
Author: Brit Long, MD (@long_brit, EM Attending Physician, San Antonio, TX) // Edited by: Alex Koyfman, MD (@EMHighAK, EM Attending Physician, UTSW / Parkland Memorial Hospital)
Welcome to EM@3AM, an emDOCs series designed to foster your working knowledge by providing an expedited review of clinical basics. We’ll keep it short, while you keep that EM brain sharp.
A 28-year-old female presents with right lower leg swelling and redness. She just returned from an overseas flight. She denies chest pain or shortness of breath. She has no medical problems but is on oral contraceptives. She has no family history of DVT or PE.
Triage vital signs (VS): BP 123/61, HR 72, T 98.2 Oral, RR 16, SpO2 99% on RA.
The patient appears well and non-toxic. Her right lower leg is swollen and red, with diameter > 3 cm compared to her left. She is neurovascularly intact in both legs.
What is the patient’s diagnosis? What’s the next step in your evaluation and treatment?
Answer: Deep Venous Thrombosis (DVT)
- Background: Venous thrombosis of the deep venous system, primarily in lower versus upper extremities.
- Pathophysiology: Clot formation in the deep veins due to fibrin production and deposition. Inciting mechanisms include venous stasis, venous injury, and hypercoagulability (Virchow’s Triad).
- Anatomy: Lower extremity contains superficial veins (greater and short saphenous veins) and deep veins (common femoral, deep femoral, superficial femoral, popliteal, peroneal, anterior/posterior tibial).
- Proximal DVT forms in the popliteal vein or higher.
- Distal DVT forms in the calf veins (anterior/posterior tibial and peroneal veins).
- DVTs are more common in the left versus right leg due to the left iliac artery crossing over the left iliac vein (compression).
- Upper extremity DVTs are less common but consist of thrombus in the axillary vein.
- History and Exam:
- Patients often present with nonspecific findings early including calf fullness or cramping.
- Symptoms later can include unilateral leg swelling (> 3 cm more than other side), edema, redness, pain for lower DVT. Upper extremity DVTs may present with arm and finger swelling.
- Exam may demonstrate unilateral leg swelling, erythema, warmth, tenderness to palpation, superficial vein dilation. Homan’s sign (painful dorsiflexion of the foot) is not sensitive or specific and should not be relied upon (sensitivity 60-96%, specificity 20-72%).
- Differential: Cellulitis, vascular disease, trauma, Baker’s cyst, compartment syndrome, fracture, gout, necrotizing fasciitis, phlegmasia cerulean dolens, phlegmasia alba dolens, and venous gangrene.
- Diagnostics:
- Begin with forming pretest probability – clinical gestalt versus Wells’. MDCalc makes it easy!
- Wells = 0: DVT unlikely (< 5%). Can perform D dimer testing. If negative, ruled out DVT.
- Wells = 1-2: DVT moderate risk; perform D dimer or US. If either negative, ruled out DVT.
- Wells > 3: DVT high risk; perform D dimer and US. If positive D dimer but negative US, require repeat US.
- Laboratory Testing
- Obtain CBC and renal function (assists with choosing anticoagulation therapy if DVT is diagnosed).
- D dimer: Elevation suggests clot presence. However, many conditions elevate D dimer (malignancy, infection, age, surgery, inflammation, immobilization, MI, new catheter, stroke).
- Quantitative D dimer (ELISA or immunoturbidimetric technique) is most commonly used. Cutoffs for a negative result depend on the assay and local instituation. Typically 500 ng/mL is utilized as the cutoff.
- If high sensitivity D dimer is negative, can be used to rule out DVT in low to medium risk patients. High risk patients require further testing if the test is negative.
- If moderate sensitivity D dimer is used, negative test result may require further testing if the patient is medium to high risk.
- Age adjusted D dimer: Normal D dimer level elevates with age. May use 10 X age (for those over age 50). This increases specificity, with minimal decrease in sensitivity. Reasonable in low to moderate risk patients.
- Qualitative D dimer: Lower sensitivity compared with other D dimer tests. Can only be used to rule out DVT in low risk patients.
- Venous Duplex Ultrasound
- Test of choice, noninvasive, performed rapidly.
- Can use 3-point test (common and superficial femoral veins, popliteal veins) or whole leg.
- Graded compression along path of vein. Full venous compression with pressure = no DVT present.
- Sensitivity and specificity approach 95%.
