Originally published at EM Cases – Visit to listen to accompanying podcast. Reposted with permission.
Follow Dr. Anton Helman on twitter @EMCases
You probably can’t remember the last time you worked a shift in the ED and didn’t see at least one patient with an ankle injury. While almost all of these patients are relatively straightforward to diagnose and manage a small but significant minority of these patients will have a more elusive diagnosis, that if not identified early, could lead to significant morbidity. On the flip side, if we’re super conservative and defensive and we immobilize everyone with an ankle injury no matter how minor we’re not doing our patients or our consultants any favors either.
With the help of Canada’s leading ED-ortho educator Arun Sayal, the brains behind The CASTED Course, and Hossein Mehdian, an Orthopedic surgeon at North York General, we cover a general way of thinking about ankle injuries, the limitations of the Ottawa Ankle Rules, a simplified approach to the ankle x-ray, the importance of identifying an external rotation mechanism of injury and much more…
Podcast production, sound design & editing by Anton Helman
Written Summary and blog post by Shaun Mehta, edited by Anton Helman January, 2018
Cite this podcast as: Helman, A, Sayal, A, Mehdian, H. Commonly Missed Ankle Injuries. Emergency Medicine Cases. January, 2018. https://emergencymedicinecases.com/commonly-missed-ankle-injuries/. Accessed [date].
Don’t short change the history and physical for ankle injuries!
We would not short change a patient with chest pain by taking a poor history. The same should apply to ankle injuries. It is best that we see and examine our patients first and then look for pathology on the x-ray, rather than the other way round, as often happens on busy shifts. Here are some useful pearls for the H&P to help distinguish the simple lateral ankle sprain or fracture from a more sinister injury.
History
The key here is mechanism, mechanism, mechanism.
- What was the direction of force applied?
- What was the height of the fall?
- What was the direction the foot turned?
- What happened afterward (i.e. weight bearing status)?
There are also certain red flags for serious injuries not to be missed:
- The patient reports an external rotation mechanism – consider this the “thunderclap headache” or “chest pain radiating to the back” of the ankle.
- The patient is not weight bearing at all.
Don’t forget the PMHx here.
- Has the ankle been injured before?
- What is the functional status of the unaffected limb?
- Are there any sensory deficits from diabetes, recent back surgery or chronic alcoholism?
External rotation mechanism of ankle injuries should be considered a red flag as the “thunderclap” headache is for subarachnoid hemorrhage.
Physical
Do not limit your assessment to where the Ottawa Ankle rules guide you.
Pitfall: Using the Ottawa Ankle Rules to guide your physical exam of a patient with an ankle injury.
A few key physical exam maneuvers to do on all patients with ankle injuries:
- Remember the ankle exam starts at the knee. Work your way down the entire fibula looking for tenderness. However, don’t be satisfied that the absence of tenderness there rules a Maisonneuve or Dupuytren’s fracture.
- Palpate the anterior aspect of ankle joint for clues of a syndesmosis injury or talus fracture
- Squeeze proximal to the ankle joint looking for pain at the syndesmosis indicative of a syndesmosis injury
Pearl: Ischemia as a result of an isolated ankle fracture is very rare. If you find signs of ischemia in the foot, examine proximally to assess for additional injuries.
Closed Ring System: A simple approach to assessing ankle injuries stability

