
Authors: Brit Long, MD (@long_brit, EM Attending Physician, San Antonio, TX) and Michael Gottlieb MD, RDMS (EM Attending Physician, Rush Medical Center Department of Emergency Medicine) // Edited by: Alex Koyfman, MD (@EMHighAK, EM Attending Physician, UT Southwestern Medical Center / Parkland Memorial Hospital)
Welcome to another edition of emDocs Cases! This will be a case-based discussion of EM topics, ranging from core to cutting edge and controversial. This post evaluates something all too common in emergency medicine: the agitated patient.
A 26-year-old male presents with agitation and combativeness. EMS reports they were called for a combative male swinging a baseball bat in public. The patient was tazed by police, and they transported him to the ED. His VS include HR 125, BP 177/100, RR 22, T 100.8F, and saturation 98% on room air.
This edition will provide some background on the agitation in the ED, important conditions to consider, ED evaluation, and interventions to control agitation.
How common is agitation in the ED? What about altered mental status?
Before we start, we need to lay some groundwork. Agitated patients are often acutely altered, which accounts for 5-10% of all ED visits.1-5 Altered mental status with agitation has large number of etiologies: medical, traumatic, substance-induced, and psychiatric causes.4-9 Rapid diagnosis and control of agitation are required.
Unfortunately, this agitation can result in violence, and these patients are at risk to themselves and others around them. Over their careers, most emergency medicine personnel (whether technician, nurse, or physician) will be threatened, and close to 40% will experience violence.5,6,10-13
What could be the cause of this patient’s agitation?
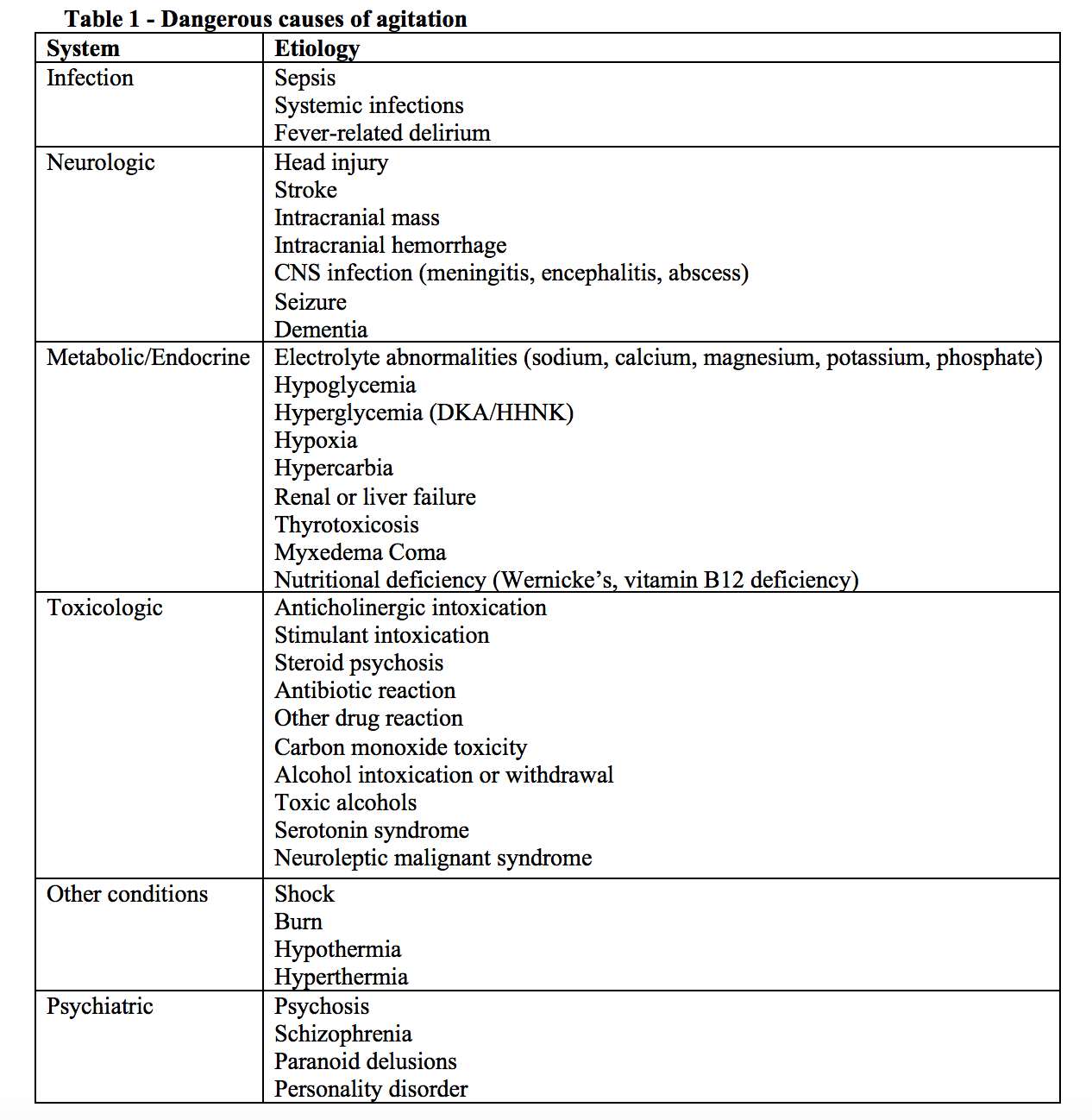
Acute agitation and altered mental status can be due to a wide variety of conditions, ranging from a dangerous medical condition to primary psychosis or intoxication.4-6 In the ED, alcohol or drug intoxication are the most common etiologies. 4-8,15-18 Others are shown in Table 1.
Are there specific types of altered mental status or agitation?
