
Author: Shelly D. Saha, MD (EM Resident, UTSW / Parkland Memorial Hospital, Dallas, TX) // Edited by: Alex Koyfman, MD (@EMHighAK) and Brit Long, MD (@long_brit)
Welcome to EM@3AM, an emDOCs series designed to foster your working knowledge by providing an expedited review of clinical basics. We’ll keep it short, while you keep that EM brain sharp.
A 37-year-old G4P3003 female at 27 weeks GA presents via EMS for vaginal bleeding. She began having brisk vaginal bleeding after coitus about 30 minutes ago and has saturated 1 pad since onset. She denies associated abdominal pain, cramping, or prior episodes of vaginal bleeding during this pregnancy. She has not had regular prenatal care; however, she did have a transabdominal ultrasound in her first trimester showing an IUP. She has a history of 3 C-sections and denies complications during her other pregnancies.
On exam, her vitals are BP 102/65, HR 112, RR 20, SpO2 100% on RA, T 36.8°C. Her abdomen is gravid, soft, and non-tender. On external pelvic exam, she has no visible lesions, and the maternal pad she is sitting on is about 50% saturated with blood. You defer a bimanual or speculum exam at this time.
What’s the diagnosis? What’s the next step in your evaluation and treatment?
Answer: Placenta previa
Background:
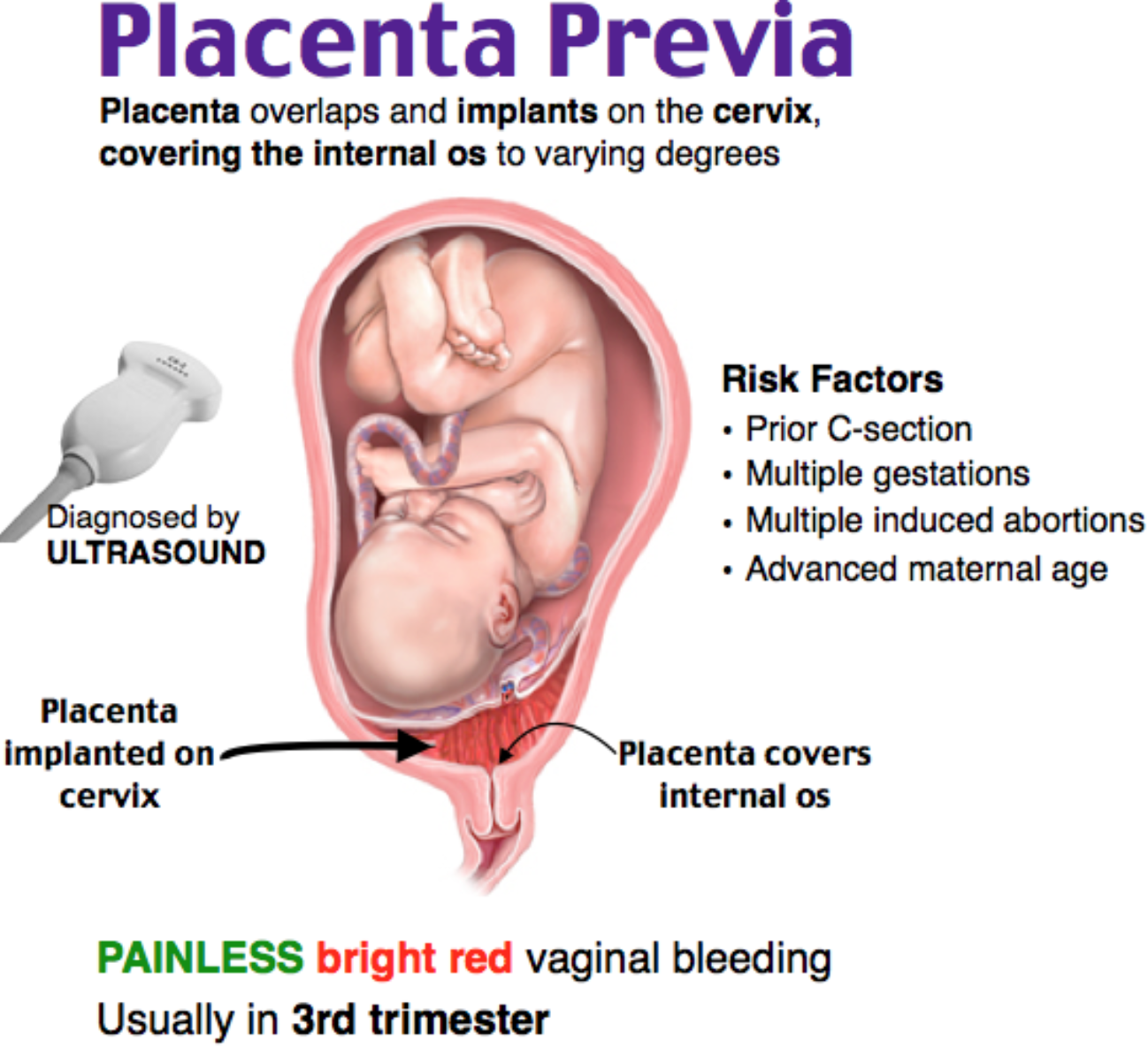
- Placenta overlying the os to any degree is classified as placenta previa.
