Author: Kristin E. Fontes, MD (Emergency Physician, Santa Barbara Cottage Hospital and Goleta Valley Cottage Hospital) // Edited by: Cynthia Santos, MD (Assistant Professor Emergency Medicine, Toxicology), Alex Koyfman, MD (@EMHighAK, EM Attending Physician, UTSW / Parkland Memorial Hospital), and Brit Long, MD (@long_brit, EM Attending Physician, San Antonio Military Medical Center)
Case presentation:
An obtunded 30-year-old man is brought to the emergency department by ambulance. He was picked up from a local hotel room where paramedics noticed various drug paraphernalia including needles, syringes, and plastic bags containing a white powdery substance. They reported pinpoint pupils and an initial respiratory rate of 5. He was given 2 mg of intramuscular naloxone twice prior to transport, and his breathing improved. After about 5 minutes, however, he again became obtunded. He is unable to provide any history on arrival to the ED.
Initial vital signs are: T 37C, HR 56, BP 100/70, RR 10, SpO2 88% (on 100% supplemental O2 via facemask)
On examination, the patient is pale and poorly responsive. He withdraws to deep sternal rub. He is bradypneic and has sonorous respirations. There are visible needle track marks predominantly over his left arm. He has no external signs of trauma.
The patient’s chart documents multiple previous ED visits involving heroin overdoses. Despite responding to 1 or 2 doses of intravenous naloxone during previous visits, you currently have to give repeat doses (0.4-1 mg increments) every 5-10 minutes due to recurrent respiratory depression. After multiple rounds of this, you start a continuous infusion of naloxone and admit him to the intensive care unit for continued management.
Questions:
- In what ways do novel synthetic opioids contribute to drug overdose mortality rates in the United States?
- What is the relative potency of fentanyl and its derivatives?
- How should naloxone be administered, and how should health care personnel protect themselves?
Pearls:
- Novel synthetic opioids (NSOs) include fentanyl derivatives and newly emerging non-fentanyl compounds, often referred to as “designer opioids.” Together with illicitly produced fentanyl, these drugs have caused a recent spike in overdose deaths, whereas deaths from prescription opioids are stabilizing.[1-3]
- The most recent CDC data demonstrate that during 2014-2015, death rates involving synthetic opioids (other than methadone) increased in both genders and all racial/ethnic groups. While mortality from heroin and semi-synthetic opioids increased as well (20.6% and 2.6%, respectively), the greatest rise was noted with synthetic opioids (72.2%).[2]
