emergency Providers all things core content Emergency Medicine available to anyone, anywhere, anytime. Reposted with permission.
Follow Dr. Swaminathan and CORE EM on twitter at @EMSwami and @Core_EM
Written by Dr. Jacob Avila (@UltrasoundMD) and edited by Dr. Swaminathan.
Superficial Venous Thrombosis (SVT)
Definition: The presence of a clot in a superficial vein.
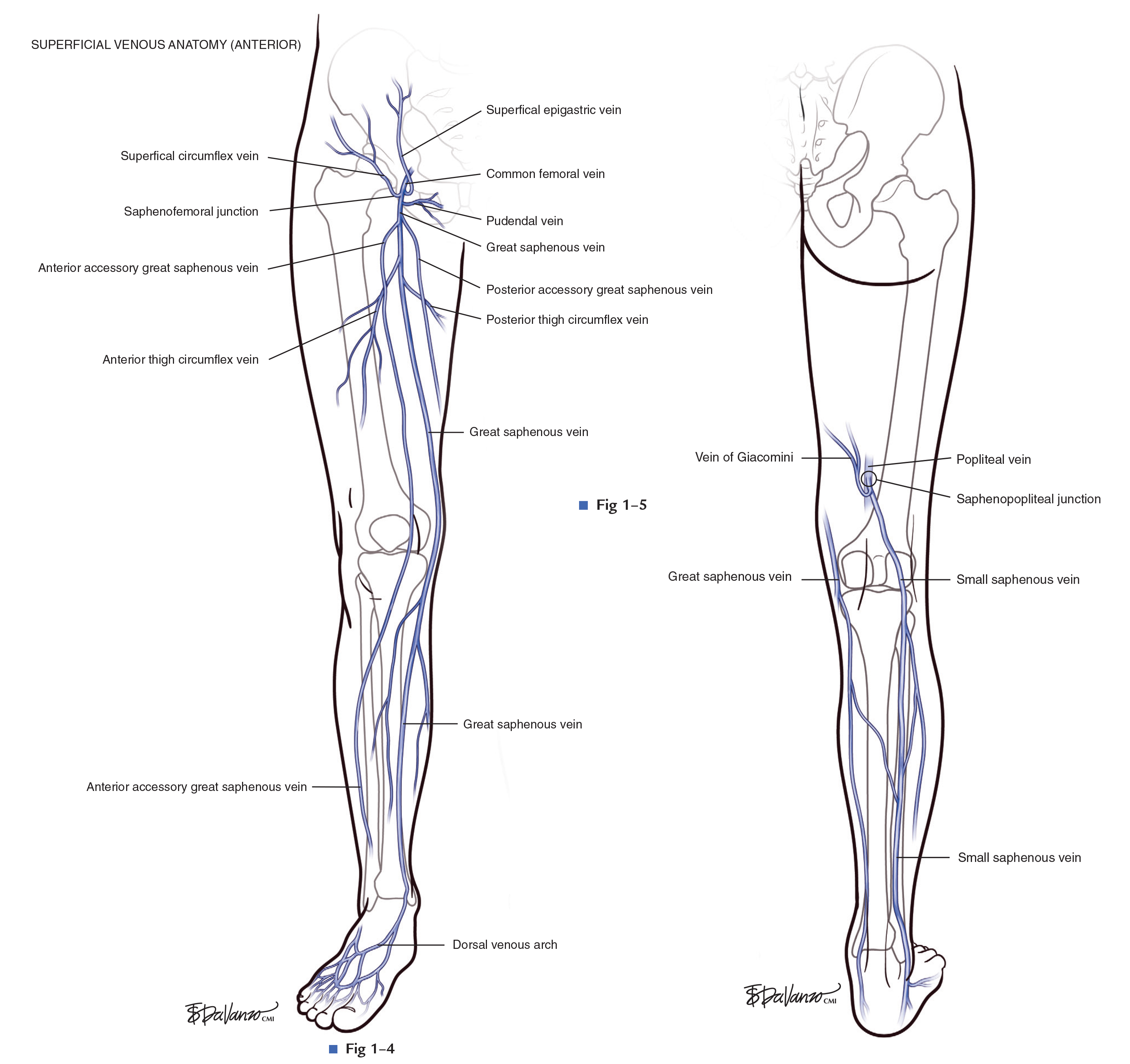
Lower Extremity Venous Anatomy (Atlas of Endovascular Venous Surgery)
Epidemiology:
- Although large prospective trials are lacking, superficial venous thrombosis (SVT) has been reported occur at a rate of 4 in 1000 per year in the US (Blumenberg 1998, Coon 1973)
- As a comparison, the incidence of venous thromboembolism (VTE) is estimated to occur in 1 in 1000 per year. (White 2003)
- The most common locations of SVT of the lower extremity are: (Cosmi 2015)
- Long saphenous vein – 50-60%
- Short saphenous vein – 11-15%
- Tributaries of the long/short saphenous – 30-40%
Pathophysiology, causes and risk factors:
- Vascular clots are caused by a combination of venous stasis, endothelial injury and hypercoagulability.
