Author: Alexander M. Mozeika, PharmD, MS3 Rutgers New Jersey Medical School // Editor: Cynthia Santos, MD (@CynthiaSantosMD, Assistant Professor, Emergency Medicine, Medical Toxicology, Rutgers NJMS); Alex Koyfman, MD (@EMHighAK); Brit Long, MD (@long_brit)

Case 1:
A 53-year-old man presents 45 minutes after a suicide attempt. He ingested 100 tablets of an unknown medication. Initial evaluation reveals:
- Vitals: T 37.2, HR 92, BP 180/84, RR 26, SpO2 99% on RA
- ABG: pH 7.41, pCO2 26, HCO3 16
- Anion gap: 24
Questions:
- What are the pharmacokinetic factors of absorption?
- How are these factors altered in the setting of toxicology (i.e. toxicokinetics)?
- What are treatment options for gastric decontamination?
Background:1-3
- Absorption is the process by which a xenobiotic enters the body.
- The rate and extent of absorption is determined by:
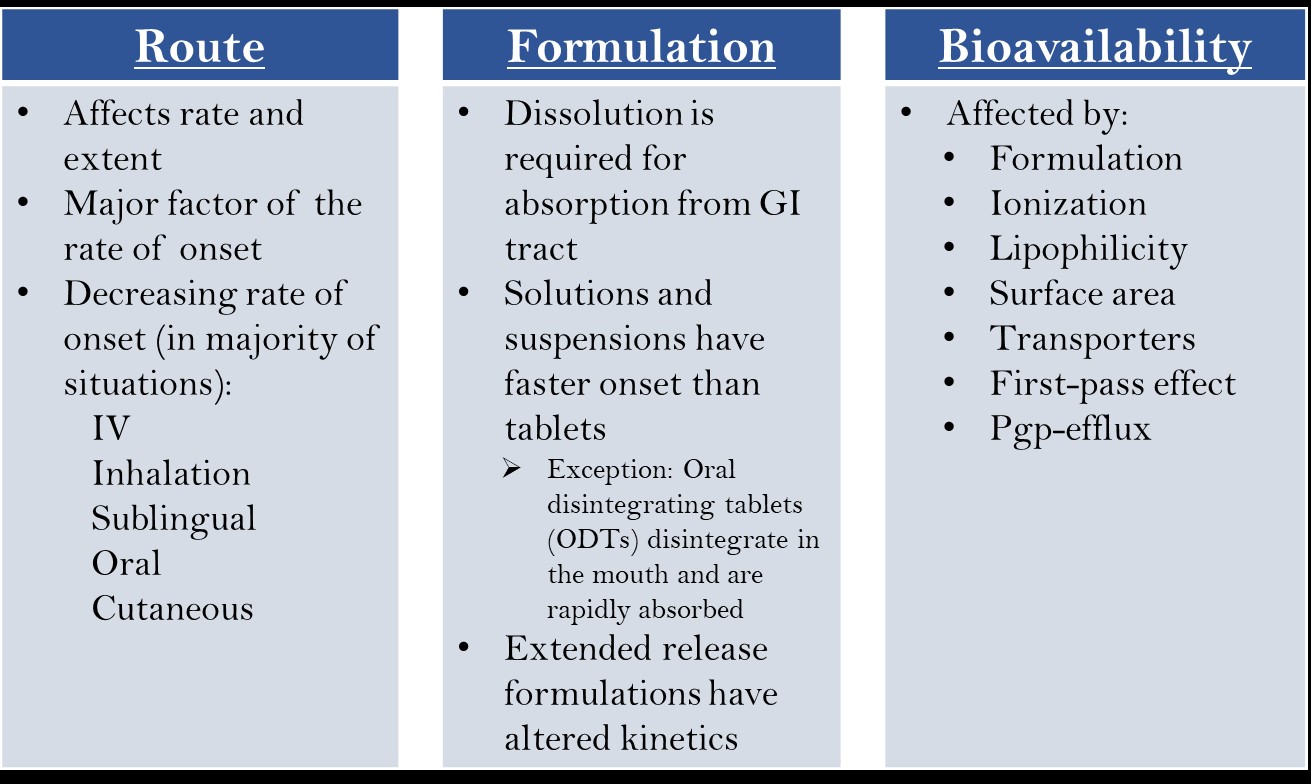
Toxicokinetics of Intracellular Absorption:1-4