- Most fentanyl-associated deaths are due to illicitly manufactured fentanyl, rather than prescription drug diversion.[3]
- Whereas synthetic opioids can also include less potent opioids like loperamide, diphenoxylate, and methadone, the focus of this post is on fentanyl and its derivatives.
- Fentanyl and its derivatives are highly lipophilic and thus rapidly distribute into the central nervous system, which leads to their high potency, rapid onset, and short duration of action; they act primarily as mu-opioid receptor agonists.[4]
Table 1. Relative potency, duration of action, and states reporting mortality from fentanyl and select novel synthetic opioids. [3-5]
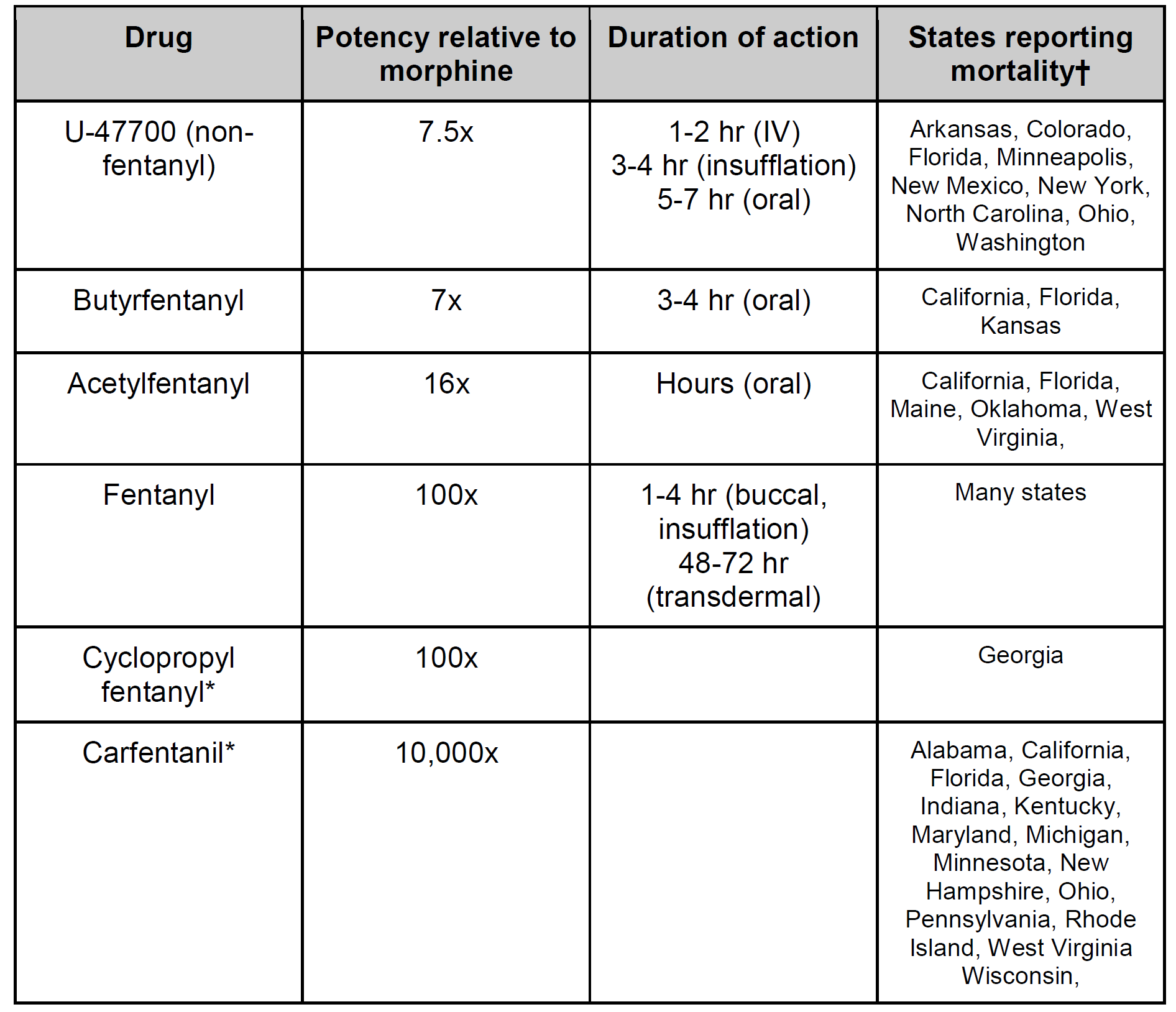
- *The pharmacokinetics of these novel drugs are not yet fully described in the literature, and these agents are not intended for human use. Carfentanil is approved for veterinary use for sedation of large animals.
- †This list may not be complete, as the spread of novel synthetic opioids is growing faster than published literature on this topic.
- Other novel synthetic opioids that have been reported include: 4-Fluorobutyrylfentanyl, Furanylfentanyl, Ocfentanil, AH-7921, and MT-45.[5]
- Fentanyl and its derivatives are commonly found as substitutes/adulterants in other preparations.
Considerations regarding counterfeit pill production:
- Fentanyl and derivatives are relatively inexpensive, influencing distributors and dealers to choose these over heroin as substitutes/adulterants.
- Users may be unaware that they are purchasing counterfeit pills, which are often identical in appearance to legally prepared pills.
- Inconsistent synthesis methods lead to varying drug concentrations in individual pills.
Considerations for healthcare providers due to relative high potency of synthetic opioids:
- Toxicity from fentanyl and derivatives may require very high doses of naloxone for reversal.
- Dermal or inhalational exposure may lead to symptom development in first responders; appropriate personal protective equipment must be used.
Naloxone tips when treating fentanyl and novel synthetic opioid exposures:
- High doses of naloxone may be needed for potent synthetic opioids so quickly escalate naloxone dosing if there is no response. (see http://www.emdocs.net/tox-cards-narcan-naloxone/). Keep in mind patients may require doses of naloxone higher than doses typically needed with other types of opiates (e.g. morphine, codeine), semi-synthetic opioids (e.g. hydromorphone, heroin), and synthetic opioids (e.g. methadone).
