Authors: Brit Long, MD (@long_brit, EM Attending Physician at SAUSHEC) and Drew A. Long, BS (@drewlong2232, Vanderbilt University School of Medicine) // Edited by: Alex Koyfman, MD (@EMHighAK, EM Attending Physician, UT Southwestern Medical Center / Parkland Memorial Hospital)
Welcome to emDocs Cases! This will be a case-based discussion of EM topics, ranging from core to cutting edge and controversial. Today, we start with something common in emergency medicine: community-acquired pneumonia (CAP).
———————————————————————————-
You start your first shift with two patients. One is a 24-year-old male with three days of fever, productive cough, and chills. He has noted decreased appetite, but no nausea, vomiting, or diarrhea. He has no past medical history, takes no medications, and has no allergies.
Exam reveals RR 23/min, HR 112 bpm, Sat 95% on RA, T 38.1C, and BP 128/68. He appears tired though nontoxic, with normal mucosa, HEENT, and abdominal exams. You detect R sided rhonchi on lung exam, but no other abnormalities.
Your second patient is a 73-year-old female with a history of CAD and DM. She presents with three days of fever, productive cough, and chills. She lives at home with her husband, who has severe dementia. She is the primary caregiver for him. She has not been able to adequately care for him due to her illness. She takes aspirin, metoprolol, hydrochlorothiazide, and metformin.
Exam reveals RR 24/min, HR 92, Sat 90% on RA, T 37.9, and BP 132/75. She has dry mucosa, with rhonchi on the left. She has normal CV and abdominal exams as well, with no skin breakdown.
So these are our two patients. Today we will discuss several aspects of community acquired pneumonia including: 1) disease perspective, 2) history and physical exam, 3) chest radiograph, 4) alternate imaging, 5) ultrasound use, and 6) clinical scores/disposition.
1. Disease perspective: what is community acquired pneumonia?
Pneumonia is an acute infection of the pulmonary alveoli. Pneumonia is a common infection and the leading cause of infectious deaths. The mortality rate in severe pneumonia is 28%, but it is more commonly under 5%. The Infectious Diseases Society of America (IDSA) recently redefined pneumonia subtypes, shown here:
|
Community-acquired pneumonia
|
Acute pulmonary infection in a patient who is not hospitalized or residing in a long-term care facility 14 or more days before presentation. |
| Hospital-acquired pneumonia | Pneumonia occurring 48 hours or more after a hospital admission not present on initial presentation. |
| Ventilator-associated pneumonia | Pneumonia occurring 48-72 hours after intubation that wasn’t present prior to that intubation. |
Community acquired pneumonia is common, as it is responsible for 60,000 hospitalizations per year. Causes of pneumonia include bacteria (most common), viruses, and fungi. However, a microbial agent is never identified in over 50% of patients with pneumonia. Typical agents include S. pneumoniae and H. influenza, with S. pneumo being the most common. “Atypical” pathogens include Legionella, Mycoplasma, and Chlamydia. Viral causes include influenza, parainfluenza, coronavirus, and many others.
2. For our patients, what historical and physical examination findings point toward pneumonia?
The common signs and symptoms of pneumonia include cough (79%-91%), fever (up to 80%), increased sputum (up to 65%), pleuritic chest pain (up to 50%), respiratory rate above 24 breaths/minute (45% to 70%), chills (40% to 50%), and dyspnea (approximately 70%).14-20 However, no combination is diagnostic. Lung findings like percussion and crackles are most reliable. But, as most of us know, examination varies and is not consistent between providers.11,14-18,20
| Finding | Positive Likelihood Ratio | Negative Likelihood Ratio |
| History:
Fever Chills |
1.7-2.1 1.3-1.7 |
0.6-0.7 0.7-0.9 |
| Examination:
Tachypnea Hyperthermia Dullness to percussion Decreased breath sounds Crackles Rhonchi Egophony |
1.6-2.3 1.5-3.4 1.4-4.4 2.2-4.3 2.3-2.5 1.6-2.7 1.4-1.5 2.0-8.6 |
0.5-0.7 0.8 0.6-0.8 0.8-0.9 0.6-0.8 0.6-0.9 0.8-0.9 0.8-1.0 |
| Laboratory:
Elevated WBC |
1.9-3.7 |
0.3-0.6 |
The 24-year-old male clinically appears to have pneumonia. However, the older female does not have a fever. Could this still be pneumonia?
Atypical equals typical in the elderly. Patients who present with nonspecific complaints, such as altered mental status or nausea/vomiting, include elderly, immunocompromised, and debilitated patients. Other nonspecific symptoms include lightheadedness, malaise, weakness, headache, joint pain, and rash. Older patients often have fewer symptoms, with delirium being more common. Up to 2/3 of elderly patients will not have cough, fever, or shortness of breath, and they are less likely to present with chills. 21-24 Over half will present with confusion. Respiratory rate is important to assess, as tachypnea is a reliable factor in pneumonia diagnosis. 21-24
3. What testing is warranted? Does everyone need a CXR to diagnose pneumonia?
Clinically, the 23-year-old male has pneumonia. You have started 1 L NS, with 1 g ceftriaxone for community acquired pneumonia with 500 mg azithromycin PO. Though he meets sepsis criteria based on SIRS, he appears nontoxic and well. Does he need a CXR? Will it change your management?