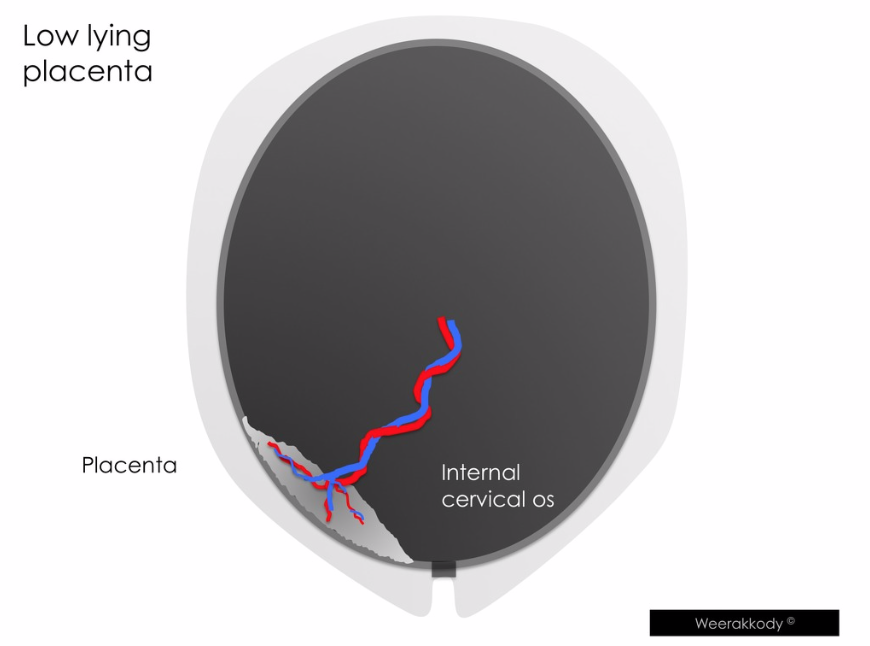
- Placental edge within 2 cm of but not overlying os is classified as low-lying placenta.
- Previous terminology of marginal, partial, complete is no longer used with TVUS providing more precise measurements.1
- Most placenta previas are diagnosed on routine prenatal transabdominal ultrasonography.
- However, early transabdominal ultrasound can be normal, so consider previa for all 2nd/3rd trimester vaginal bleeding.

Epidemiology
- Incidence: 1 in 200 pregnancies (increasing due to more C-sections being performed).1
- Many previas diagnosed in mid-pregnancy will resolve by time of birth due to placental “migration” away from cervix as pregnancy progresses.
- Risk factors: C-section, recurrent abortions, prior uterine surgery, multiparity, older maternal age, smoking, cocaine use, prior previa, multiple gestations.2-4
Clinical Implications
- Adverse outcomes for both mother and fetus.
- Poor maternal outcomes: increased need for blood transfusions, hysterectomy, ICU admission, sepsis, DIC, postpartum hemorrhage, mortality.5
- Poor fetal-neonatal outcomes: increased risk of prematurity, lower birth weight, lower Apgar score, mortality (increased 3- to 4-fold).1
- Placenta accreta (placental attachment to myometrium) occurs in approximately 10% of patients with placenta previa.6
- Vasa previa is more common in patients with placenta previa or low-lying placenta.