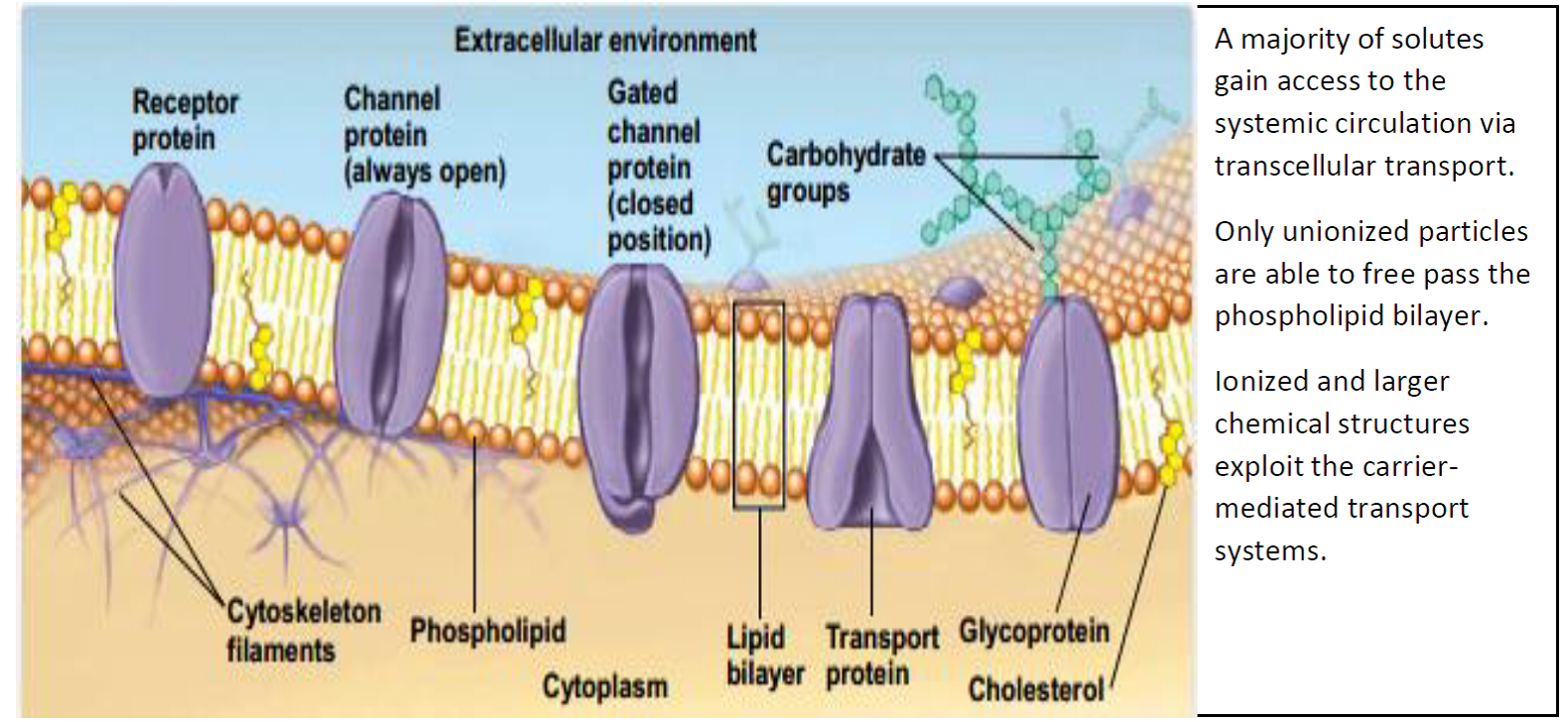
Image: Cells and Tissues. In: Marieb EN, ed. Human Anatomy & Physiology. 5th ed: Benjamin-Cummings Pub Co; 2001.
- Numerous drug formulations exist, each with different disintegration and dissolution properties.
- Delayed-released or enteric-coated tablets have prolonged onsets of absorption and unpredictable kinetic profiles.
- Ionization status of xenobiotics affects the location and extent of absorption.
- Only unionized molecules can cross the phospholipid bilayer.
- The Henderson-Hasselbach equation can be used to describe the ratio of ionized to unionized molecules at a particular pH.
Case 1 (continued):
Patient was found to have an initial ASA level of 32.5 mg/dL. Urinary alkalinization was started to decrease renal tubular reabsorption through “ion trapping”.
Ion Trapping:
- Pharmacological concept that relies on acid-base biochemical properties.