The diagnosis of CAP is typically based on the combination of history, exam, and CXR.5,6,11,13 In the ED, many patients with respiratory complaints receive a CXR, and if suggestive of pneumonia, antibiotics are often given.15-19 The prevalence of pneumonia in patients with URI symptoms approaches 5%-7% when vital signs are otherwise normal.
How good is CXR for diagnosing pneumonia?
CXR is often considered a standard for diagnosis of pneumonia, but this test lacks specificity and sensitivity. 15,16,20 The 2007 IDSA guidelines recommend some form of imaging, with clinical symptoms, to diagnose pneumonia (Level III evidence, moderate recommendation).6 However, CXR is negative in over 30% of patients with pneumonia, with a sensitivity ranging from 46%-77%.19,25-28 One study found CXR missed one third of pneumonias, and CT excluded pneumonia in 30% of cases where pneumonia was diagnosed based on CXR.20,25-28 CXR cannot be relied on for diagnosis, and many other conditions may demonstrate radiograph findings that mimic pneumonia. Immunosuppression, dehydration, and elderly patients more commonly do not demonstrate radiographic findings due to lack of neutrophil migration. 27-30 These patients may present later with radiographic findings on repeat imaging. Other patients with influenza, pertussis, asthma, and COPD present similarly to pneumonia with negative radiograph.11 Strep pneumoniae classically presents as lobar infiltrate, Staph aureus as abscess or extensive infiltration, and Klebsiella as lobar pneumoina with bulging minor fissure. These are just several examples of “classic” findings, but these should not be relied on.
Other findings on CXR include pleural effusions, basilar infiltrates, interstitial infiltrates, or abscesses. Pneumonia can present with varying patterns on CXR, and many patients may not demonstrate the classic radiologic findings, particularly elderly and immunocompromised patients.11,15
When is chest radiograph not warranted?
We know that history and physical exam are not always reliable. Some form of imaging, usually CXR, is often used to evaluate for pneumonia.16,23 Patients with abnormal vital signs or signs of sepsis (including tachycardia, respiratory rate > 20 breaths/minute, or fever), age greater than 64 years, and exam findings (focal consolidation, egophony, rales, rhonchi, or wheezes unilaterally) warrant radiograph.16,23,36,39-41 Patients younger than 64 years with the absence of abnormal vital signs or physical examination findings may not need CXR, as probability of pneumonia is less than 5%.16,36,41-44 Despite this, many institutional and provider preferences vary.