One major key is determining whether the patient is suffering from delirium or excited delirium. Delirium is a global disturbance in attention, cognition, and/or consciousness that occurs abruptly and fluctuates.8,17-20 Approximately 25% of elderly patients in the ED demonstrate delirium, which is a medical emergency (mortality rate approaches 33%).17-23 Change in consciousness ranges from coma to hyperactive agitation (the most common form is hypoactive delirium).6-8,17,18 One third of patients with dementia will demonstrate agitation, but most patients with delirium demonstrate shifting attention, difficulty following commands, and trouble with concentration.17-23
Excited delirium presents as an acute agitated state (fear, violence, shouting, hyperactivity, panic) and delirium, followed by respiratory compromise and potentially death.9,24-25 Patients are usually hyperthermic with increased strength. Close to 2/3’s of patients will die at the scene or during transport to the ED.9,24-25
Chronic cognitive impairment may also be associated with agitation. Patients with developmental disability, dementia, or severe brain injury can be confused and agitated in unfamiliar settings.8,17
What should the evaluation focus on?
Patient assessment and de-escalation should occur at the same time. Sedation may be needed as soon as possible with acute agitation.7,8 History can determine the cause in over 90% of patients,6-8,17 and history from the patient, EMS personnel, bystanders, family/friends, and caregivers is important. Patients may provide a different history than others when asked in the ED, and the goal should be determining the true underlying issue, as well as the time of onset, recent stressors, or exacerbating factors (infection, intoxication, trauma, medications, etc.). Other pertinent factors include baseline mental status, history of prior psychiatric disease/hospitalization, other violent episodes, and daily functional status. Substance use/intoxication, fevers, recent illness, trauma, history of immunocompromised state, cancer, or neurologic disease (mass, stroke, multiple sclerosis) suggest a medical etiology.6-8,14,16,17
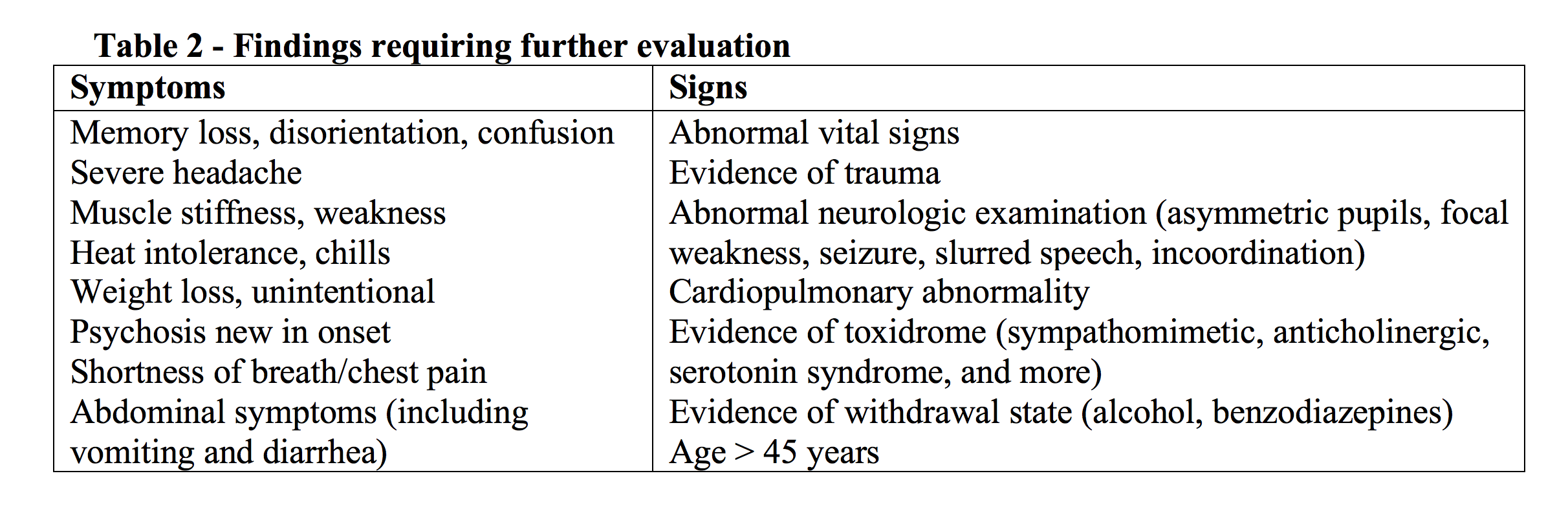
Exam should focus on vital signs and cardiopulmonary and neurologic systems. A blood glucose is needed as soon as it can be obtained. Table 2 contains signs and symptoms that should trigger a more in-depth evaluation, and physicians should focus on patient mental status including behavior, appearance, affective state, thought process, suicidal or homicidal ideations, attention, psychosis, awareness, judgment and insight, executive functions, and reliability. Components of the past history such as prior psychiatric conditions/hospitalization, family history, substance use, stressors, social support, and living condition are also important.6-8,14,16,17
What tests should you order? Do you need labs or imaging?
As is the rule with any altered patient, obtain that rapid point-of-care glucose level. Hypoglycemia can present in a variety of ways, with agitation a potential cause. Females should have a pregnancy test obtained. Other tests include ECG, CK, electrolytes, liver function, ethanol, and TSH should be considered, especially with new onset psychosis/agitation or red flags. A noncontrast head CT is recommended if findings of intracranial abnormality are present.6-8
Upon review of records, your patient has a record of repeated cocaine use and visits for intoxication/agitation. He is starting to wake and become agitated. Your techs were able to obtain bilateral IV’s and ECG, which shows sinus tachycardia. The serum glucose is 112.
What interventions are available to calm this patient?
The specific intervention and what you begin with depends on the degree of agitation. Patients who are agitated but willing to talk may just need some soft words and a sandwich, and if this does not work, oral medications are a great option. Patients who are agitated and disruptive but not dangerous need sedation, and an IV may be too dangerous during acute agitation, so IM may be best. Patients who are violent and uncontrollable may need immediate IM sedation as well.
