Author: Brit Long (@long_brit, EM Attending Physician, San Antonio, TX) and Michael Vivirito, RN, CEN (Joint Base Elmendorf Richardson Medical Center, Emergency Medicine) // Edited by: Alex Koyfman, MD (@EMHighAK)
You have just diagnosed a 42-year-old female with pneumonia. She has had four days of fever and productive cough, but otherwise she has normal vital signs and appears well. Her chest X-ray shows a right middle lobe pneumonia, she is PO tolerant, and you have been able to obtain follow-up. You recently heard of several studies evaluating corticosteroids for pneumonia. You have already written for her antibiotics, but are steroids warranted too?
This post will evaluate the current literature behind steroid use in pneumonia.
Community-acquired pneumonia (CAP) is a common infection evaluated and managed in the ED. For more on CAP, see this emDocs post. At the lung level, CAP includes inflammation resulting in fluid in the alveoli and impairing oxygen delivery. The body’s natural immune response includes formation and release of cytokines, which result in other patient symptoms such as fevers, chills, and rigors.
Corticosteroids are potent anti-inflammatory agents that are used as adjunctive treatment for a variety of conditions (i.e. meningitis, gout, asthma/COPD, severe sepsis, etc.). These agents can attenuate local and systemic inflammatory responses and decrease cytokine activity. Several recent studies, including randomized controlled trials (RCTs) and meta-analyses, have evaluated the use of corticosteroids as adjunctive treatment and the effect on mortality during hospitalization, duration of hospitalization, mechanical ventilation time, incidence of ARDS, and adverse effects from the therapy.1-7
Let’s start our deep dive…
1. Wu et al., AJEM 2017: Meta-analysis including 7 RCTs, with 592 patients. Goal to evaluate clinical efficacy with respect to mortality, length of hospital stay, and length of mechanical ventilation. All included studies evaluated patients receiving antibiotics, with included patients randomized to steroids versus placebo.
– Steroids were associated with reduced mortality (5.8%, 17 out of 293) versus placebo (12.04%, 36 of 299 patients), with relative risk (RR) for mortality 0.49 (95% CI 0.29-0.85).
– Patients receiving steroids also demonstrated decreased length of stay versus the group receiving placebo (weighted mean difference (WMD) -4.21 days, 95% CI -6.61 – -1.81), with no difference in duration of mechanical ventilation.
– Limitations: Several different doses and therapy durations were included for steroids. The meta-analysis also included studies with differing inclusion and exclusion criteria, resulting in significant heterogeneity.
2. Bi et al., PLos ONE 2016: Meta-analysis including 8 RCTs with 528 patients. Steroids included hydrocortisone 200-300mg/day, prednisolone/methylprednisolone 20-50mg/day, methylprednisolone 1mg/kg/day. Evaluated all-cause mortality, length of stay, development of ARDS, and need for mechanical ventilation.
– Mortality was decreased in patients receiving steroids, with relative risk 0.46 (95% CI 0.28 to 0.77), though steroids given for over 5 days demonstrated the greatest mortality reduction.
– Length of stay was reduced by over 4 days, as well as decreased need for mechanical ventilation (RR 0.50, 95% CI 0.27 – 0.92) and decreased risk of ARDS (RR 0.23, 95% CI 0.07 – 0.80).
– Adverse Effects: Patients receiving steroids demonstrated no increase in hyperglycemia (RR 1.03, 95% CI 0.61 – 1.72) or GI bleeding (RR 0.66, 95% CI 0.19 – 2.31).
– Limitations included a wide variation in length of treatment with steroids (1-9 days, with mean 5 days), with different steroids evaluated.
3. Siemieniuk et al., Ann Intern Med 2015: Meta-analysis including 12 RCTs with 1974 patients. Six of the 12 included studies evaluated patients with severe pneumonia (388 patients). Steroids included dexamethasone, prednisone, prednisolone, methylprednisolone, or hydrocortisone ranging from 1 to 10 days.
– Overall, groups receiving steroids demonstrated 5.3% mortality rate versus 7.9% in the placebo groups.
– In patients with severe pneumonia, mortality was decreased with RR 0.39 (95% CI 0.20-0.77). In patients not meeting criteria for severe pneumonia, no difference was found in mortality with steroids (RR 1.00, 95% CI 0.79 – 1.26).