You obtain a CXR for both patients, as the younger male meets SIRS criteria with positive findings on exam, and the older patient has an abnormal exam. The CXR in the male is positive for right lower lobe pneumonia, and labs show WBC 12, BUN 22 mg/dL, and normal electrolytes otherwise. His lactate is 1.2. The female has nonspecific findings with negative CXR. Her lactate is 2.8, WBC is 15.2, influenza rapid screen is negative, and BUN 32 mg/dL. You are still suspicious of pneumonia based on her history and exam. What else can help you?
4. How about ultrasound?
US is quick and reliable for the diagnosis of pneumonia. US demonstrates a sensitivity of 95%, compared to 60% for CXR.33-35 US findings suggestive of pneumonia include air bronchograms, b-lines, consolidations, pleural line abnormalities, and pleural effusions. Pathognomonic findings include dynamic air bronchograms.33-35 Positive likelihood ratios (LR) for these findings are 15.6 to 16.8, with negative likelihood ratios of 0.03 to 0.07.33-35
Please see this video for more: https://www.youtube.com/watch?v=21yJm6IDuRA
You ultrasound the female patient, and on the left side you detect the following imaging:
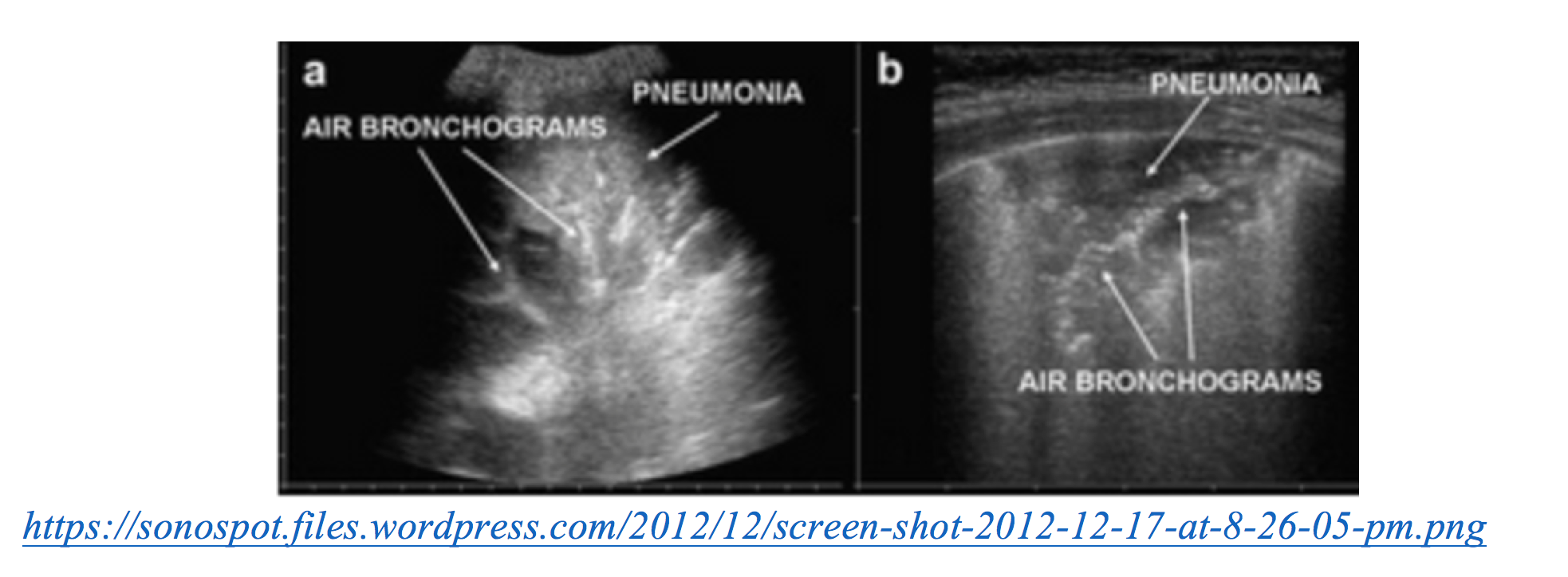
You start antibiotics and fluids, as your suspicion on pneumonia has increased. What can you use to further characterize these findings?
5. How about CT?
Chest CT has a sensitivity that approaches 100%.19,30 In patients with suspected pneumonia, 27% have identifiable infiltrate on CT and nothing on CXR.30 Another study suggests CT reveals pulmonary infiltrates in 33% of patients with no finding on CXR, while excluding CAP in close to 30% of patients with infiltrates on CXR.19,28,30 CT is more precise and accurate for pneumonia.19,28,30 Like every test in the ED, the risks and benefits must be weighed, as CT has significant cost and increased radiation compared to CXR, and it can potentially increase the ED length of stay. It should not be used as the standard diagnostic tool. However, in septic patients with no identifiable source and negative chest radiograph but upper respiratory symptoms suggestive of pneumonia, it should be considered.
CT chest noncontrast demonstrates infiltrate on the left. You continue your management.
6. Ok, I’ve diagnosed pneumonia, and it seems to be community acquired. Who can go home? Are there scales or systems that can assist in making this decision?