Non-pharmacologic Interventions
If you can, start with verbal de-escalation.6,7,26-29 Most clinicians know the power of the turkey sandwich, and food and other measures (blankets) can go a long way. A quiet, safe location without other patients or loose supplies/objects is recommended. Larger rooms may allow the patient to feel less trapped. Decreased noise and dimmed lights may also produce a calmer environment. A patient’s ability to consider these options allows you to assess their ability to cooperate, and if medication is necessary in the ED, the patient may be more likely to take an oral medication.26-29 Richmond et al. provides several great techniques for de-escalation.29
Pharmacologic Interventions
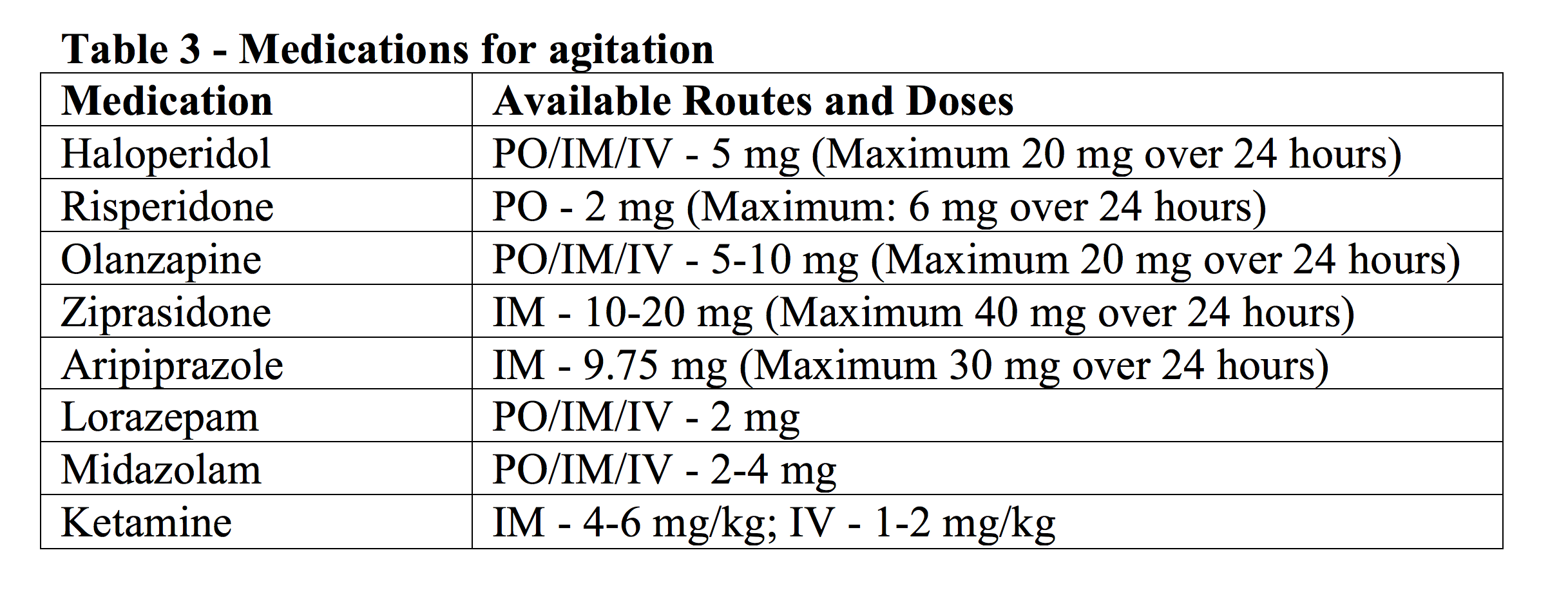
Unfortunately, verbal de-escalation doesn’t always work, and you may need to turn to medications. The objective is to calm, not completely sedate, the patient. 6,7,29-31 You have multiple options for route: PO, IM, or IV. If able, start with PO dosing, which decreases the risk of harm to you and the patient, while providing autonomy for the patient.6,31,32 Based on the literature, oral medications are just as effective as IV or IM.33-39 Dissolvable formulations ensure the medication reaches the patient.6,39
First-Generation Antipsychotic Agents
Haloperidol, a first-generation antipsychotic (FGA), is one of the classic medications for agitation, commonly in those with a known psychiatric history. Haloperidol is a typical, butyrophenone-type antipsychotic that possesses high affinity for D2 receptors.28 The mean time to sedation is 25-28 min, with mean total sedation time 84-126 min.40,41 Extrapyramidal symptoms (Parkinsonism, dystonia, akathisia) are the most common side effects, which can be decreased with use of an anticholinergic agent (diphenhydramine).28,42 A risk of QTc prolongation is present, which may be increased in patients taking other QTc prolonging agents.28
Second-Generation Antipsychotic Agents
Second-generation (atypical) antipsychotics (SGA) have recently been studied due to a better side effect profile.6,43-53 Patients can experience significant dysphoria after FGAs, and one study demonstrated a significant patient preference for SGAs vs. FGAs.54-56 Common SGAs include aripiprazole, olanzapine, ziprasidone, and quetiapine. These agents work at D2 receptors, like the FGAs, but they also affect 5-HT2A, histamine, norepinephrine, and a-2 receptors.28
SGAs have demonstrated similar overall efficacy vs. FGAs.43-46 Wright et al. found improved sedation with olanzapine vs. haloperidol during the first 45 minutes of treatment, but this resolved by one hour.43 FGAs and SGAs demonstrated low rates of adverse events.43,45,46 Though all antipsychotic medications can prolong the QTc, this occurs less commonly with SGAs and is rare in the ED (olanzapine, quetiapine, and risperidone).56
Though FGAs and SGAs are often given PO or IM, the IV route is a safe alternative when available.52,53 One study with olanzapine IV demonstrated a very low rate of akathisia, QTc prolongation, or allergic reactions among 672 ED patients.52 Another study identified no significant difference in respiratory depression, intubation, QTc prolongation, or other side effects among 784 patients receiving olanzapine IV or IM.53
Benzodiazepines
Benzodiazepines work at the GABA receptor and increase sedation. Several options are available, though lorazepam and midazolam are the most common agents. Lorazepam can be provided PO, IM, or IV. Midazolam can be provided via the intranasal, rectal, PO, IM or IV route. Lorazepam has a mean time to sedation 32 min and mean total sedation time 217 min, while midazolam has mean time to sedation 13-18 min and mean total sedation time 82-105 min.40,41 Some may prefer midazolam due to its more rapid action, while others may favor lorazepam’s longer total sedation time. Both can be effective. One study comparing ziprasidone vs. midazolam found midazolam had a more rapid time to sedation, but it required more doses of rescue medications.57
A combination of haloperidol with benzodiazepines may be superior to an agent alone. Several studies demonstrate improved sedation and no significant difference in adverse events.58-60 Other studies have evaluated midazolam with droperidol, which found improved behavior control with combination treatment.47-49
Ketamine
Ketamine is a dissociate agent that affects NMDA, nitric oxide synthase, and multiple opioid receptors.61,62 The medication works within 2-3 min and has a duration of effect up to 30 min.61,62 Recent literature has evaluated ketamine for use in the agitated patient. One study evaluated ketamine in agitated patients requiring aeromedical transport, finding a ketamine-based protocol resulted in lower rate of intubations.63 However, this is retrospective data, with no comparison agents described. Another study evaluated IM ketamine and IM haloperidol, finding ketamine to have faster time to adequate sedation (5 minutes vs. 17 minutes) but with higher rates of overall complications (49% vs. 5%) and intubations (39% vs. 4%).64 The one ED prospective, comparative study compared ketamine vs. haloperidol, benzodiazepines, or a combination of haloperidol and benzodiazepines.65 This study found ketamine resulted in a greater number of patients successfully sedated at 5, 10, and 15 min.65 Intubation was low in both groups.65 Keep in mind ketamine may wear off faster than other agents, needing another dose. Ketamine is not recommended in schizophrenia due to its potential to increase acute agitation, though it has not been associated with long-term consequences.66,67