- Vasa previa – unprotected fetal vessels run over or near cervical os.
- High risk of fetal-neonatal hemorrhage with fetal vessel damage during labor.
- Stable placenta previa without bleeding or other complications is optimally delivered at 36 – 37 6/7 weeks of gestation.7
ED Presentation & Evaluation
- Painless vaginal bleeding after 18 weeks gestation is placenta previa until proven otherwise.
- Classic presentation is painless 2nd or 3rd trimester vaginal bleeding.
- However, uterine contractions occur in 15-20% of first bleeding episodes, so previa should always be on the differential for late term bleeding, even when abdominal pain/contractions are present.8 Must also consider placental abruption with pain and bleeding.
- Can have sentinel bleed which is rarely life-threatening; subsequent bleeding episodes tend to be more severe and occur more frequently.
- History
- Ask about prior placenta previa, uterine surgery, social risk factors, prenatal ultrasound abnormalities.
- Quantify amount of bleeding (number of pads saturated, passage of clots) and symptoms associated with bleeding (chest pain, shortness of breath, etc.).
- Physical exam
- Identify vital signs concerning for hemodynamic instability.
- Maternal tachypnea, tachycardia, hypotension, hypoxia are signs of hypovolemia.
- Use visual aids to monitor blood loss (regularly check maternity pad saturation).
- Never perform digital exam for late term bleeding until placental location is known (high chance of disrupting a clot if there is a previa).
- Obstetricians debate over whether a speculum exam is safe – can be performed to exclude other causes of vaginal bleeding (laceration, infection, etc), but it is important to avoid direct cervical manipulation.
- Identify vital signs concerning for hemodynamic instability.
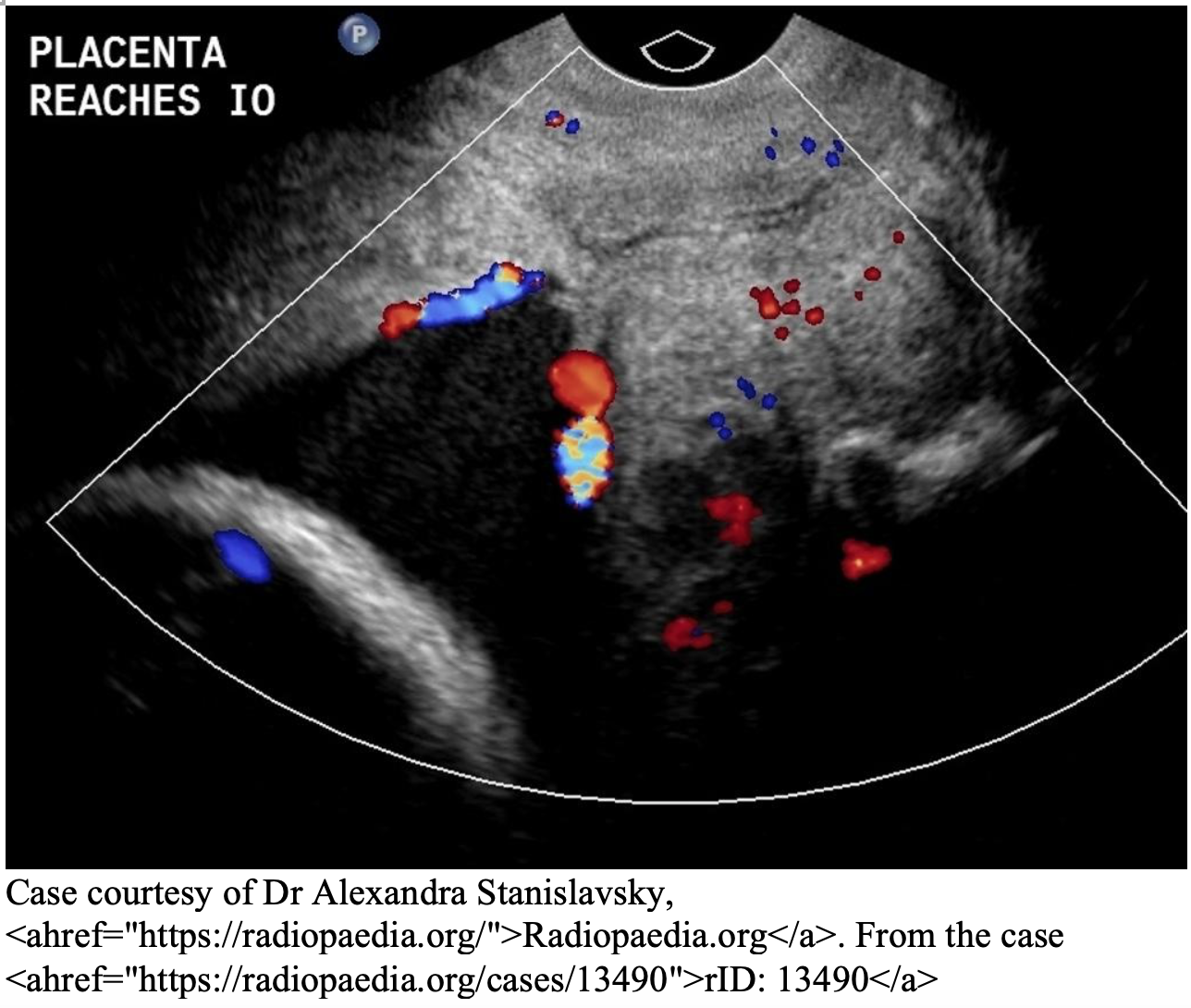
- Diagnosed by transvaginal ultrasound (95% sensitivity, 93% specificity).9
- Transabdominal ultrasound is less sensitive (86% sensitivity, 93% specificity).9
ED Management10
- Early involvement of obstetrics team – these patients will range from needing admission for observation to emergency C-section based on severity of bleed.
- Continuous maternal and fetal monitoring.
- Administer RhoGAM to Rh negative women.
- Resuscitate with fluids and blood transfusion to achieve and maintain maternal hemodynamic stability. In patients with massive bleed or actively bleeding placenta previa, prioritize giving blood products.
- Some sources argue for a transfusion goal of hemoglobin > 10 g/dL in anticipation of a rapid Hgb drop in the actively bleeding placenta.10