- Low pretest probability: Negative 3-point or whole leg US rules out DVT.
- Moderate to High probability: Negative whole leg US can rule out DVT. However, negative 3-point US cannot rule out DVT if negative. May add D dimer to 3-point US. If both negative, DVT is ruled out.
- ED POCUS: Data based on 2-point and 3-point testing. Should not be used to rule out DVT based on current literature (sensitivity 86-100%, specificity 89-99%).
- For some great content on DVT US, see this EMinSono page and this Ultrasound Podcast page for more.
- CT Venogram
- Can be used in conjunction with CT pulmonary angiography for PE. However, this should not be routinely added to CT PE, as interobserver agreement is poor.
- MRI
- Limited due to availability, cost, and lack of data. May assist in evaluation of vena cava and pelvic veins.
- Begin with forming pretest probability – clinical gestalt versus Wells’. MDCalc makes it easy!
- Isolated Distal DVT: Unknown significance. Most US examinations do not evaluate the distal system; however, the concern is that a distal DVT will extend and become a proximal DVT. Risk factors for extension include positive D dimer, > 5 cm in length, multiple veins, close to proximal veins, no reversible provoking factor for DVT, history of DVT/PE, hospital admission, active cancer.
- Management
- Proximal DVT, no history of cancer or active cancer: Oral anticoagulant (DOAC – direct oral anticoagulant) preferred over vitamin K antagonist (VKA) (Grade 2B). VKA is preferred over LMWH (Grade 2C). Duration of therapy is 3 months for 1st clot (Grade 1B).
- For more on direct oral anticoagulants, see this recent EMin5 post on emDocs.
- Proximal DVT with cancer: LMWH preferred over DOAC or VKA (Grade 2C). Duration 3 months for 1st clot (Grade 1B).
- Distal, isolated DVT: Proximal propagation may occur in up to 25% of distal clots.
- If no risk factors for extension and absence of severe symptoms, then serial imaging over 2 weeks is preferred (Grade 2C). No clear role for antiplatelet therapy, but this is reasonable.
- Presence of risk factors for extension or severe symptoms: Anticoagulation is preferred over serial imaging (Grade 2C). Same anticoagulation recommendations as for proximal DVT (Grade 1B).
- Superficial thrombophlebitis: Clots in the saphenous vein can spread to the deep venous system. Treat initially with NSAIDs, warm compresses, compression stockings. Repeat US in 3-5 days. If clot extends or is within 5 cm of the saphenous-femoral junction, may consider anticoagulation.
- Catheter-directed thrombolysis: Does not demonstrated benefits in most patients with proximal DVT, increased risk of bleeding. However, patients with iliofemoral DVT may benfit with decreased risk of post-thrombotic syndrome.
- For phegmasia cerulean dolens, consider thrombolytics/thrombectomy with vascular surgery consultation. Anticoagulation with heparin/VKA is needed.
- Recurrent DVT on anticoagulation: consider admission for vascular surgery and hematology consultation, IVC filter, heparin for anticoagulation.
- Complications: Biggest risk is embolus to the lungs (pulmonary embolism). Other complications include phlegmasia cerulean dolens, phlegmasia alba dolens, and venous gangrene. Of patients with PE, close to 40% will have concomitant DVT.
- Venous insufficiency may occur due to damage to venous valves. This ranges from varicose veins to postphlebetic syndrome (pain, swelling, ulcerations, increased infection risk).
- Disposition
- Most patients with DVT may be discharged home with DOAC or LMWH bridge to warfarin. Patients should be ambulatory, hemodynamically stable, low risk of bleeding, have no renal failure, and be able to follow up within several days.
- Consider admission for extensive clot (phlegmasia), ileofemoral DVT, high bleeding risk, significant comorbidities, unable to obtain follow up, renal disease (GFR < 30).
- Patients with negative US who are high risk require repeat US in 3-5 days.
This is the first week of a brand-new resource for EM@3AM to cement that learning, brought to you by Rosh Review.

A 52-year-old woman with recently diagnosed breast cancer presents to the emergency department with pain and swelling in her right leg. She denies any other medical history besides breast cancer and is not taking any other medicines at this time besides chemotherapy. Examination shows tenderness along the right calf and swelling to the right lower leg that appears more prominent than the left leg. She is noted to have pitting edema in the symptomatic leg. Venous duplex ultrasonography of the right leg reveals an occlusive thrombus in the popliteal vein. What is the appropriate management of this patient?