When should you use physical restraints?
Restraints are still often used in the ED, with studies demonstrating their use in close to half of agitated patients.68-70 Physical restraints have been associated with injury related to agitation, and they do not protect patients from all injuries, as continued fighting can result in rhabdomyolysis.6,71 Asphyxiation, strangulation, and chest compression may also occur, and restraints are also associated with psychological adverse events.71-74
Verbal de-escalation and patient seclusion should be your first go-to. A show of force with multiple people may help, and if these fail, pharmacologic intervention is warranted before physical restraints if possible.6,7,69,70 If restraint is needed, five people are recommended (one for the head and one for each extremity). However, if physical restraint is required, soft cloth and locked leather restraints are most common.75 Though cloth restraints are often the most common form used, they can tighten and decrease circulation. Restraints should be secured to the bedframe, rather than the side rails, with one arm up and one down.75
During the restraint, verbal de-escalation should continue. The minimal restraints necessary to protect the patient and providers is recommended, along with close monitoring.6,75,76 The Centers for Medicare and Medicaid Services (CMS) states adult patients should remain in constant physical restraints no longer than 4 hours, 2 hours for adolescents, and 1 hour for children < 9 years.76 Restraints should be removed when able.
What about pediatric, pregnant, and elderly patients?
Pediatric Patients
Pediatric psychiatric and behavioral crises are increasing, accounting for close to 5% of pediatric ED visits.77 Agitation can begin with tantrums or defiance, which can progress to aggressive behavior and even physical violence. Verbal de-escalation is first-line, similar to adults. Family and caregivers can help with this, but if these members are the source of the agitation, then they need to be removed from the room.78
If medication is needed, PO should be attempted first. If the patient has a known psychiatric issue, an extra dose of home medication can be used. A new medication may result in a different reaction than adults. For example, benzodiazepines can result in paradoxical agitation, especially in young patients with developmental delay. Diphenhydramine is safe, as are antipsychotics (though FGA and SGA agents demonstrate greater extrapyramidal effects in pediatric patients).78,79 A FGA should be given with diphenhydramine. Olanzapine has been studied and has minimal side effects in pediatric patients.80
Pregnant Patients
Pregnant patients present another level of difficulty with agitation. Psychiatric conditions that were previously adequately managed may worsen during pregnancy, and the medications that are usable in pregnancy are limited.81,82 Risperidone is safe, with no known teratogenic effects, and can be used first line.82,83 Haloperidol is associated with fetal limb defects if used in a prolonged manner, but may be used for patients for acute events.82,84-86 Benzodiazepines are associated with cleft lip and remain controversial in prolonged use, but they may be safe in the acute setting.87 Valproic acid, carbamazepine, and lithium should be avoided due to teratogenicity in the first trimester.88-94 Restraints should be avoided if possible, but if they are required, IVC compression may occur in the 2nd/3rd trimester.82 Left lateral decubitus position or a support under the patient’s right side can be used to reduce this.82
Elderly Patients
Elderly patients are another challenging population due to increased comorbidities and different response to medications.6,30 This group more commonly requires an evaluation for inciting factors of agitation (Head CT, ECG, electrolytes, etc.).95,96 Similar to other populations, start with verbal de-escalation, with friends and family members utilized to assist with calming and reorienting the patient. If medications are used, use a lower dose (dose reduction by at least 1/2).95,96 Titration should also be slower than with younger patients.6,95,96 Benzodiazepines are associated with poor outcomes, even with one dose, and should be avoided.97,98 FGAs and SGAs can be used first-line, but close evaluation of the patient’s medication list is recommended, as the combination of an antipsychotic with other QTc prolonging agents can further increase the QTc interval.30
Case Conclusion
Your patient continues to swear, and you use a “show of force” with security and several technicians, in combination with attempting to verbally de-escalate. Instead of calming the patient, this worsens the patient’s agitation. You ask the nurse to administer ketamine 1.5 mg/kg IV, which calms the patient within one minute and averts a potentially disastrous situation.