There are a number of aspects that impact mortality from pneumonia. These are shown below.5,6,15,16,20,25
| Finding | Odds Ratio (95% CI) |
| History:
Acute confusion Shortness of breath History of heart failure History of cancer History of neurologic disease History of renal disease |
2.0 (1.7-2.3) 2.9 (1.9-3.8) 2.4 (2.2-2.5) 2.7 (2.5-2.9) 4.4 (3.8-4.9) 2.7 (2.5-2.9) |
| Examination:
Tachypnea Hypothermia (temperature < 37oC) SBP < 100 mm Hg |
2.5 (2.2-2.8) 2.6 (2.1-3.2) 5.4 (5.0-5.9) |
| Ancillary studies:
BUN > 20 mg/dL WBC < 4 x 109 cells/L WBC > 10 x 109 cells/L Multilobar involvement |
2.7 (2.3-2.0) 5.1 (3.8-6.4) 4.1 (3.5-4.8) 3.1 (1.9-5.1) |
Scores or scales can assist in patient disposition by stratifying illness severity, including CURB-65 and PSI/PORT.5-7,25,31,32,45-48 CURB-65 was derived and validated in 2003. Based on this score, patients with 0 or 1 point can be discharged with antibiotic therapy. Patients with 2 points can be admitted or observed, while those with greater than 3 points should be admitted. Patients with score 4 or 5 should be admitted to the ICU.7,25,47,48 The CRB-65 scale may help when labs are difficult or not feasible, and CURB does not incorporate age.51,52 The table below shows the score, available on MDcalc: https://www.mdcalc.com/curb-65-score-pneumonia-severity
| Predictor | Score |
| Confusion
BUN > 19 mg/dL (> 7 mmol/L) Respiratory Rate > 30 Systolic BP < 90 mm Hg or Diastolic < 60 mm Hg Age > 65 years |
1
1 1 1 1 |
| Score:
0 1 2 3 4 or 5 |
30-day Mortality:
0.60-0.70% 2.10-2.70% 6.80-9.20% 14.00-14.50% 27-57% |
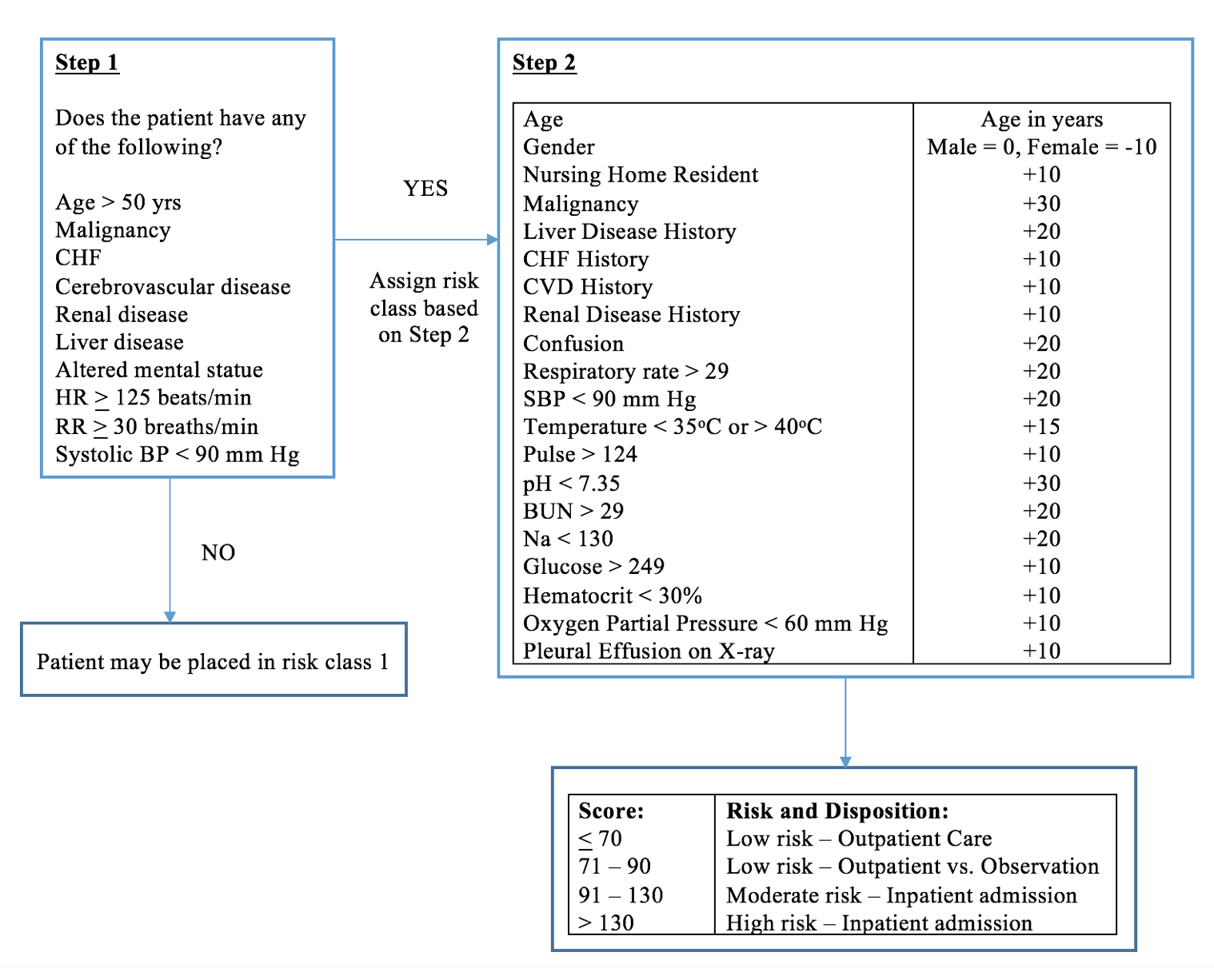
The PSI/PORT score consists of a five-tier risk stratification system.7,25,31,32 It has been validated several times: one study of 38,000 admitted patients, and another study of 2,287 patients in an inpatient and outpatient setting.31,32,49-51 The score is based on age, comorbidities, physical exam, and labs, with completion requiring several steps.25,31,32,49,50,51 The first step entails evaluating patient age. Patients over 50 years are assigned to classes II – V.25,31,32,49-51 A diagram of the PSI/PORT score is shown below. This score can increase the number of patients treated as outpatient, with reduction in mortality and admission rates (by 15%).25,49-56 See MDCalc: https://www.mdcalc.com/psi-port-score-pneumonia-severity-index-cap. The SOAR score is another option, but we will not discuss this score here.25,46,57
How do the scores compare?