The commonly cited Weber classification system is cumbersome and impractical for ED use. In the Closed Ring Classification System the ankle is thought of as a ring of bone and ligaments surrounding the talus consisting of the tibia, the medial malleolus and medial deltoid ligaments, the fibula and lateral ligaments and calcaneus.
A single disruption in the ring allows stability to be preserved. Two disruptions portends instability and will likely cause the joint to shift.
There are notable exceptions to this system:
- Lateral malleolus fracture even with no medial injury may become unstable.
- Isolated syndesmosis injury
Approach to ankle injuries x-ray interpretation
There are many great resources that help walk you through good approaches to the ankle x-ray. Here is an excellent EM focused summary.
Remember that the ankle joint is very sensitive to even the slightest deviation. A shift of even 1mm can result in disruption of the ankle mechanics with downstream arthritis and gait disturbance.
Ensure a mortise view in addition to the standard AP and lateral views.
To make reading these images efficient, concentrating on ankle stability, focus on a few key areas:
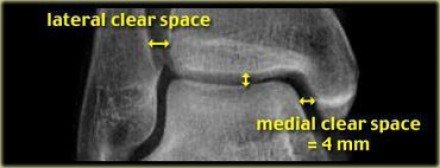
Talar shift: look to make sure there is congruence between the clear space on either side of the talus; measure the medial clear space and the lateral clear space. If they are incongruent or the medial clear space is >4mm the ankle is likely unstable.
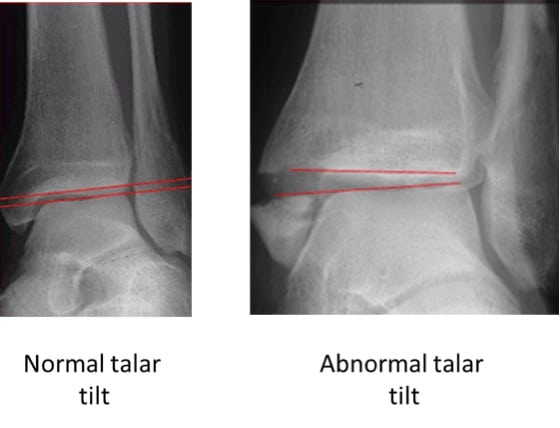
Talar tilt: The lines in red below should be parallel. Talar tilt indicates an unstable ankle.
 Tibio-fibular clear-space: Measure the gap between the tibia and fibula 1cm proximal to the tibial plafond on both the AP view and mortise view. They should be <6mm. If >6mm, suspect a syndesmosis injury.
Tibio-fibular clear-space: Measure the gap between the tibia and fibula 1cm proximal to the tibial plafond on both the AP view and mortise view. They should be <6mm. If >6mm, suspect a syndesmosis injury.

Tibio-fibular clear space
Specific Ankle Injuries: Nuances of Diagnosis & Management
The isolated Weber B fracture: Controversial management
A Weber B fracture is an oblique lateral malleolus fracture at the level of the talar dome.

While Weber B fractures associated with any suspicion for medial or deltoid ligament injury should be made non-weight bearing in a back slab, there are two ED management options for isolated Weber B fractures without any suspicion for medial involvement.
- Backslab, non-weight bearing or
- Place the patient in a foam boot without crutches (have them weight bearing as tolerated) and have them
 follow up in a week in the orthopedic clinic. At that time they’ll “declare themselves” as either remaining stable (so you’ve saved them having to be completely immobilized) or they’ll shift on weight-bearing views and become unstable requiring surgery. Just be sure to warn them that this might happen.
follow up in a week in the orthopedic clinic. At that time they’ll “declare themselves” as either remaining stable (so you’ve saved them having to be completely immobilized) or they’ll shift on weight-bearing views and become unstable requiring surgery. Just be sure to warn them that this might happen.
Note that in our experts’ opinion, ultrasound does not play a role in assessing the integrity of the deltoid ligament in the ED to help make decisions about the stability of Weber B fractures.
High ankle sprain: The isolated syndesmosis injury

Ligaments of the ankle. Note the location of the distal tibiofibular syndesmosis.
A high ankle sprain is an isolated distal tibiofibular syndesmosis injury (not a severe lateral ankle sprain). They are missed in 20% of ED cases. The syndesmosis ligaments stabilize the ankle mortise so that an injury to the syndesmosis may result in an unstable ankle injury.
Any patient who refuses to weight bear, with anterior ankle pain, and a mechanism of external rotation with ankle dorsiflexion should be considered to have a syndesmosis injury until proven otherwise. Consider this injury in sports where players wear a boot (eg. hockey, snowboarding, etc.) that generally prevents typical lateral ankle sprains.
Physical Exam Pearls for syndesmosis injury:
Toe walking to prevent painful dorsiflexion.
Squeeze/Hopkin’s test – 94% specific, 30% sensitive
Squeeze tibia/fibula together at mid-calf level and assess for pain at syndesmosis distally near the talus.
External rotation test – 85% specific, 20% sensitive
Stabilize the leg with the hip and knee flexed to 90 degrees. Holding the patient’s foot and externally rotating it with a small amount of dorsiflexion will elicit pain at the syndesmosis.
Why is it important to pick up a syndesmosis injury clinically?
- Needs an X-ray: assess tibiofibular clear space (see above under x-ray interpretation) for stability, rule out commonly associated fractures (proximal fibula, medial malleolus)
- Treatment Δ: splint, non-weight-bearing, f/u fracture clinic
- Prognosis Δ: return to activity 4-6 months
Tillaux fracture
A Tillaux fracture is an intra-articular Salter-Harris class III fracture of the distal tibia with avulsion of the anterolateral tibial epiphysis.
Tillaux fractures occur in children whose growth plates are not fully closed (ages 11-15). Remember that in children, the ligaments tend to be stronger than the growth plate. Tillaux fractures can be considered “the syndesmosis injury of children” because the clinical presentation is similar. As in syndesmosis injuries, be concerned in the patient who is refusing to weight bear, with anterior ankle pain, and the mechanism was external rotation. Tillaux fractures often occur as a result of a low energy mechanism.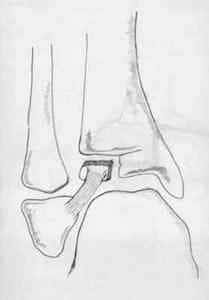
Signs of Tillaux fracture:
- Swelling over anterior aspect of distal leg and ankle
- Presence of bruising or ecchymosis
- External rotation deformity of the foot (severe injuries)
- Possible tenderness over the medial malleolus or deltoid ligament
Maisonneuve and Dupuytren’s fractures
Maisonneuve and Dupuytren’s fractures are Weber C spiral fractures of the proximal third and middle third of the fibula respectively.