- Only unionized molecules can cross the phospholipid bilayer.
- Henderson-Hasselbach equation:
-
- pH = pKa + = pKa +
- (algebraically rearranged)
- Ionization state can be exploited and used therapeutically (i.e. urine alkalization traps ionized weak-acid chemical moieties in urine).
- Example:
- In Case 1 (see above), urine alkalinization is initiated with sodium bicarbonate to achieve a urinary pH of 7.5 to decrease the renal tubular absorption of salicylate, which has a pKa of 3.5.
- At pH of 3.5, then [A–]/[HA] = 100 = 1
- At pH of 7.5, then [A–]/[HA] = 104 = 10,000
- In Case 1 (see above), urine alkalinization is initiated with sodium bicarbonate to achieve a urinary pH of 7.5 to decrease the renal tubular absorption of salicylate, which has a pKa of 3.5.
- Weak Acids:
- If the pKa < pH of the environment, the conjugate base (anion) form of the species will predominate. Example = CH3COO–
- If the pKa > pH of the environment, the environment is more acidic, and the acidic (neutral) form will predominate. Example CH3COOH
- Example: Weak acids (NSAIDS, salicylates) tend to be absorbed in acidic environments, such as the stomach.
- Weak Bases:
- If the pKa < pH of the environment, the environment is more basic, and the species will remain in the neutral form. Example = NH3
- If the pKa > pH of the environment, the environment is more acidic, and the species will accept an extra H+, and the base will exist in its cation form. Example = NH4+
- Example: Weak bases tend to be absorbed in basic environments, such as the duodenum. Drug users may ingest amphetamines (a weak base) with basic substances (e.g. Maalox) to increase absorption of the amphetamines and enhance their “high”.
Case 1 (continued):
Repeat ASA concentrations were 40.7, 40.7, and 45 mg/dL at 6, 11, and 14 hours, respectively. The delayed elevation of salicylate concentration made the medical team concerned for unabsorbed drug.
Why were the salicylate concentrations continuing to rise?
Bezoars:1,5
- Bezoars are concretions of foreign material that adhere together in the stomach.
- Pharmacobezoars are a subtype of bezoars in which the foreign material is composed of medications. Due to the reduced surface area of the bezoar compared to the individual pills, the absorption of drug is slow.
- Risk of bezoar formation increases with xenobiotics that delay gastric emptying, induce pylorospasm, or are enteric-coated. Furthermore, risk increases with any anatomical anomalies that obstruct the gastric outflow tract.
- Pearl: Enteric-coated medications may be radiolucent and thus require a high degree of clinical suspicion and direct visualization via endoscopy.
- Treatments include endoscopic removal or aspiration of gastric contents alternating with dissolution of bezoar via sodium bicarbonate (or other xenobiotic-specific solvents).
- Substances that form pharmacobezoars:

Table adapted from: Howland MA. Pharmacokinetic and Toxicokinetic Principles. In: Hoffman RS, Howland MA, Lewin NA, Nelson LS, Goldfrank LR, eds. Goldfrank’s Toxicologic Emergencies, 10e. New York, NY: McGraw-Hill Education; 2015.
Case 2:
A 72-year-old man with a history of prostate cancer with metastases to the spine. His home dose of morphine is 30 mg orally every 4 hours for chronic cancer pain. He is admitted to the hospital for pre-op observation, is made NPO, and is placed on an order for “morphine 30 mg IV every 4 hours” by the intern. He becomes obtunded and has bradypnea.
Why is the conversion or oral to IV dosing important?
First-Pass Effect:6,7
- Metabolism of a xenobiotic before it reaches the systemic circulation.
- Most metabolism is performed by the liver following gastrointestinal absorption.
- Can also occur by enterocytes, skin, lungs, and vascular endothelium.
- Various routes of administrations and formulations bypass the liver’s first pass effect thereby enhancing absorption.
Image from: Wilkinson GR. Drug metabolism and variability among patients in drug response. New England Journal of Medicine. 2005;352(21):2211-2221.
Case 3:8
A 43-year-old woman was found dead in her apartment. Empty bottles of loperamide and cimetidine were found at the scene.
What mechanism accounted for this toxicity?
P-Glycoprotein Efflux Transporters:8,9
- Active (energy requiring) efflux pumps that may decrease the bioavailability of drugs.
- Found in enterocytes (brush border), blood-brain barrier, blood-testis barrier, etc.
- P-glycoprotein efflux pumps share significant substrate specificity with the CYP3A4 enzymes.