Several studies have looked at score characteristics. PSI/PORT may have better sensitivity, with CURB-65 demonstrating greater specificity and PPV. Remember, PSI/PORT requires calculation with history, exam, labs, and CXR, while CURB-65 does not have hypoxemia or CXR findings. ROC curves are 0.81 for PSI, 0.73 for CURB, and 0.76 for CURB-65 in one study,50,51 with 0.736 for PSI and 0.694 for CURB-65 in another.58
| Characteristic | PSI
(95% CI) |
CURB-65
(95% CI) |
CURB
(95% CI) |
CRB-65
(95% CI) |
| Pooled Sensitivity | 0.90 (0.87-0.92) | 0.62 (0.54-070) | 0.63 (0.49-0.76) | 0.33 (0.24-0.44) |
| Pooled Specificity | 0.53 (0.46-0.59) | 0.79 (0.75-0.83) | 0.77 (0.68-0.83) | 0.92 (0.86-0.96) |
| Positive Predictive Value | 0.14 (0.13-0.16) | 0.24 (0.19-0.30) | 0.17 (0.14-0.22) | 0.28 (0.18-0.41) |
| Negative Predictive Value | 0.98 (0.98-0.99) | 0.95 (0.93-0.97) | 0.97 (0.96-0.97) | 0.94 (0.92-0.95) |
| Diagnostic Odds Ratio | 10.77 (8.29-13.97) | 6.40 (5.05-8.10) | 5.75 (4.59-7.21) | 5.97 (3.41-10.44) |
PSI/PORT can identify more patients as low risk. Keep in mind the scores may be better when used together to predict mortality, though this has not been evaluated. These scores do not assess social status. Homelessness, poor follow up, substance abuse, and PO intolerance are not accounted for in these scores, and they can underestimate severity in younger patients. Clinical gestalt is necessary in association with scores. 50,51,58-61
The 24-year-old has a CURB-65 of 0 and PSI/PORT of 24 points (Class 1). The female has a CURB-65 of 2 and PSI/PORT 93 points (Class IV).
Bonus: What about biomarkers other than lactate?
A lot of research has focused on biomarkers. These include WBC, Procalcitonin (PCT), and CRP. Elevated WBC cannot be relied upon, with over ¼ of patients with confirmed pneumonia demonstrating normal WBC. 21,62-64 The +LR of 1.9-3.7 and poor specificity are also unreliable.16,20,25,51,60
PCT is released in response to bacterial infections, 65-68 with a meta-analysis finding a pooled sensitivity and specificity of 77% and 79%, respectively.66 Sensitivity for bacterial infection in another meta-analysis is 88%, with a specificity of 81%.67 Most studies to date have evaluated the use of PCT to determine when to discontinue antibiotics. However, studies including a Cochrane meta-analysis suggest PCT does not affect mortality, relapse rate, or length of stay.69-71
CRP comes from the liver in response to inflammation and possesses a sensitivity of 70% and specificity of 90% if a threshold of 40 mg/L is used for pneumonia diagnosis, though specificity is 65% in another study.72,73
WBC, PCT, and CRP should not be used for routine evaluation of pneumonia, and further study is needed.
The 24-year-old male is looking better, now with normal VS. He wants to leave, and you discharge him with antibiotics. The female also feels improved following your resuscitation, but with her risk stratification score and your clinical gestalt, you discuss her case with the hospitalist, who agrees with you that she should be admitted.
Summary
– Pneumonia possesses a wide range of presentations.
– One study shows a prevalence of 2.6% for pneumonia in patients with URI symptoms, while other studies suggest this is closer to 7%.
– No combination of history, exam, and testing can improve the diagnostic probability of pneumonia to over 50%.
– Patients younger than 65 years with normal vital signs and normal lung exam may not require a CXR. Patients with URI symptoms, vital sign abnormalities, and abnormal lung findings should have imaging.
– For imaging, US can be beneficial. Patients with high likelihood of pneumonia and negative CXR, such as those with immunosuppression, dehydration, and older age, may need additional imaging such as CT chest.
– Clinical scores can assist in risk stratification and disposition, but they should only be used in association with clinical judgment and gestalt.
– Patient social situation, substance abuse history, and PO tolerance should be taken into consideration.
References/Further Reading:
- Halm EA, Teirstein AS. Management of community acquired pneumonia. N Engl J Med 2002;347:2039-45.
- Clinical Classifications for Health Policy Research: Hospital Inpatient Statistics, 1996. Rockville, MD, Agency for Health Care Policy and Research. HCPR publication no. 99-0034; 1999.
- National Vital Statistics Report: Deaths: Final Data for 2011. Vol 63, No. 3, 2013. http://www.cdc.gov/nchs/data/nvsr/nvsr63/nvsr63_03.pdf. Accessed October 07, 2016.
- gov – Hospital Compare. https://www.medicare.gov/hospitalcompare/search.html (Accessed on April 19, 2016).
- Kalil AC, Metersky ML, Klompas M, Muscedere J, Sweeney DA, Palmer LB, et al. Management of Adults With Hospital-acquired and Ventilator-associated Pneumonia: 2016 Clinical Practice Guidelines by the Infectious Diseases Society of America and the American Thoracic Society. Clinical Infectious Diseases 2016;63(5):1-51.
- Mandell LA, Wunderink RG, Anzueto A, Bartlett JG, Campbell GD, Dean NC, Dowell SF, File TM Jr, Musher DM, Niederman MS, Torres A, Whitney CG; Infectious Diseases Society of America; American Thoracic Society. Infectious Diseases Society of America/American Thoracic Society consensus guidelines on the management of community-acquired pneumonia in adults. Clin Infect Dis. 2007 Mar 1;44 Suppl 2:S27-72.
- Wunderink RG, Waterer GW. Community-acquired pneumonia: pathophysiology and host factors with focus on possible new approaches to management of lower respiratory tract infections. Infect Dis Clin North Am 2004; 18:743.
- Strieter RM, Belperio JA, Keane MP. Host innate defenses in the lung: the role of cytokines. Curr Opin Infect Dis 2003; 16:193.