For some great FOAMed resources, see:
https://emcrit.org/racc/human-bondage-chemical-takedown/
http://rebelem.com/chemical-sedation-of-the-agitated-patient/
http://emupdates.com/2016/09/03/emergency-management-of-the-agitated-patient/
http://emergencymedicineireland.com/2016/10/eusem16-ketamine-acute-behavioural-disturbance/
http://blog.ercast.org/art-chemical-takedown/
http://www.tamingthesru.com/blog/bread-and-butter/agitatedpatient
Key Points
– Acute agitation is common in the ED and requires rapid assessment and management.
– Acute agitation has a broad differential diagnosis which includes metabolic, neurologic, infectious, toxicologic, and psychiatric etiologies.
– Focused history and exam coupled with appropriate treatment strategies can effectively manage these patients.
– All patients should receive a point-of-care glucose test, with additional testing depending upon the specific patient presentation.
– Management should involve verbal de-escalation techniques, followed by pharmacologic interventions, with physical restraints reserved as a last resort.
– Medication options include FGAs, SGAs, benzodiazepines, and ketamine. The management of pediatric, pregnant, and elderly patients warrants special consideration.
References/Further Reading:
- Elie M, Rousseau F, Cole M, et al. Prevalence and detection of delirium in elderly emergency department patients. CMAJ. 2000 Oct 17;163(8):977-81.
- Hustey F, Meldon S. The prevalence and documentation of impaired mental status in elderly emergency department patients. Ann Emerg Med. 2002 Mar;39(3):248-53.
- Hustey F, Meldon S, Smith M, et al. The effect of mental status screening on the care of elderly emergency department patients. Ann Emerg Med. 2003 May;41(5):678-84.
- Kanich W, Brady W, Huff S, et al. Altered mental status: Evaluation and etiology in the ED. Am J Emerg Med. 2002 Nov;20(7):613-7.
- Nordstrom K, Zun LS, Wilson MP, et al. Medical Evaluation and Triage of the Agitated Patient: Consensus Statement of the American Association for Emergency Psychiatry Project BETA Medical Evaluation Workgroup. West J Emerg Med. 2012;13(1):3-10.
- New A, Tucci VT, Rios J. A Modern-Day Fight Club? The Stabilization and Management of Acutely Agitated Patients in the Emergency Department. Psychiatr Clin North Am. 2017 Sep;40(3):397-410.
- Han JH, Wilber ST. Altered mental status in older patients in the emergency department. Clin Geriatr Med. 2013;29(1):101–36.
- Wilber ST, Ondrejka JE. Altered mental status and delirium. Emerg Med Clin North Am. 2016;34(3):649–65.
- Takeuchi A, Ahern TL, Henderson SO. Excited Delirium. West J Emerg Med. 2011;12(1):77-83.
- Al-Sahlawi KS, Zahid MA, Shahid AA, et al. Violence against doctors: 1. A study of violence against doctors in accident and emergency departments. Eur J Emerg Med. 1999; 6:301.
- Schwartz TL, Park TL. Assaults by patients on psychiatric residents: a survey and training recommendations. Psychiatr Serv. 1999; 50:381.
- Lavoie FW, Carter GL, Danzl DF, et al. Emergency department violence in United States teaching hospitals. Ann Emerg Med. 1988;17(11):1227–1233.
- Kansagra SM, Rao SR, Sullivan AF, et al. A survey of workplace violence across 65 U.S. emergency departments. Academic Emergency Medicine. 2008;15(12):1268–1274.
- American College of Emergency Physicians Clinical Policies Subcommittee (Writing Committee) on the Adult Psychiatric Patient. Clinical Policy: Critical Issues in the Diagnosis and Management of the Adult Psychiatric Patient in the Emergency Department. Ann Emerg Med. 2017;69(4):480-498.
- Olshaker JS, Browne B, Jerrard DA, Prendergast H, Stair TO. Medical clearance and screening of psychiatric patients in the emergency department. Acad Emerg Med. 1997 Feb;4(2):124-8.
- Stowell KR, Florence P, Harman HJ, et al. Psychiatric Evaluation of the Agitated Patient: Consensus Statement of the American Association for Emergency Psychiatry Project BETA Psychiatric Evaluation Workgroup. West J Emerg Med. 2012;13(1):11-16.
- Caplan LR. Delirium: a neurologists view—the neurology of agitation and overactivity. Rev Neurol Dis. 2010;7(4):111-8.
- Ely EW, Margolin R, Francis J, et al. Evaluation of delirium in critically ill patients: validation of the Confusion Assessment Method for the Intensive Care Unit (CAMICU). Crit Care Med. 2001;29(7):1370–9.
- Inouye SK, Van Dyck CH, Alessi CA, et al. Clarifying confusion: the confusion assessment method: a new method for detection of delirium. Ann Intern Med. 1990;113(12):941–8.
- Grover S. Assessment scales for delirium: a review. World J Psychiatry. 2012;2(4):58.
- Naughton BJ, Moran MB, Kadah H, et al. Delirium and other cognitive impairment in older adults in the emergency department. Ann Emerg Med. 1995 Jun;25(6):751-5.
- Inouye S, Rushing J, Foreman M, et al. Does delirium contribute to poor hospital outcomes? A three-site epidemiologic study. J Gen Intern Med. 1998; 13: 234-242.
- Pompei P, Foreman M, Rudberg M, et al. Delirium in hospitalized older persons: outcome and predictors. J Gen Intern Med. 1998 Apr;13(4):234-42.