- The P-glycoprotein efflux pumps can be saturated which results in rapid and extensive increases in the rate of absorption.
- As the concentration of substances greatly exceeds the capacity of transport mechanisms, absorption rate plateaus and exhibits zero-order absorption kinetics.
- Numerous substances can saturate these efflux pumps, including cimetidine, macrolide antibiotics, azole antifungals, piperine (a component of black pepper).
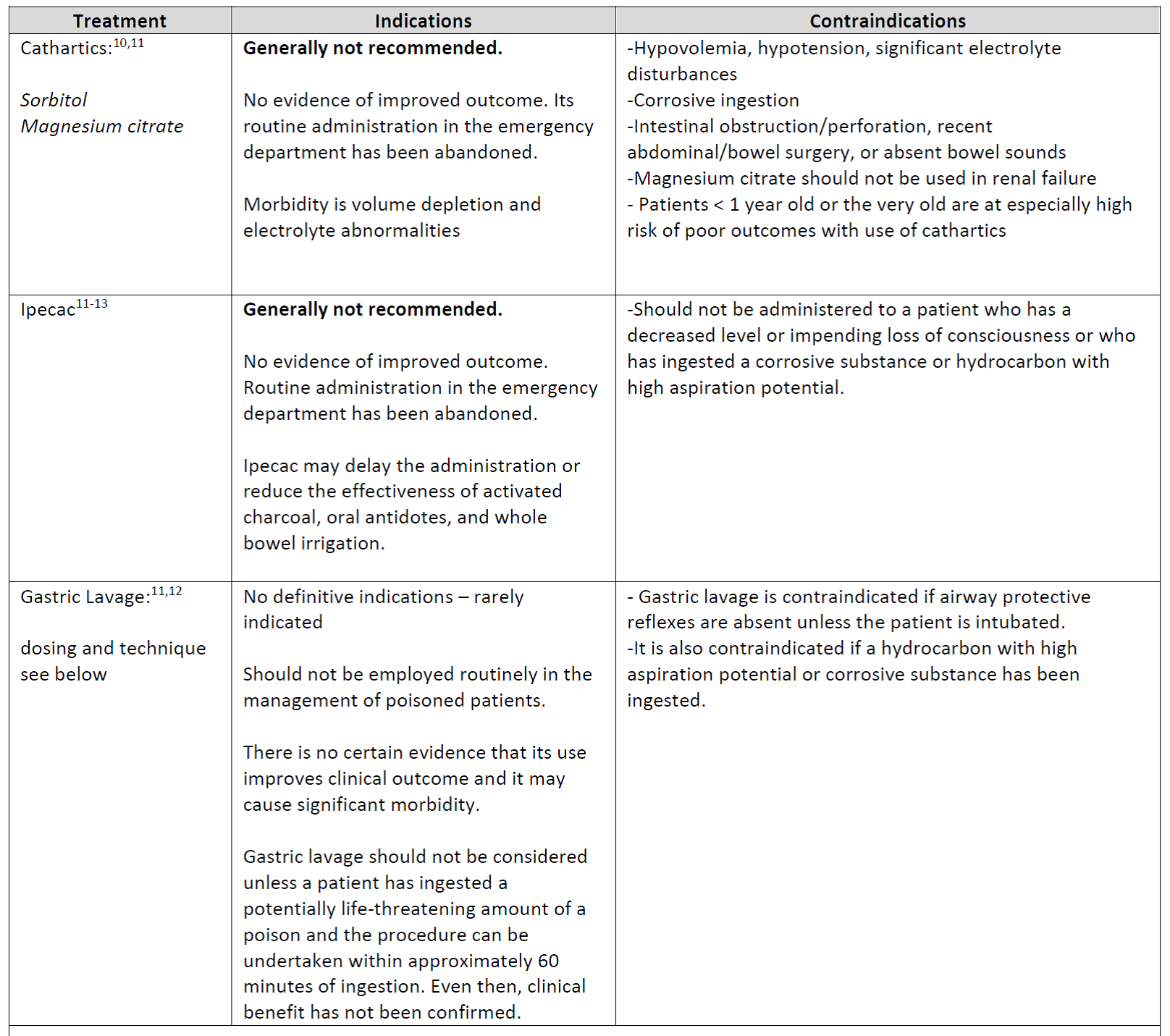
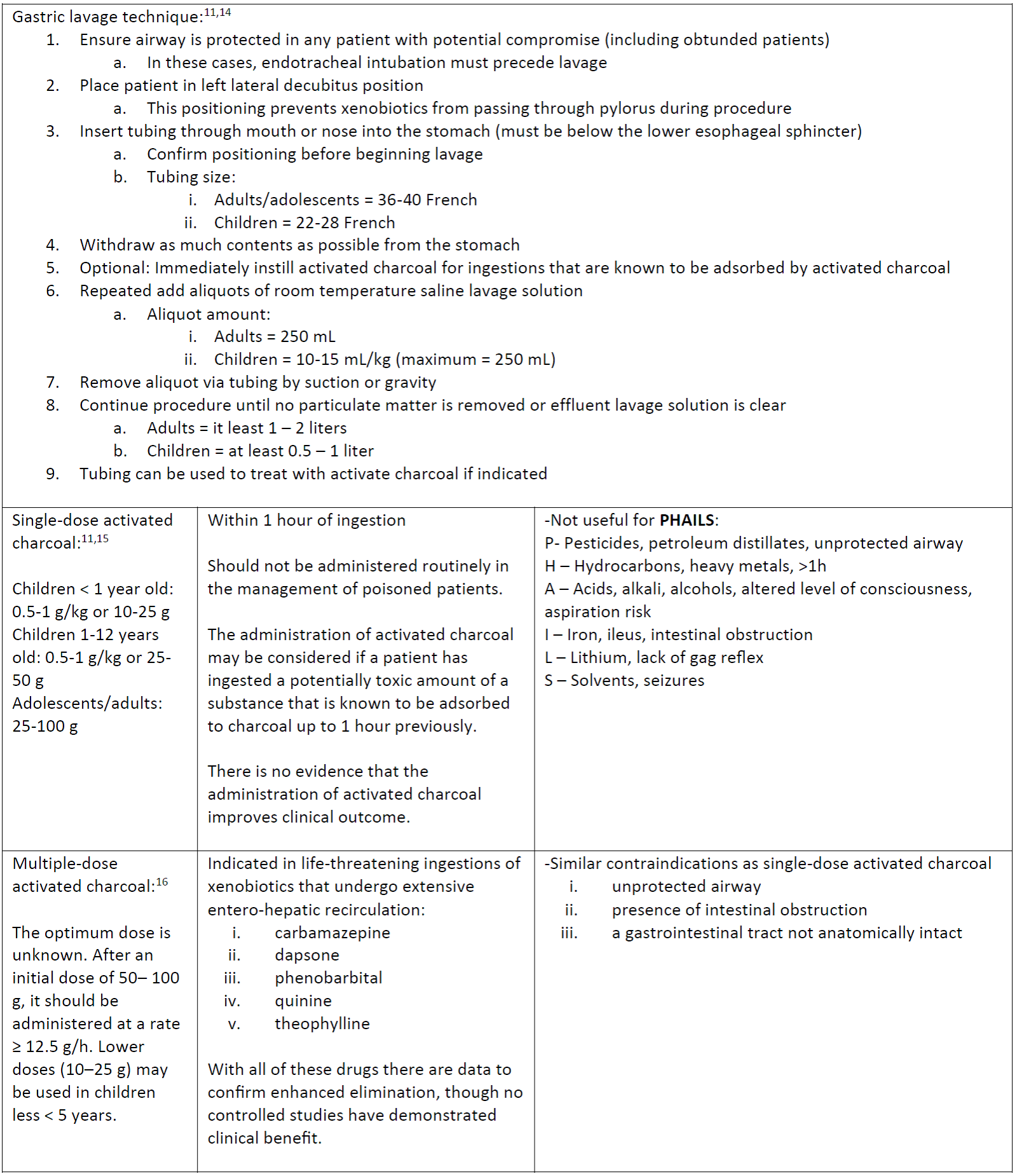
Gastric Decontamination:
- Therapeutic processes to decrease the absorption of an ingestion:
Main Points:
- Ion trapping is an important therapeutic modality to limit the absorption and enhance the elimination of compounds.
- Absorption can be greatly altered from traditional pharmacokinetics in toxicological settings.
- Bezoars can cause pronounced durations and delays in absorption following an ingestion.
- The first-pass effect and P-glycoprotein pumps also have a significant role in the absorption of toxicants, as well xenobiotic-xenobiotic interactions causing toxicity.
- Gastric decontamination is a management tool to minimize xenobiotic absorption.
- Single-dose activated charcoal is the main treatment option for gastric decontamination in patients that present within 1 hour of ingestion.