- Mason CM, Nelson S. Pulmonary host defenses and factors predisposing to lung infection. Clin Chest Med 2005; 26:11.
- Johansson N, Kalin M, Tiveljung-Lindell A, Giske CG, and Hedlung J. Etiology of community-acquired pneumonia: Increased microbiological yield with new diagnostic methods. Clin Infect Dis 2010; 50:202.
- Wunderink RG, Waterer GW. Community-acquired pneumonia. New Engl J Med 2014;370(6):543-51.
- de Roux A, Marcos MA, Garcia E, Mensa J, Ewig S, Lode H, Torres A. Viral community-acquired pneumonia in nonimmunocompromised adults. Chest 2004; 125:1343.
- Chow AW, Benninger MS, Brook I, Brozek JL, Goldstein EJC, Hicks LA, et al. IDSA clinical practice guidelines for acute bacterial rhinosinusitis in children and adults. Clin Infect Dis 2012 Mar 20;
- Maloney G, Anderson E, Yealy DM. Chapter 65: Pneumonia and Pulmonary Infiltrates. Tintinalli’s Emergency Medicine: A Comprehensive Study Guide, 8th http://accessemergencymedicine.mhmedical.com/content.aspx?bookid=1658§ionid=109429397. Accessed 03 October, 2016.
- Marrie TJ. Community-acquired pneumonia. Clin Infect Dis 1994; 18:501.
- Metlay JP, Kapoor WN, Fine MJ. Does this patient have community-acquired pneumonia? Diagnosing pneumonia by history and physical examination. JAMA 1997; 278:1440.
- Coley CM, Married TJ, Lave JR, et al. Processes and outcomes of care for patients with community-acquired pneumonia: results from the Pneumonia Patient Outcomes Research Team (PORT) cohort study. Arch Intern Med 1999 May 10;159(9):970-80.
- Rosh AJ. Diagnosing pneumonia by medical history and physical examination. Ann Emerg Med 2005 Nov;46(5):465-467.
- Claessens YE, Debray MP, Tubach F, Brun AL, Rammaert B, Hausfater P, Naccache JM, Ray P, Choquet C, Carette MF, et al. Early chest computed tomography scan to assist diagnosis and guide treatment decision for suspected community-acquired pneumonia. Am J Respir Crit Care Med 2015;192:974–982.
- Metlay JP, Fine JM. Testing strategies in the initial management of patients with community-acquired pneumonia. Ann Intern Med. 2003;138:109-118.
- Marrie TJ. Community-acquired pneumonia in the elderly. Clin Infect Dis. 2000 Oct;31(4):1066-78.
- Riquelme R, Torres, A, el-Ebiary M, de la Bellacasa JP, Estruch R, Mensa J et al. Community-acquired pneumonia in the elderly: A multivariate analysis of risk and prognostic factors. Am J Respir Crit Care Med 1996 Nov;154(5):1450-5.
- Metlay JP, Schulz R, Li YH, Singer DE, Marrie TJ, Coley CM et al. Influence of age on symptoms at presentation in patients with community-acquired pneumonia. Arch Intern Med 1997 Jul 14;157(13):1453-9.
- Fernandez-Sabe N, Carratala J, Roson B, Dorca J, Verdaguer R, Manresa F, Gudiol F. Community-acquired pneumonia in very elderly patients: causative organisms, clinical characteristics, and outcomes. Medicine (Baltimore) 2003 May;82(3):159-69.
- Singanayagam A, Chalmers JD, Hill AT. Severity assessment in community-acquired pneumonia: a review. Q J Med 2009;102:379-88.
- Syrja H, Broas M, Suramo I, Ojala A, Lahde S. High-resolution computed tomography for the diagnosis of community-acquired pneumonia. Clin Infect Dis. 1998;27:358-63.
- Bartlett JG, Mundy LM. Community-acquired pneumonia. N Engl J Med. 1995;333:1618-24.
- Self WH, Courtney DM, McNaughton DC et al. High discordance of chest x-ray and computed tomography for detection of pulmonary opacities in ED patients: implications for diagnosing pneumonia. Am J Emerg Med 2013;31:401-5.
- Hash RB, Stephens JL, Laurens MB, Vogel RL. The relationship between volume status, hydration, and radiographic findings in the diagnosis of community-acquired pneumonia. J Fam Pract. 2000;49:833-7.
- Hayden GE, Wrenn KW. Chest radiograph vs. computed tomography scan in the evaluation for pneumonia. J Emerg Med 2009 Apr;36(3):266-70.
- Fine MJ, Stone RA, Singer DE, Coley CM, Marrie TJ, Lave JR et al. Processes and outcomes of care for patients with community-acquired pneumonia: results from the Pneumonia Patient Outcomes Research Team (PORT) cohort study. Arch Intern Med 1999 May 10;159(9):970-80.
- Fine MJ, Auble TE, Yealy DM, Hanusa BH, Weissfeld LA, Singer DE, et al. A prediction rule to identify low-risk patients with community-acquired pneumonia. N Engl J Med 1997 Jan 23;336(4):243-50.