- Some recommend to forgo the initial low starting dose and start with 2 mg of naloxone if the use of fentanyl and novel synthetic opioids are suspected.[3]
- Retrospective chart review of fentanyl overdoses in Chicago in 2005-2006 reported a mean dose of 3.36 milligrams IV required for rescue (no withdrawal symptoms reported); dose range was 0.4-12 mg.[6] During fentanyl overdose outbreaks, patients have required up to 14 mg of naloxone to reverse CNS and respiratory depression.[7]
Protective Personal Equipment:
- There have been multiple reports of nurses and first responders becoming symptomatic and requiring Naloxone after dermal and inhalational exposure from exposure of the powdered form of fentanyl or fentanyl derivatives.[7,8]
- Fentanyl and novel synthetic opioids in the white powder form may put first responders at risk through inhalation of airborne particulate, contact via mucous membranes or possibly through skin contact. Exposure to carfentanil in particular can be risky for first responders since as little as a few grains of salt can result in respiratory depression.[7]
- If the presence of highly potent synthetic opioids are suspected, health care personal should use nitrile gloves, eye protection, and respiratory protection, with escalation to other types of PPE as situationally indicated.[7,8]
Complications from synthetic opioid toxicity:
- Rapid death after intravenous fentanyl abuse may be due to chest wall rigidity; mechanism poorly understood but may be related to central dopaminergic activity.[9,10]
- Pulmonary hemorrhage resulting in hypoxic respiratory failure has been reported after fentanyl and butyrfentanyl abuse; mechanism is unknown.[11]
- Serotonin syndrome has been reported after fentanyl use in patients concomitantly taking other serotonergic agents.[12]
Key Points:
- Potent synthetic opioids like Fentanyl and novel synthetic opioids (especially carfentanil) are associated with recent increased mortality from opioid abuse; users are often unaware of what they are consuming.
- Higher doses (e.g. exceeding 10 mg) of naloxone may be required for rescue from these potent synthetic opioids.
- Health care personal should use nitrile gloves, eye protection, and respiratory protection if there is high suspicion of the powdered form of these potent synthetic opioids, with escalation to other types of PPE as situationally indicated.
References:
- DEA issues carfentanil warning to police and public. https://www.dea.gov/divisions/hq/2016/hq092216.shtml (September 22, 2016)
- Rudd RA, Seth P, David F, Scholl L. Increases in drug and opioid-involved overdose deaths – United States, 2010-2015. MMWR Morb Mortal Wkly Rep 2016 Dec 30;65(5051):1445-1452.
- Prekupec MP, Mansky PA, Baumann MH. Misuse of novel synthetic opioids: a deadly new trend. J Addict Med 2017 Jun 5 [Epub ahead of print].
- Zawilska JB. An expanding world of novel psychoactive substances: opioids. Front Psychiatry 2017 Jun 30;8:110.
- Mohr A, Friscia M, Papsun D, Kacinko S, et al. Analysis of Novel Synthetic Opioids U-47700, U-50488 and Furanyl Fentanyl by LC–MS/MS in Postmortem Casework, Journal of Analytical Toxicology 2016. 40(9):709–717.
- Schumann H, Erickson T, Thompson TM, Zautcke JL, Denton JS. Fentanyl epidemic in Chicago, Illinois and surrounding Cook County. Clin Toxicol 2008 Jul;46(6):501-6.
- Lybeck A, Colella R. Synthetic Opioid Overdose: Practical Considerations for Emergency Medical Services. Evidence-based EMS. Available at: http://www.naemsp-blog.com/emsmed/2017/6/15/synthetic-opioid-overdose-practical-considerations-for-emergency-medical-services
- Centers for Disease Control. Fentanyl: Preventing Occupational Exposure to Emergency Responders. Available at: www.cdc.gov/niosh/topics/fentanyl/risk.html.
- Burns G, DeRienz RT, Baker DD, Casavant M, Spiller HA. Could chest wall rigidity be a factor in rapid death from illicit fentanyl abuse? Clin Toxicol (Phila) 2016 Jun;54(5):420-3.
- Coruh B, Tonelli MR, Park DR. Fentanyl-induced chest wall rigidity. Chest 2013 Apr;143(4):1145-1146.
- Ruzycki S, Yarema M, Dunham M, Sadrzadeh H, Tremblay A. Intranasal fentanyl intoxication leading to diffuse alveolar hemorrhage. J Med Toxicol 2016 Jun;12(2):185-8.
- Gaffney RR, Schreibman IR. Serotonin syndrome in a patient on trazodone and duloxetine who received fentanyl following a percutaneous liver biopsy. Case Rep Gastroenterol 2015 May 6;9(2):132-6.





1 thought on “Tox Cards: Novel Synthetic Opioids”
Pingback: Länkar v49-50 | Internmedicin