- Continue blood transfusion until patient is hemodynamically stable and bleeding has slowed.
- Most women presenting with actively bleeding placenta previa do not require emergency C-section and stabilize with the above measures.11
- Indications for C-section:
- Active labor.
- Nonreassuring fetal heart rate tracing or maternal hemodynamic instability unresponsive to resuscitation.
- Severe bleeding after 34 weeks – maternal risk of hemorrhage > fetal risk of preterm birth after 34 weeks.
Disposition
- >24 weeks: admission to L&D for observation vs emergency C-section if unstable after resuscitation.
- <24 weeks: can potentially be discharged home if small amount of bleeding which has resolved and patient has reliable follow-up.
- Many women have recurrent bleeding episodes requiring multiple hospitalizations.
From Dr. Katelyn Hanson and Hanson’s Anatomy:


A 23-year-old G1P0 woman at 30 weeks gestation presents to the emergency department for vaginal bleeding. She has had no prior prenatal care. She reports that she is soaking through one pad every eight hours. She denies abdominal cramping or a gush of water and reports good fetal movement. Her vital signs are T 37.2°C, HR 100, BP 105/70 mmHg, and RR 18. Her abdomen is soft, nontender, and consistent with a 30 week pregnancy. Which of the following is the most likely cause of this patient’s symptoms?
A) Abruptio placentae
B) Placenta previa
C) Threatened abortion
D) Velamentous cord insertion
Answer: B
Placenta previa is the presence of placental tissue overlying the internal cervical os and is a common cause of painless vaginal bleeding in women beyond 20 weeks gestation. Patients classically present with painless bleeding in the second or third trimester. Most cases of placenta previa are not seen on first-trimester ultrasound, and any woman without a second- or third-trimester ultrasound that presents with antepartum vaginal bleeding needs to have an abdominal ultrasound to assess the location of the placenta. Complications of placenta previa include hemorrhage, preterm labor and rupture of membranes, and fetal malpresentation. Type and screening for blood in patients with placenta previa serve two important purposes. First, mothers that are Rh negative should receive Rho (D) immune globulin after any bleeding episodes, including from delivery, previa, abruption, or threatened abortion, to prevent alloimmunization. Second, since hemorrhage is an important and potentially life-threatening complication of placenta previa, knowledge of maternal blood type is important for giving cross-matched blood.