- Sztajnkrycer MD, Baezz AA. Cocaine, excited delirium and sudden unexpected death. Emerg Med Serv. 2005;34(4):77-81.
- Ruttenber AJ, Lawler-Heavner J, Yin M, et al. Fatal excited delirium following cocaine use: epidemiologic findings provide new evidence for mechanisms of cocaine toxicity. J Forensic Sci. 1997;42(1):25-31.
- Gaynes BN, Brown CL1, Lux LJ, et al. Preventing and De-escalating Aggressive Behavior Among Adult Psychiatric Patients: A Systematic Review of the Evidence. Psychiatr Serv. 2017 Aug 1;68(8):819-831.
- Knox DK, Holloman GH Jr. Use and avoidance of seclusion and restraint: consensus statement of the American Association for emergency psychiatry project Beta seclusion and restraint workgroup. West J Emerg Med. 2012 Feb;13(1):35-40.
- Wilson MP, Pepper D, Currier GW, Holloman GH Jr, Feifel D. The psychopharmacology of agitation: consensus statement of the American Association for emergency psychiatry project Beta psychopharmacology workgroup. West J Emerg Med. 2012 Feb;13(1):26-34.
- Richmond JS, Berlin JS, Fishkind AB, et al. Verbal De-escalation of the Agitated Patient: Consensus Statement of the American Association for Emergency Psychiatry Project BETA De-escalation Workgroup. West J Emerg Med. 2012 Feb;13(1):17-25.
- Somes J, Donatelli NS. Medicating the “Out of Control” Older Adult. J Emerg Nurs. 2016 Jan;42(1):75-7.
- Zun L, Wilson MP, Nordstrom K. Treatment Goal for Agitation: Sedation or Calming. Ann Emerg Med. 2017 Nov;70(5):751-752.
- Gault TI, Gray SM, Vilke GM, Wilson MP. Are oral medications effective in the management of acute agitation? J Emerg Med. 2012 Nov;43(5):854-9.
- Currier GW, Simpson GM. Risperidone liquid concentrate and oral lorazepam versus intramuscular haloperidol and intramuscular lorazepam for treatment of psychotic agitation. J Clin Psychiatry. 2001 Mar;62(3):153-7.
- Lejeune J, Larmo I, Chrzanowski W, et al. Oral risperidone plus oral lorazepam versus standard care with intramuscular conventional neuroleptics in the initial phase of treating individuals with acute psychosis. Int Clin Psychopharmacol. 2004 Sep;19(5):259-69.
- Currier GW, Chou JC, Feifel D, et al. Acute treatment of psychotic agitation: a randomized comparison of oral treatment with risperidone and lorazepam versus intramuscular treatment with haloperidol and lorazepam. J Clin Psychiatry. 2004 Mar;65(3):386-94.
- Kinon BJ, Ahl J, Rotelli MD, McMullen E. Efficacy of accelerated dose titration of olanzapine with adjunctive lorazepam to treat acute agitation in schizophrenia. Am J Emerg Med. 2004 May;22(3):181-6.
- Hsu WY, Huang SS, Lee BS, Chiu NY. Comparison of intramuscular olanzapine, orally disintegrating olanzapine tablets, oral risperidone solution, and intramuscular haloperidol in the management of acute agitation in an acute care psychiatric ward in Taiwan. J Clin Psychopharmacol. 2010 Jun;30(3):230-4.
- Lim HK, Kim JJ, Pae CU, et al. Comparison of risperidone orodispersible tablet and intramuscular haloperidol in the treatment of acute psychotic agitation: a randomized open, prospective study. Neuropsychobiology. 2010;62(2):81-6.
- Pascual JC, Pérez V, Martín JL, Safont G, Puigdemont D, Alvarez E. Olanzapine orally-disintegrating tablet in severe psychotic agitation: a naturalistic study. Actas Esp Psiquiatr. 2007 Jan-Feb;35(1):47-51.
- Nobay F, Simon BC, Levitt MA, Dresden GM. A prospective, double-blind, randomized trial of midazolam versus haloperidol versus lorazepam in the chemical restraint of violent and severely agitated patients. Acad Emerg Med. 2004 Jul;11(7):744-9.
- Isenberg DL, Jacobs D. Prehospital Agitation and Sedation Trial (PhAST): A Randomized Control Trial of Intramuscular Haloperidol versus Intramuscular Midazolam for the Sedation of the Agitated or Violent Patient in the Prehospital Environment. Prehosp Disaster Med. 2015 Oct;30(5):491-5.
- Wirshing WC. Movement disorders associated with neuroleptic treatment. J Clin Psychiatry. 2001;62 Suppl 21:15-8.
- Wright P, Birkett M, David SR, et al. Double-blind, placebo-controlled comparison of intramuscular olanzapine and intramuscular haloperidol in the treatment of acute agitation in schizophrenia. Am J Psychiatry. 2001 Jul;158(7):1149-51.
- Meehan K, Zhang F, David S, et al. A double-blind, randomized comparison of the efficacy and safety of intramuscular injections of olanzapine, lorazepam, or placebo in treating acutely agitated patients diagnosed with bipolar mania. J Clin Psychopharmacol. 2001 Aug;21(4):389-97.
- Breier A, Meehan K, Birkett M, et al. A double-blind, placebo-controlled dose-response comparison of intramuscular olanzapine and haloperidol in the treatment of acute agitation in schizophrenia. Arch Gen Psychiatry. 2002 May;59(5):441-8.
- Battaglia J, Lindborg SR, Alaka K, Meehan K, Wright P. Calming versus sedative effects of intramuscular olanzapine in agitated patients. Am J Emerg Med. 2003 May;21(3):192-8.