- Bourcier JE, Paquet J, Seinger M, Gallard E, Redonnet JP, Cheddadi F. Performance comparison of lung ultrasound and chest x-ray for the diagnosis of pneumonia in the ED. Am J Emerg Med. 2014 Feb;32(2):115-8.
- Hu QJ, Shen YC, Jia LQ, Guo SJ, Long HY, Pang CS, et al. Diagnostic performance of lung ultrasound in the diagnosis of pneumonia: a bivariate meta-analysis. Int J Clin Exp Med 2014 Jan 15;7(1):115-21.
- Chavez MA, Shams N, Ellington LE, Naithani N, Gilman RH, Steinhoff MC, et al. Lung ultrasound for the diagnosis of pneumonia in adults: a systematic review and meta-analysis Respir Res. 2014 Apr 23;15:50.
- Pauker SG, Kassirer JP. The threshold approach to clinical decision making. N Engl J Med. 1980;302:1109-17.
- Salkind AR, Cuddy PG, Foxworth JW. The rational clinical examination. Is this patient allergic to penicillin? An evidence-based analysis of the likelihood of penicillin allergy. JAMA. 2001;285:2498-505.
- Cohen ML. Epidemiology of drug resistance: implications for a post-antimicrobial era. Science. 1992;257:1050-5.
- Gonzales R, Bartlett JG, Besser RE, et al. Principles of appropriate antibiotic use for treatment of uncomplicated acute bronchitis: background. Ann Intern Med 2001; 134:521.
- Emerman CL, Dawson N, Speroff T, et al. Comparison of physician judgment and decision aids for ordering chest radiographs for pneumonia in outpatients. Ann Emerg Med 1991;20:1215.
- Graffelman AW, Cessie SL, Knuistingh Neven A, et al. Can history and exam alone reliably predict pneumonia? Fam Pract 2007;56:465.
- O’Brien WT, Rohweder DA, Lattin GE, et al. Clinical indicators of radiographic findings in patients with suspected community-acquired pneumonia: who needs a chest x-ray? J Am Coll Radiol 2006; 3: 703.
- Engle MF, Paling FP, Hoepelman AIM, van der Meer V, Oosterheert JJ. Evaluating the evidence for the implantation of C-reactive protein measurement in adult patients with suspected lower respiratory tract infection in primary care: a systematic review. Fam Pract 2012; 29: 383.
- Nolt BR, Gonzales R, Maselli J, et al. Vital-sign abnormalities as predictors of pneumonia in adults with acute cough illness. Am J Emerg Med 2007; 25: 631.
- Kamath A, Pasteur MC, Slade MG, et al. Recognising severe pneumonia with simple clinical and biochemical measurements. Clin Med 2003;3:54e6.
- Myint PK, Kamath AV, Vowler SL, Maisey DN, Harrison BD, British Thoracic Society. Severity assessment criteria recommended by the British Thoracic Society (BTS) for community-acquired pneumonia (CAP) and older patients. Should SOAR (systolic blood pressure, oxygenation, age and respiratory rate) criteria be used in older people? A compilation study of two prospective cohorts. Age Ageing 2006;35:286-91.
- Lim WS, van der Eerden MM, Laing R, et al. Defining community acquired pneumonia severity on presentation to hospital: an international derivation and validation study. Thorax 2003;58:377-82.
- Lim WS, Lewis S, Macfarlane JT. Severity prediction rules in community acquired pneumonia: a validation study. Thorax 2000;55:219-23.
- Shah BA, Ahmed W, Dhobi GN, Shah NN, Khursheed SQ, Haq I. Validity of pneumonia severity index and CURB-65 severity scoring systems in community acquired pneumonia in an Indian setting. Indian J Chest Dis Allied Sci. 2010 Jan-Mar;52(1):9-17.
- Aujesky D, Auble TE, Yealy DM, Stone RA, Obrosky DS, Meehan TP, et al. Prospective comparison of three validated prediction rules for prognosis in community-acquired pneumonia. Am J Med. 2005 Apr;118(4):384-92.
- Loke YK, Kwok CS, Niruban A, Myint PK. Value of severity scales in predicting mortality from community-acquired pneumonia: systematic review and meta-analysis. Thorax 2010;65:884-890.
- Capelastegui A, España PP, Quintana JM, et al. Validation of a predictive rule for the management of community-acquired pneumonia. Eur Respir J. 2006;27(1):151-7.
- Yealy DM, Auble TE, Stone RA, Lave JR, Meehan TP, Graff LG, et al. Effect of increasing the intensity of implementing pneumonia guidelines: a randomized, controlled trial. Ann Intern Med. 2005 Dec 20;143(12):881-94.
- Renaud B, Coma E, Labarere J, Hayon J, Roy PM, Boureaux H. Routine use of the Pneumonia Severity Index for guiding the site-of-treatment decision of patients with pneumonia in the emergency department: a multicenter, prospective, observational, controlled cohort study. Clin Infect Dis. 2007 Jan 1;44(1):41-9.
- Carratalà J, Fernández-Sabé N, Ortega L, Castellsagué X, Rosón B, Dorca J, et al. Outpatient care compared with hospitalization for community-acquired pneumonia: a randomized trial in low-risk patients. Ann Intern Med. 2005 Feb 1;142(3):165-72.