- Risk factors for the development of SVT are similar to those of VTE. (Cosmi 2015)
- Risk factors of complications of SVT (such as propagation of clot into deep veins) include male gender, history of VTE, cancer, SVT in a non-varicose vein, large SVT >5 cm, or SVT involving the sapheno-femoral junction (SFJ). (Bauersachs 2013)
Clinical Significance:
- SVT previously thought to be a benign disease entity (Cosmi 2015)
- However, subsequent studies have demonstrated that in patients with lower extremity SVT concomitant DVT and PE was seen in approximately 25% and 5% respectively. (Frappe 2014, Cosmi 2015)
- Half of the DVTs seen in SVT are non-contiguous and 17% of DVTs are seen in the contralateral limb. (Cosmi 2015)
Signs + Symptoms:
- Pain and redness to an area in the distribution of a superficial vein.
- Tendernesss of the vein may precede redness.
Diagnosis:
- Clinical diagnosis involves visualizing an area of redness and swelling and palpating a painful cord along the path of a vein.
- However, the clinical diagnosis of SVT can be unreliable and the extent of the SVT is often underestimated clinically. (Bauersachs 2013) Additionally, many other dermatologic conditions may mimic SVT (Cosmi 2015)
- The current objective test of choice is ultrasound demonstrating a non-compressible superficial vein, with or without echogenic thrombus inside of the vein.
Management:
- Due to the lack of large clinical trials evaluating the treatment of SVT, much of the literature relies heavily on expert consensus.
- Traditional treatment involves NSAIDS and stockings. This treatment is still recommended by most for SVT’s <5cm in length and >3cm from the SFJ. (Cosmi 2015)

- 2012 ACCP guidelines suggest that patients with SVT > 5 cm can be treated with prophylactic dose of fondaparinux or LMWH for 45 days. (Guyatt 2012)
- This recommendation was largely based on the CALISTO trial, which randomized 3002 patients with SVT to get either fondaparinux or placebo and reported that the rate of PE or DVT was 85% lower in the fondaparinux group (Decousus 2010)
- SVT within 3 cm of SFJ is considered by some to be equivalent to DVT and can be treated as such (Cosmi 2015)
- Topical NSAIDS may help symptoms and can be used at the same time as anticoagulation (Kearon 2012)
- There is no literature supporting or refuting using the same treatment in the evaluation of upper extremity SVT.
- If an SVT is uncovered in the lower extremity, a bilateral duplex ultrasound evaluating the deep venous system should be considered.
Take Home Points
- SVT >5cm or <3 cm from the SFJ should be treated with anti-coagulation.
- The rate of concurrent DVT and PE in patients with SVT is 25% and 5%, respectively.
Read More
References:
- Frappe P, et al the STEPH Study Group. Annual diagnosis rate of superficial-vein thrombosis of the lower limbs: the STEPH community-based study. J Thromb Haemost 2014; 12: 831–8. PMID: 24679145
- White RH. The epidemiology of venous thromboembolism. Circulation 2003; 107: I4–8. PMID: 12814979
- Blumenberg RM, et al.: Occult deep venous thrombosis complicating superficial thrombophlebitis. J Vasc Surg 1998, 27:338– 343. PMID: 9510288
- Coon WW et al. Venous thromboembolism and other venous disease in the Tecumseh Community Health Study. Circulation 1973;48:839–846. PMID: 4744789
- Cosmi B. Management of superficial vein thrombosis. Journal of thrombosis and haemostasis : JTH. 13(7):1175-83. 2015. PMID: 25903684
- Guyatt GH et al. Executive summary: Antithrombotic Therapy and Prevention of Thrombosis, 9th ed: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines. Chest. 141(2 Suppl):7S-47S. 2012. PMID: 22315257
- Decousus H et al. Fondaparinux for the treatment of superficial-vein thrombosis in the legs. The New England journal of medicine. 363(13):1222-32. 2010. PMID: 20860504
- Bauersachs RM. Diagnosis and treatment of superficial vein thrombosis. Hämostaseologie. 33(3):232-40. 2013. PMID: 23757000
- Kearon C, et al. Antithrombotic therapy for VTE disease: Antithrombotic Therapy and Prevention of Thrombosis, 9th ed: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines. Chest. 141(2 Suppl):e419S-94S. 2012. PMID: 22315268





1 thought on “CORE EM: Superficial Venous Thrombosis (SVT)”
Pingback: CORE EM: Superficial Venous Thrombosis (SVT) – Global Intensive Care