A. Begin treating with dabigatran orally and discharge to follow up with her primary medical doctor
B. Begin treating with intravenous heparin and admit to the medicine floor for further management
C. Begin treating with low molecular weight heparin subcutaneously and discharge to follow up with her primary medical doctor
D. Begin treating with warfarin orally and discharge to follow up with her primary medical doctor
Answer: C
Treatment for acute deep venous thrombosis (DVT) is divided into three stages: initial (0-7 days), long term (7 days-3 months) and extended (> 3 months). As it has become safe and common place for patients with a diagnosis of DVT to begin treatment in the emergency department and be discharged to follow up as an outpatient, it is imperative that the emergency physician understand the initial and long term treatment options. Parenteral anticoagulation has long been the mainstay of first-line DVT treatment to prevent extension or recurrence of clot. Most cases of proximal DVT will be treated with anticoagulant therapy in the initial and long term phases. There are now an array of anticoagulant options, including new direct oral anticoagulants, and choice of treatment must be tailored to the individual patient. In this cancer patient with a new diagnosis of DVT without other complicating factors the best treatment option would be to begin low molecular weight heparin therapy and discharge her to follow up with her primary doctor. This treatment allows outpatient management and choosing low molecular weight heparin for therapy is preferred in cancer patients for initial anticoagulation. Patients with active cancer carry a higher risk of recurrent venous thromboembolism and bleeding, and they have variable responses to traditional vitamin K antagonist therapy. Therefore, low molecular weight heparin is recommended.
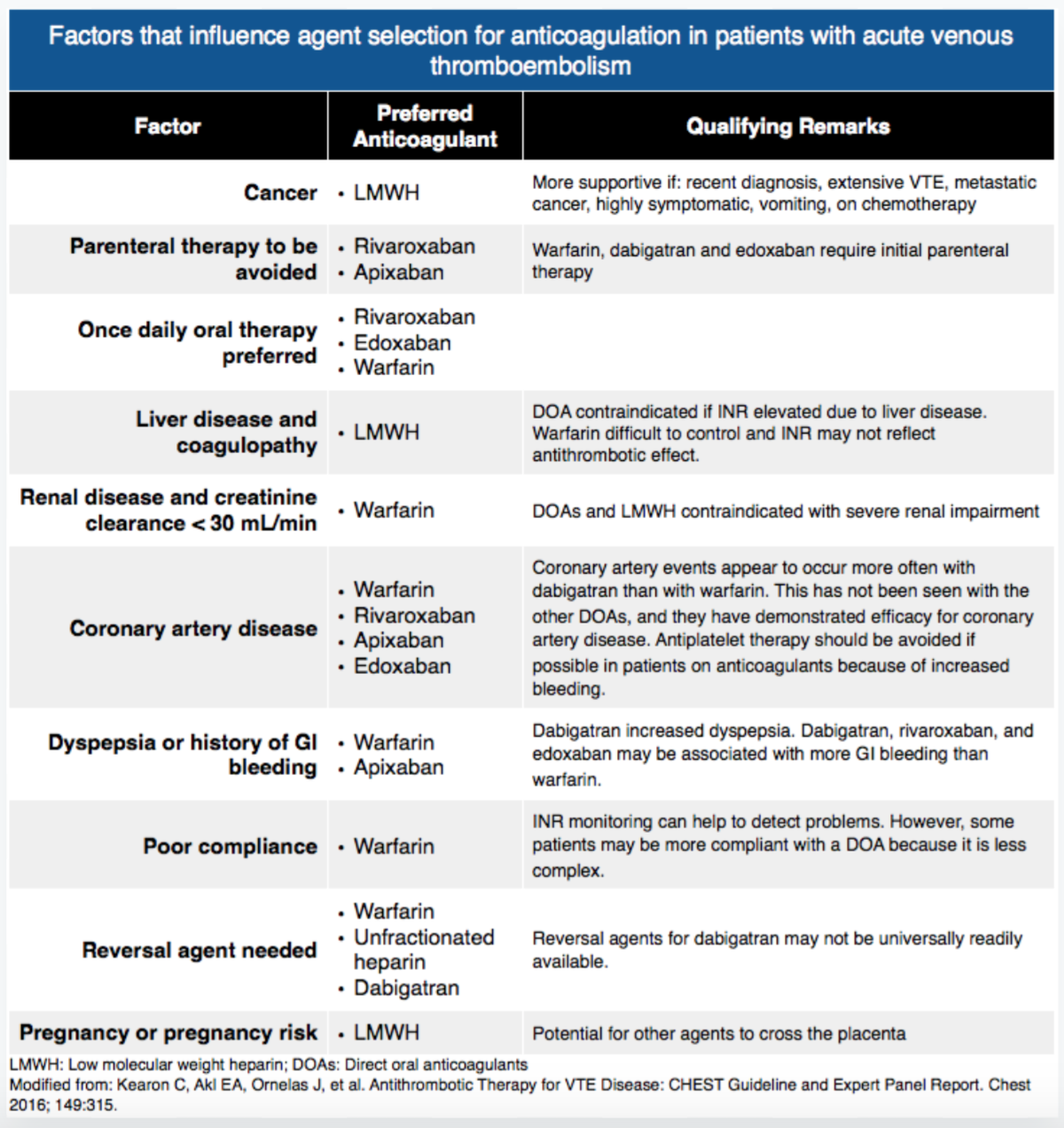
There are many other anticoagulation options available to the clinician including dabigatran, a thrombin inhibitor, and apixaban and rivaroxaban, both Xa inhibitors. Apixaban and rivaroxaban are good options for monotherapy. However, dabigatran does require bridging therapy with low molecular weight heparin. Therefore, beginning treatment with dabigatran and discharging to follow up with her primary medical doctor (A) would not be appropriate. The wide array of oral anticoagulants offers patients the flexibility for outpatient management of DVT and has become the mainstay of management for patients with a new DVT. Therefore, beginning treatment with