- Atlas SJ, Benzer TI, Borowsky LH, et al. Safely increasing the proportion of patients with community-acquired pneumonia treated as outpatients. Arch Intern Med 1998;158:1350–6.
- Subramanian DN, Musonda P, Sankaran P, Tariq SM, Kamath AV, Myint PK. Performance of SOAR (systolic blood pressure, oxygenation, age and respiratory rate) scoring criteria in community-acquired pneumonia: a prospective multi-centre study. Age Ageing. 2013 Jan;42(1):94-7.
- Man SY, Lee N, Ip M, Antonio GE, Chau SS, Mak P, et al. Prospective comparison of three predictive rules for assessing severity of community-acquired pneumonia in Hong Kong. Thorax 2007;62:348-53.
- Ewig S, Kleinfeld T, Bauer T, Seifert K, Schäfer H, Göke N. Comparative validation of prognostic rules for community- acquired pneumonia in an elderly population. Eur Respir J 1999;14:370-5.
- Buising KL, Thursky KA, Black JF, MacGregor L, Street AC, Kennedy MP, et al. A prospective comparison of severity scores for identifying patients with severe community acquired pneumonia: reconsidering what is meant by severe pneumonia. Thorax 2006;61:419-24.
- Roson B, Carratala J, Dorca J, Casanova A, Manresa F, Gudiol F. Etiology, reasons for hospitalization, risk classes, and outcomes of community-acquired pneumonia in patients hospitalized on the basis of conventional admission criteria. Clin Infect Dis 2001;33:158-65.
- Furer V, Raveh D, Picard E, Goldberg S, Izbicki G. Absence of leukocytosis in bacteraemic pneumococcal pneumonia. Prim Care Respir J. 2011 Sep;20(3):276-81.
- Harper C, Newton P. Clinical aspects of pneumonia in the elderly veteran. J Am Geriatr Soc 1989;37:867-72.
- Gleckman R, Hibert O. Afebrile bacteremia. A phenomenon in geriatric patients. JAMA 1982;248:1478-82.
- Liu D, Su L, Guan W, Xiao K, Xie L. Prognostic value of procalcitonin in pneumonia: A systematic review and meta‐ Respirology (Carlton, Vic). 2016;21(2):280-288.
- Wacker C, Prkno A, Brunkhorst FM, Schlattmann P. Procalcitonin as a diagnostic marker for sepsis: a systematic review and meta-analysis. Lancet Infect Dis 2013 May;13(5):426-35.
- Simon L, Gauvin F, Amre DK, Saint-Louis P, Lacroix J. Serum procalcitonin and C-reactive protein levels as markers of bacterial infection: a systematic review and meta-analysis. Clin Infect Dis 2004 Jul 15;39(2):206-17.
- Maisel A, Neath S-X, Landsberg J, et al. Use of procalcitonin for the diagnosis of pneumonia in patients presenting with a chief complaint of dyspnoea: results from the BACH (Biomarkers in Acute Heart Failure) trial. European Journal of Heart Failure 2012;14(3):278-286.
- Bouadma L, Luyt CE, Tubach F, Cracco C, Alvarez A, Schwebel C, Schortgen F, et al. Use of procalcitonin to reduce patients’ exposure to antibiotics in intensive care units (PRORATA trial): a multicenter randomised controlled trial. Lancet 2010 Feb 6;375(9713):463-74.
- Jensen JU, Hein L, Lundgren B, Bestle MH, Mohr TT, Andersen MH, et al. Procalcitonin-guided interventions against infections to increase early appropriate antibiotics and improve survival in the intensive care unit: a randomized trial. Crit Care Med 2011 Sep;39(9):2048-58.
- Schuetz P, Müller B, Christ-Crain M, et al. Procalcitonin to initiate or discontinue antibiotics in acute respiratory tract infections. Cochrane Database Syst Rev 2012;CD007498.
- Flanders SA, Stein J, Shochat G, et al. Performance of a bedside C-reactive protein test in the diagnosis of community-acquired pneumonia in adults with acute cough. Am J Med 2004; 116:529.
- Almirall J, Bolíbar I, Toran P, et al. Contribution of C-reactive protein to the diagnosis and assessment of severity of community-acquired pneumonia. Chest 2004; 125:1335.
- Diehr P, Wood RW, Bushyhead J, Krueger L, Wolcott B, Tompkins RK. Prediction of pneumonia in outpatients with acute cough—a statistical approach. J Chronic Dis 1984;37:215-25.
- Macfarlane J, Holmes W, Gard P, Macfarlane R, Rose D, Weston V, et al. Prospective study of the incidence, aetiology and outcome of adult lower respiratory tract illness in the community. Thorax 2001;56:109-14.






2 thoughts on “emDocs Cases: ED Evaluation of Community-Acquired Pneumonia”
Pingback: Länkar v20 | Internmedicin
Pingback: emDOCs.net – Emergency Medicine EducationCorticosteroids for Pneumonia: Ready for Primetime? - emDOCs.net - Emergency Medicine Education