- Chan EW, Taylor DM, Knott JC, Phillips GA, Castle DJ, Kong DC. Intravenous droperidol or olanzapine as an adjunct to midazolam for the acutely agitated patient: a multicenter, randomized, double-blind, placebo-controlled clinical trial. Ann Emerg Med. 2013 Jan;61(1):72-81.
- Taylor DM, Yap CYL, Knott JC, et al. Midazolam-Droperidol, Droperidol, or Olanzapine for Acute Agitation: A Randomized Clinical Trial. Ann Emerg Med. 2017 Mar;69(3):318-326.
- Yap CYL, Taylor DM, Knott JC, et al. Intravenous midazolam-droperidol combination, droperidol or olanzapine monotherapy for methamphetamine-related acute agitation: subgroup analysis of a randomized controlled trial. 2017 Jul;112(7):1262-1269.
- Centorrino F, Meyers AL, Ahl J, et al. An observational study of the effectiveness and safety of intramuscular olanzapine in the treatment of acute agitation in patients with bipolar mania or schizophrenia/schizoaffective disorder. Hum Psychopharmacol. 2007 Oct;22(7):455-62.
- MacDonald K, Wilson M, Minassian A, et al. A naturalistic study of intramuscular haloperidol versus intramuscular olanzapine for the management of acute agitation. J Clin Psychopharmacol. 2012 Jun;32(3):317-22.
- Martel ML, Klein LR, Rivard RL, Cole JB. A Large Retrospective Cohort of Patients Receiving Intravenous Olanzapine in the Emergency Department. Acad Emerg Med. 2016 Jan;23(1):29-35.
- Cole JB, Moore JC, Dolan BJ, et al. A Prospective Observational Study of Patients Receiving Intravenous and Intramuscular Olanzapine in the Emergency Department. Ann Emerg Med. 2017 Mar;69(3):327-336.
- Lambert M, Schimmelmann BG, Karow A, Naber D. Subjective well-being and initial dysphoric reaction under antipsychotic drugs – concepts, measurement and clinical relevance. 2003 Nov;36 Suppl 3:S181-90.
- Karow A, Schnedler D, Naber D. What would the patient choose? Subjective comparison of atypical and typical neuroleptics. 2006 Mar;39(2):47-51.
- Glassman AH, Bigger JT Jr. Antipsychotic drugs: prolonged QTc interval, torsade de pointes, and sudden death. Am J Psychiatry. 2001 Nov;158(11):1774-82.
- Martel M, Sterzinger A, Miner J, Clinton J, Biros M. Management of acute undifferentiated agitation in the emergency department: a randomized double-blind trial of droperidol, ziprasidone, and midazolam. Acad Emerg Med. 2005 Dec;12(12):1167-72.
- Battaglia J, Moss S, Rush J, et al. Haloperidol, lorazepam, or both for psychotic agitation? A multicenter, prospective, double-blind, emergency department study. Am J Emerg Med. 1997 Jul;15(4):335-40.
- Bieniek SA, Ownby RL, Penalver A, Dominguez RA. A double-blind study of lorazepam versus the combination of haloperidol and lorazepam in managing agitation. 1998 Jan-Feb;18(1):57-62.
- Hui D, Frisbee-Hume S, Wilson A, et al. Effect of Lorazepam With Haloperidol vs Haloperidol Alone on Agitated Delirium in Patients With Advanced Cancer Receiving Palliative Care: A Randomized Clinical Trial. 2017 Sep 19;318(11):1047-1056.
- Weant KA, Linder LM, Ross CA. Ketamine for the acute management of excited delirium and agitation in the prehospital setting. 2017 Nov 14. doi: 10.1002/phar.2060. [Epub ahead of print]
- Clements JA, Nimmo WS. Pharmacokinetics and analgesic effect of ketamine in man. Br J Anaesth. 1981 Jan;53(1):27-30.
- Le Cong M, Humble I. A Ketamine Protocol and Intubation Rates for Psychiatric Air Medical Retrieval. Air Med J. 2015 Nov-Dec;34(6):357-9.
- Cole JB, Moore JC, Nystrom PC, et al. A prospective study of ketamine versus haloperidol for severe prehospital agitation. Clin Toxicol (Phila). 2016 Aug;54(7):556-62.
- Riddell J, Tran A, Bengiamin R, Hendey GW, Armenian P. Ketamine as a first-line treatment for severely agitated emergency department patients. Am J Emerg Med. 2017 Jul;35(7):1000-1004.
- Lahti AC, Koffel B, LaPorte D, Tamminga CA. Subanesthetic doses of ketamine stimulate psychosis in schizophrenia. 1995 Aug;13(1):9-19.
- Lahti AC, Warfel D, Michaelidis T, Weiler MA, Frey K, Tamminga CA. Long-term outcome of patients who receive ketamine during research. Biol Psychiatry. 2001 May 15;49(10):869-75.
- Cleary KK, Prescott K. The Use of Physical Restraints in Acute and Long-term Care: An Updated Review of the Evidence, Regulations, Ethics, and Legality. J Acute Care Phys Ther. 2015 Apr;6(1):8-15.
- Zun LS, Downey L. The use of seclusion in emergency medicine. Gen Hosp Psychiatry. 2005 Sep-Oct;27(5):365-71.
- Downey LV, Zun LS, Gonzales SJ. Frequency of alternative to restraints and seclusion and uses of agitation reduction techniques in the emergency department. Gen Hosp Psychiatry. 2007 Nov-Dec;29(6):470-4.
- Mohr WK, Petti TA, Mohr BD. Adverse effects associated with physical restraint. Can J Psychiatry. 2003 Jun;48(5):330-7.
- Rubin BS, Dube AH, Mitchell EK. Asphyxial deaths due to physical restraint. A case series. Arch Fam Med. 1993 Apr;2(4):405-8.
- Evans D, Wood J, Lambert L. Patient injury and physical restraint devices: a systematic review. J Adv Nurs. 2003 Feb;41(3):274-82.