Abruptio placentae (A) describes the separation of the placenta from the uterine wall prior to delivery. It is the second most common cause of vaginal bleeding after 20 weeks of gestation. In contrast to placenta previa, abruptio placenta is typically associated with abdominal pain. Threatened abortion (C) describes vaginal bleeding before 20 weeks gestation. The patient in the question above is in her third trimester and, therefore, cannot be diagnosed with threatened abortion. Velamentous cord insertion (D) is an uncommon cause of late-trimester bleeding caused by exposed fetal umbilical cord vessels. It is a far less common cause of late-trimester bleeding than placenta previa.
Further Reading:
FOAMed:
- emDOCs – The Bleeding Pregnant Patient in the Third Trimester: Pearls and Pitfalls http://www.emdocs.net/9117-2/
- EM in 5 – Third Trimester Bleeding https://emin5.com/2018/06/05/third-trimester-vaginal-bleeding/
- Taming the Sru – Placenta Previa http://www.tamingthesru.com/blog/annals-of-b-pod/b-pod-case/placenta-previa
- EMRAP – Placenta Previa https://www.emrap.org/episode/emrap20181/placentaprevia
References:
- Silver, R. M. (2015). Abnormal Placentation. Obstetrics & Gynecology, 126(3), 654-668. doi:10.1097/aog.0000000000001005
- Ananth CV, Wilcox AJ, Savitz DA, Bowes WA Jr, Luther ER. Effect of maternal age and parity on the risk of uteroplacental bleeding disorders in pregnancy. Obstet Gynecol 1996;88:511–6.
- Macones GA, Sehdev HM, Parry S, Morgan MA, Berlin JA. The association between maternal cocaine use and placenta previa. Am J Obstet Gynecol 1997;177:1097–100.
- Ananth CV, Demisse K, Smulian JC, Vintzileos AM. Placenta previa in singleton and twin births in the United States, 1989 through 1998: a comparison of risk factor profiles and associated conditions. Am J Obstet Gynecol 2003;188:275–81.
- Crane JM, Van den Hof MC, Dodds L, Armson BA, Liston R. Maternal complications with placenta previa. Am J Perinatol 2000;17:101–5.
- Miller, D., Chollet, J., and Goodwin, T. Clinical risk factors for placenta previa-accreta. American Journal of Obstetrics and Gynecology, 1997(1): 210-214.
- Gyamfi-Bannerman, C. (2018). Society for Maternal-Fetal Medicine (SMFM) Consult Series #44: Management of bleeding in the late preterm period. American Journal of Obstetrics and Gynecology, 218(1). doi:10.1016/j.ajog.2017.10.019
- Winn, H. N., MD, & Hobbins, J. C., MD. (2000). Clinical Maternal-Fetal Medicine (1st ed.). New York: The Parthenon Publishing Group.
- Petpichetchian, C., Pranpanus, S., Suntharasaj, T, et al. (2018). Comparison of transabdominal and transvaginal sonography in the diagnosis of placenta previa. J Clin Ultrasound, 46(6), 386-390. doi:10.1002/jcu.22600
- Lockwood, C. J., MD, MHCM, & Russo-Stieglitz, K., MD. (2019, January 30). Placenta Previa: Management. Retrieved from https://www.uptodate.com/contents/placenta-previa-management?search=placentaprevia&source=search_result&selectedTitle=1~102&usage_type=default&display_rank=1
- Cotton DB, Read JA, Paul RH, Quilligan EJ. The conservative aggressive management of placenta previa. Am J Obstet Gynecol 1980; 137:687.






1 thought on “EM@3AM: Placenta Previa”
Pingback: July FOAMed - FRCEM Success