Authors: Courtney Cassella, MD (@Corablacas, EM Resident Physician, Icahn SoM at Mount Sinai) // Edited by: Alex Koyfman, MD (@EMHighAK, EM Attending Physician, UT Southwestern Medical Center / Parkland Memorial Hospital) and Brit Long, MD (@long_brit, EM Attending Physician, San Antonio, TX)
Clinical Case:
A 34-year-old woman presents to the emergency department referred by her employee health services for hypertension. The patient was getting her yearly physical for work health clearance. In the office her blood pressure was 187/104. She was referred immediately to the emergency department. Review of systems was negative including headaches, chest pain, shortness of breath, abdominal pain, or urinary complaints. On physical exam her blood pressure is 174/98 but otherwise unremarkable. The patient was discharged with primary care follow-up.
In the ED, we see patients with asymptomatic hypertension who are frequently discharged with primary care follow-up. This post opens a brief discussion and opportunity for learning about an instance where asymptomatic hypertension requires urgent action, hypertension in pregnancy.
What if this patient was 2 weeks post-partum?
*Note: this post is not comprehensive. For a full review of preeclampsia and eclampsia see this emDocs post by Derek Marcantel: http://www.emdocs.net/preeclampsia-and-eclampsia-common-pitfalls-in-diagnosis-and-management/
When do you have to worry about preeclampsia? 1
- > 20 weeks to 4 weeks postpartum
- It is important to note that preeclampsia and eclampsia can occur 4 weeks postpartum
- Definition
- Hypertension (SBP >140 mmHg or DBP >90 mmHg) AND
- New onset proteinuria, sudden increase in proteinuria, or end-organ dysfunction (HELLP syndrome)
- After 20 weeks gestation
- Severe preeclampsia (one or more criteria) 1
- SBP >160 mmHg or DBP >110 mmHg
- Proteinuria of 5 g or higher in 24-hour urine specimen or 3+ or greater on two random samples 4 hours apart
- Renal insufficiency
- Oliguria <500 mL in 24 h
- Creatinine >1.1mg/d or doubling serum concentration
- Cerebral or visual disturbances
- Pulmonary edema or cyanosis
- Impaired liver function
- Manifests as epigastric or RUQ pain
- Transaminitis 2X normal
- Thrombocytopenia
- Fetal growth restriction
What, if any work-up would you pursue in this patient? What do you need to diagnose preeclampsia?3,4
- Patients with preeclampsia may have asymptomatic hypertension. This is one population where laboratory evaluation is essential in the evaluation.
- *Correlate: Women of child bearing age presenting with asymptomatic hypertension should be evaluated for pregnancy or if they are post-partum
Workup
- Urinalysis – proteinuria (≥1+ protein on urinalysis)
- Formal diagnosis is >300 mg/24 hour urine collection
- CMP – electrolytes, renal function, hepatic function
- CBC – thrombocytopenia, smear may show schistocytes
- Magnesium – baseline level for treatment
- Head CT if new onset seizure or focal neurologic exam
- Fetal monitoring
What blood pressure medications would you use for preeclampsia? What is the management of preeclampsia?1,2
- First, always consult OB/GYN
Mild preeclampsia – Asymptomatic
- PO anti-hypertensive medications
- Although often initially managed inpatient, can be managed as an outpatient with close obstetric follow-up.

* Table is a brief summary of starting doses
Severe preeclampsia
- Stabilize – ABCs, IV access, left lateral decubitus position
- Goal: Decrease of blood pressure ≤ 20 mmHg. Do not attempt to lower to “normal” as this will decrease perfusion to the fetus
- Start magnesium sulfate prophylaxis
- Definitive treatment is delivery of the fetus

- Labetalol is a first-line agent. Contraindications: asthma, heart disease, CHF
- Hydralazine is associated with maternal hypotension, HA, fetal distress
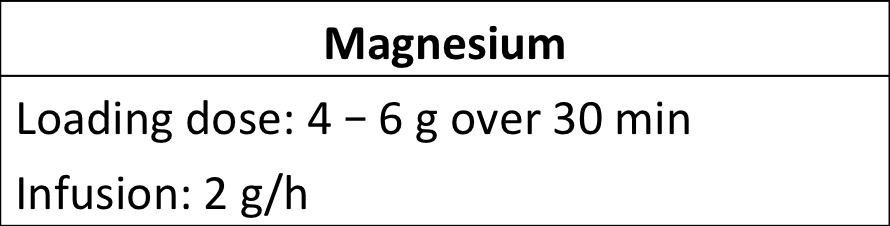
- Reduce loading dose to 2 g in renal insufficiency.2
- Monitor for toxicity: decreased deep tendon reflexes, respiratory depression
References
- American College of Obstetricians and Gynecologists. Committee on Practice Bulletins-Obstetrics. Diagnosis and management of preeclampsia and eclampsia. Obstet Gynecol. 2002;99:159–167.
CrossRef [PubMed: 16175681]
- American College of Obstetrics and Gynecology Task Force on Hypertension in Pregnancy. Hypertension in Pregnancy. ACOG Practice Guideline. 2013:1-79. https://www.acog.org/Resources-And-Publications/Task-Force-and-Work-Group-Reports/Hypertension-in-Pregnancy. Accessed December 01, 2017.
- Young J. Maternal Emergencies After 20 Weeks of Pregnancy and in the Postpartum Period. In: Tintinalli JE, Stapczynski J, Ma O, Yealy DM, Meckler GD, Cline DM. eds.Tintinalli’s Emergency Medicine: A Comprehensive Study Guide, 8e New York, NY: McGraw-Hill; 2016. http://accessemergencymedicine.mhmedical.com.eresources.mssm.edu/content.aspx?bookid=1658§ionid=109431050. Accessed December 01, 2017.
- Wittels KA. Preeclampsia and Eclampsia. In: Sherman SC, Weber JM, Schindlbeck MA, Rahul G. P. eds. Clinical Emergency Medicine, 1e New York, NY: McGraw-Hill; 2014. http://accessemergencymedicine.mhmedical.com.eresources.mssm.edu/content.aspx?bookid=991§ionid=55139157. Accessed December 01, 2017.