- Berzlanovich AM, Schöpfer J, Keil W. Deaths due to physical restraint. Dtsch Arztebl Int. 2012 Jan;109(3):27-32.
- Glezer A, Brendel RW. Beyond emergencies: the use of physical restraints in medical and psychiatric settings. Harv Rev Psychiatry. 2010 Nov-Dec;18(6):353-8.
- Centers for Medicare and Medicaid Services. State Operations Manual. Department of Health and Human Services; 2008. Available at: https://www.cms.gov/Regulations-and-Guidance/Guidance/Transmittals/downloads/R37SOMA.pdf. Last accessed: December 3rd, 2017.
- Grupp-Phelan J, Harman JS, Kelleher KJ. Trends in mental health and chronic condition visits by children presenting for care at U.S. emergency departments. Public Health Rep. 2007 Jan-Feb;122(1):55-61.
- Santillanes G, Gerson RS. Special Considerations in the Pediatric Psychiatric Population. Psychiatr Clin North Am. 2017 Sep;40(3):463-473.
- Ratcliff SL, Meyer WJ 3rd, Cuervo LJ, et al. The use of haloperidol and associated complications in the agitated, acutely ill pediatric burn patient. J Burn Care Rehabil. 2004 Nov-Dec;25(6):472-8.
- Cole JB, Klein LR, Strobel AM, et al. The Use, Safety, and Efficacy of Olanzapine in a Level I Pediatric Trauma Center Emergency Department Over a 10-Year Period. Pediatr Emerg Care. 2017 Jul 11. doi: 10.1097/PEC.0000000000001231. [Epub ahead of print]
- Yonkers KA, Vigod S, Ross LE. Diagnosis, pathophysiology, and management of mood disorders in pregnant and postpartum women. Obstet Gynecol. 2011 Apr;117(4):961-77.
- Aftab A, Shah AA. Behavioral Emergencies: Special Considerations in the Pregnant Patient. Psychiatr Clin North Am. 2017 Sep;40(3):435-448.
- Ratnayake T, Libretto SE. No complications with risperidone treatment before and throughout pregnancy and during the nursing period. J Clin Psychiatry. 2002 Jan;63(1):76-7.
- McCullar FW, Heggeness L. Limb malformations following maternal use of haloperidol. 1975 Jan;231(1):62-4.
- Iqbal MM, Aneja A, Rahman A, et al. The potential risks of commonly prescribed antipsychotics: during pregnancy and lactation. Psychiatry (Edgmont). 2005 Aug;2(8):36-44.
- Diav-Citrin O, Shechtman S, Ornoy S, et al. Safety of haloperidol and penfluridol in pregnancy: a multicenter, prospective, controlled study. J Clin Psychiatry. 2005 Mar;66(3):317-22.
- Dolovich LR, Addis A, Vaillancourt JM, Power JD, Koren G, Einarson TR. Benzodiazepine use in pregnancy and major malformations or oral cleft: meta-analysis of cohort and case-control studies. BMJ. 1998 Sep 26;317(7162):839-43.
- Wyszynski DF, Nambisan M, Surve T, et al; Antiepileptic Drug Pregnancy Registry. Increased rate of major malformations in offspring exposed to valproate during pregnancy. 2005 Mar 22;64(6):961-5.
- Jentink J, Loane MA, Dolk H, et al; EUROCAT Antiepileptic Study Working Group. Valproic acid monotherapy in pregnancy and major congenital malformations. N Engl J Med. 2010 Jun 10;362(23):2185-93.
- Hernández-Díaz S, Smith CR, Shen A, et al; North American AED Pregnancy Registry; North American AED Pregnancy Registry. Comparative safety of antiepileptic drugs during pregnancy. 2012 May 22;78(21):1692-9.
- Cohen LS, Friedman JM, Jefferson JW, Johnson EM, Weiner ML. A reevaluation of risk of in utero exposure to lithium. 1994 Jan 12;271(2):146-50.
- Cohen LS. Treatment of bipolar disorder during pregnancy. J Clin Psychiatry. 2007;68 Suppl 9:4-9.
- ACOG Committee on Practice Bulletins-Obstetrics. ACOG Practice Bulletin: Clinical management guidelines for obstetrician-gynecologists number 92, April 2008 (replaces practice bulletin number 87, November 2007). Use of psychiatric medications during pregnancy and lactation. Obstet Gynecol. 2008 Apr;111(4):1001-20.
- Källén AJ. Maternal carbamazepine and infant spina bifida. Reprod Toxicol. 1994 May-Jun;8(3):203-5.
- Peisah C, Chan DK, McKay R, Kurrle SE, Reutens SG. Practical guidelines for the acute emergency sedation of the severely agitated older patient. Intern Med J. 2011 Sep;41(9):651-7.
- Aftab A, Shah AA. Behavioral Emergencies: Special Considerations in the Geriatric Psychiatric Patient. Psychiatr Clin North Am. 2017 Sep;40(3):449-462.
- Kruse WH. Problems and pitfalls in the use of benzodiazepines in the elderly. Drug Saf. 1990 Sep-Oct;5(5):328-44.
- Bogunovic OJ, Greenfield SF. Practical geriatrics: Use of benzodiazepines among elderly patients. Psychiatr Serv. 2004 Mar;55(3):233-5.





5 thoughts on “emDocs Cases: ED Approach to Agitation”
Pingback: Agitation aux Urgences: une revue pour le clinicien – ABCMed
Pingback: emDOCs.net – Emergency Medicine EducationJournalFeed Weekly Wrap-Up - emDOCs.net - Emergency Medicine Education
Pingback: Ep 115 Emergency Management of the Agitated Patient - Emergency Medicine Cases
Pingback: The Agitated Patient in the ED: Moderate & Severe Agitation - CanadiEM
Pingback: Agitation w/ Reuben Strayer – The Paramedic Practitioner