- Multiple-dose activated charcoal can decrease absorption and enhance elimination for xenobiotics that extensively undergo entero-hepatic recirculation.
References:
- Howland MA. Pharmacokinetic and Toxicokinetic Principles. In: Hoffman RS, Howland MA, Lewin NA, Nelson LS, Goldfrank LR, eds. Goldfrank’s Toxicologic Emergencies, 10e. New York, NY: McGraw-Hill Education; 2015.
- Buxton ILO. Pharmacokinetics: The Dynamics of Drug Absorption, Distribution, Metabolism, and Elimination. In: Brunton LL, Hilal-Dandan R, Knollmann BC, eds. Goodman & Gilman’s: The Pharmacological Basis of Therapeutics, 13e. New York, NY: McGraw-Hill Education; 2017.
- Shargel L, Yu ABC. Introduction to Biopharmaceutics and Pharmacokinetics. In: Shargel L, Yu ABC, eds. Applied Biopharmaceutics & Pharmacokinetics, 7e. New York, NY: McGraw-Hill Education; 2016.
- Cells and Tissues. In: Marieb EN, ed. Human Anatomy & Physiology. 5th ed: Benjamin-Cummings Pub Co; 2001.
- Parker V, Goldberg D, King MA. Case 1: Mysteriously Rising Salicylate Levels in a 15-year-old Girl. Pediatrics in review. 2017;38(6):280.
- Pond SM, Tozer TN. First-pass elimination basic concepts and clinical consequences. Clinical pharmacokinetics. 1984;9(1):1-25.
- Wilkinson GR. Drug metabolism and variability among patients in drug response. New England Journal of Medicine. 2005;352(21):2211-2221.
- Bhardwaj RK, Glaeser H, Becquemont L, Klotz U, Gupta SK, Fromm MF. Piperine, a major constituent of black pepper, inhibits human P-glycoprotein and CYP3A4. Journal of Pharmacology and Experimental Therapeutics. 2002;302(2):645-650.
- Lin JH, Yamazaki M. Role of P-Glycoprotein in Pharmacokinetics: Clinical implications. Clinical Pharmacokinetics. 2003;42(1):59–98.
- American Academy of Clinical Toxicology, European Association Poison Centres and Clinical Toxicologists. Position paper: cathartics. Journal of Toxicology: Clinical Toxicology. 2004;42(3):243-253.
- Hoegberg LCG, Gude A-B. Techniques Used to Prevent Gastrointestinal Absorption. In: Hoffman RS, Howland MA, Lewin NA, Nelson LS, Goldfrank LR, eds. Goldfrank’s Toxicologic Emergencies, 10e. New York, NY: McGraw-Hill Education; 2015.
- Benson B, Hoppu K, Troutman W, et al. Position paper update: gastric lavage for gastrointestinal decontamination. Clinical toxicology. 2013;51(3):140-146.
- Höjer J, Troutman W, Hoppu K, et al. Position paper update: ipecac syrup for gastrointestinal decontamination. Clinical toxicology. 2013;51(3):134-139.
- Olson KR, Anderson IB, Benowitz NL, et al. Comprehensive Evaluation and Treatment. Poisoning & Drug Overdose, 7e. New York, NY: McGraw-Hill Education; 2017.
- American Academy of Clinical Toxicology, European Association Poison Centres and Clinical Toxicologists. Position paper: single-dose activated charcoal. Clinical Toxicology. 2005;43(2):61-87.
- American Academy of Clinical Toxicology, European Association Poison Centres and Clinical Toxicologists. Position paper: multiple-dose activated charcoal. Clinical Toxicology. Clinical Toxicology. 1999; 37(6), 731–751.





4 thoughts on “TOXCards: Absorption Toxicokinetics”
Pingback: Intox – översikt – Mind palace of an ER doc
Would you please share the evidence base for this statement ” dissolution of bezoar via sodium bicarbonate (or other xenobiotic-specific solvents”. I am unaware that such a thing is studied and more concerned that dissolution will lead to increased absorption
Thanks for your comment. The use of sodium bicarbonate during endoscopy to dissolve bezoars have been reported in some case reports and in GI literature. I believe this should be done only if aspiration follows in order to avoid increased absorption. The quality of evidence isn’t great but it’s been reported, more commonly with phytobezoars.
https://www.science.gov/topicpages/g/gastric+bezoar+treated.html
OK, so what does a phytobezoar where absorption is of no consequence have to do with a drug?