intravenous heparin and admitting to the medicine floor for further management (B) would not be appropriate management of this patient. The clinician would not be faulted for beginning therapy with heparin and admitting this patient, but the most appropriate management would be outpatient therapy. To date, the most common and preferred outpatient regimen for patients with DVT who do not have cancer includes low molecular weight heparin as a bridge with vitamin K antagonist therapy such as warfarin. However, novel anticoagulation therapy is gaining speed. Beginning treatment with warfarin and discharging to follow up with her primary medical doctor (D) would not be appropriate since warfarin therapy requires bridging with low molecular weight heparin.
FOAMed:
https://coreem.net/core/deep-venous-thrombosis-dvt/
http://www.ultrasoundpodcast.com/?s=DVT
References:
- Wells PS et al. Does this patient have deep vein thrombosis? 2006; 295(2):199-207.
- Wells PS et al. Evaluation of D-dimer in the diagnosis of suspected deep-vein thrombosis. N Engl J Med. 2003; 349(13):1227-35.
- Adams D et al. Clinical utility of an age-adjusted D-dimer in the diagnosis of venous thromboembolism. Ann Emerg Med 2014.
- Baldridge ED et al. Clinical significance of free-floating venous thrombi. J Vasc Surg 1990; 11: 62-9.
- Pacouret G et al. Free-floating thrombus and embolic risk in patients with angiographically confirmed proximal deep venous thrombosis: a prospective study. Arch Intern Med 1997; 157: 305-8.
- Crisp JG et al. Compression ultrasonography of the lower extremity with portable vascular ultrasonography can accurately detect deep venous thrombosis in the emergency department. Ann Emerg Med 2010; 56 (6): 601-10.
- Kim DJ et al. Test characteristics of emergency physician-performed limited compression ultrasound for lower-extremity deep vein thrombosis. J Emerg Med 2016.
- Kearon C et al. Antithrombotic therapy for VTE disease: CHEST guideline and expert panel report. Chest 2016; 149(2): 315-52.
- Decousus H et al. Fondaparinux for the treatment of superficial-vein thrombosis in the legs. N Engl J Med 2010; 363:1222-1232.
- Bashir R et al. Comparative outcomes of catheter-directed thrombolysis plus anticoagulation vs anticoagulation alone to treat lower-extremity proximal deep vein thrombosis. JAMA Intern Med. 2014;174(9):1494-1501.





2 thoughts on “EM@3AM: DVT”
Pingback: CanadiEM Frontline Primer - Lower Leg Swelling - CanadiEM
Pingback: Episode 19: Early ED Discharge in Patients with low-risk VTE with DOACs - The Pharm So Hard Podcast