Medial ankle injury with medial clear space widening associated with Masonneuve fracture.
Again, the mechanism of injury for these fractures is external rotation of the ankle.
These fractures are commonly missed 2nd fractures, and this is why your ankle exam starts at the proximal fibula and includes the entire length of the fibula. Possible associated injuries include a medial malleolus fracture, deltoid ligament rupture, syndesmosis injury or posterior malleolus fracture. Be suspicious of a fibula fracture if the medial clear space is > 4 mm. The fibula may not be tender. Either way, consider a full tib-fib x-ray to rule out a Masonneuve or Dupuytern’s fracure for all patients with suspected medial ankle injuries.
Pearl: For all medial ankle injuries consider tib-fib x-rays to rule out an associated fibula fracture, regardless of whether or not the patient is tender along the fibula.
Both Maisonneuve and Dupuytren’s injuries are unstable injuries and require the patient to have a splint, be non-weight-bearing, and see an orthopedic surgeon. Immobilization in a below-knee posterior slab and crutches is acceptable according to our experts.
The most commonly missed fracture is the 2nd fracture.
Snowboarder’s fracture

Lateral process of the talus fracture also known as a snowboarder’s fracture
A snowboarder’s fracture is a lateral process of talus fracture that is commonly misdiagnosed as a simple ankle sprain. Yet again, the mechanism of injury is external rotation of the ankle usually associated with dorsiflexionand an axial load upon landing. The talus is an often overlooked bone on physical exam. Just as we are trained to assess the scaphoid bone for occult fracture for all wrist injuries we should assess the talus bone for occult fracture for all ankle injuries. Get a good mortise view of your ankle to pick up this fracture, which can be very subtle or occult on x-ray. If in doubt on your x-ray, place the patient in a posterior slab, non-weight-bearing and have them follow in up fracture clinic. If available, get a CT ankle.
The talus is the “scaphoid bone of the ankle”. Make sure to always assess the talus on physical exam of the ankle.
Common situations in which talus fractures are missed:
- Patients who injured their ankle in a boot/skate
- Patients in an MVC with distracting injuries
- Older patients with osteoporosis
- Patients diagnosed with ankle sprain returning weeks later with ongoing pain
Important ‘can’t miss’ ankle sprain mimics
- Syndesmosis injuries
- Tillaux fracture
- Snowboarder’s fracture
- Achilles tendon rupture
Take home points for commonly missed ankle injuries
- Eversion/External rotation mechanism = red flag for syndesmosis, talus, tillaux, deltoid, Maisonneuve and Dupuytren’s injuries that may require surgery.
- The Ottawa Ankle Rules should not be used a guide for your physical exam of a patient with an ankle injury.
- Anterior ankle pain/tenderness should raise the possibility of a syndesmosis high ankle sprain injury or tillaux fracture.
- Always examine the medial ankle to assess not only for medial malleolus but also for deltoid ligament injuries.
- If any medial tenderness, examine the entire fibula for a Maisonneuve or Dupuytren’s fracture and order a tib-fib x-ray.
- The talus is the “scaphoid bone of the ankle”. Make sure to always assess the talus on physical exam of the ankle. If the x-ray is not giving an answer, a CT is a reasonable next step.
For more on MSK Injuries & Trauma download our free eBook: EM Cases Digest Vol. 1 MSK & Trauma