– Patients receiving steroids in the setting of severe pneumonia also demonstrated faster time to clinical stability and decreased length of stay.
– Risk of ARDS was decreased in patients receiving steroids, with RR 0.24 (95% CI 0.10 – 0.56), as was need for mechanical ventilation with RR 0.45 (95% CI 0.26-0.79).
– Limitations: Similar to prior meta-analyses, steroid doses and routes of administration varied.
– Adverse Effects: For patients receiving steroids, investigators found an increased risk of hyperglycemia requiring treatment (RR 1.49, 95% CI 1.01 – 2.19). Results did not suggest difference in neuropsychiatric abnormalities or need for rehospitalization.
4. Shaqif et al., JHM 2013: Meta-analysis with 8 RCTs and 1119 patients. Steroid included use of methylprednisolone or equivalent doses below 2mg/kg/day.
– This meta-analysis suggested no difference in mortality, though decreased incidence of shock (RR 0.12, 95% CI 0.03 – 0.41) and reduced occurrence of chest radiograph findings (RR 0.13, 95% CI 0.06 – 0.27) were found in patients receiving steroids.
– No change in ICU length of stay was found, though total hospital length of stay was decreased in the steroid group (RR -1.21 days, 95% CI: -2.12 – -0.29).
– Limitations: Mechanical ventilation included invasive and noninvasive measures, with increased noninvasive measures in patients with steroids. Studies varied significantly with regard to patient comorbidities, illness severity, and duration of follow-up. Varied corticosteroid regimens were included.
– Adverse Effects: One included study suggested higher risk of hyperglycemia, while 3 others demonstrated no difference.
5. Blum et al., Lancet 2015: This double-blind, multicenter, randomized, placebo-controlled trial included 785 patients greater than age 18 years with CAP. Patients were randomized to prednisone 50 mg daily for 7 days versus placebo. Primary outcome included time to clinical stability (stable vital signs for 24 hours).
– Time to clinical stability was shorter in the steroid group (median time 3.0 vs. 4.4 days, hazard ratio [HR] 1.33, 95% CI 1.15-1.50).
– Complications associated with pneumonia did not differ between the groups (odds ratio [OR] 0.49, 95% CI 0.23-1.02). However, rates of in-hospital hyperglycemia were higher in the steroid group (OR 1.96, 95% CI 1.31-2.93).
6. Torres et al., JAMA 2015: This was a multicenter, randomized, double-blind, placebo-controlled trial conducted in over 100 patients with severe community acquired pneumonia and CPR greater than 150 mg/L at admission. Patients with uncontrolled diabetes, immunocompromised state, recent upper GI bleed (90 days), and H1N1 influenza were excluded. Patients received methylprednisolone 0.5 mg/kg IV over 12 hours for 5 days within 36 hours of admission. Outcomes included development of shock, need for mechanical ventilation, death within 72 hours or composite outcome of late treatment failure (radiographic progression, continued respiratory failure, development of shock, need for mechanical ventilation, and early and late treatment failure).
– Steroids reduced treatment failure (difference 18%, OR 0.34, 95% CI 0.14-0.87). However, in-hospital mortality did not differ.
What about for patients with lower respiratory tract infection but no pneumonia?
7. Hay et al., JAMA 2017: This multicenter, placebo-controlled, RCT evaluated oral prednisolone in 401 adult patients with acute lower respiratory infections (defined by cough and at least 1 other lower respiratory tract symptom), specifically duration and illness severity. Patients were not included if they had asthma. Included patients did not receive antibiotics. The steroid included prednisolone 40 mg daily for 5 days. Primary outcome was duration of moderately bad or worse cough and mean severity of symptoms on days 2-4.
– No change in cough duration or mean symptom severity was present between the steroid or placebo groups. No serious adverse events were found.
– However, this study included patients not receiving antibiotics. We chose to include this study, though the patient population differs from other studies (which consist of patients with pneumonia).
With these studies, what should the emergency physician do with steroids?
Recommendations
– CAP can be deadly, and the immune and inflammatory systems are responsible for clearing the infection. Unfortunately, an excessive immune response can be harmful, resulting in pulmonary dysfunction, ARDS, sepsis, and mortality.
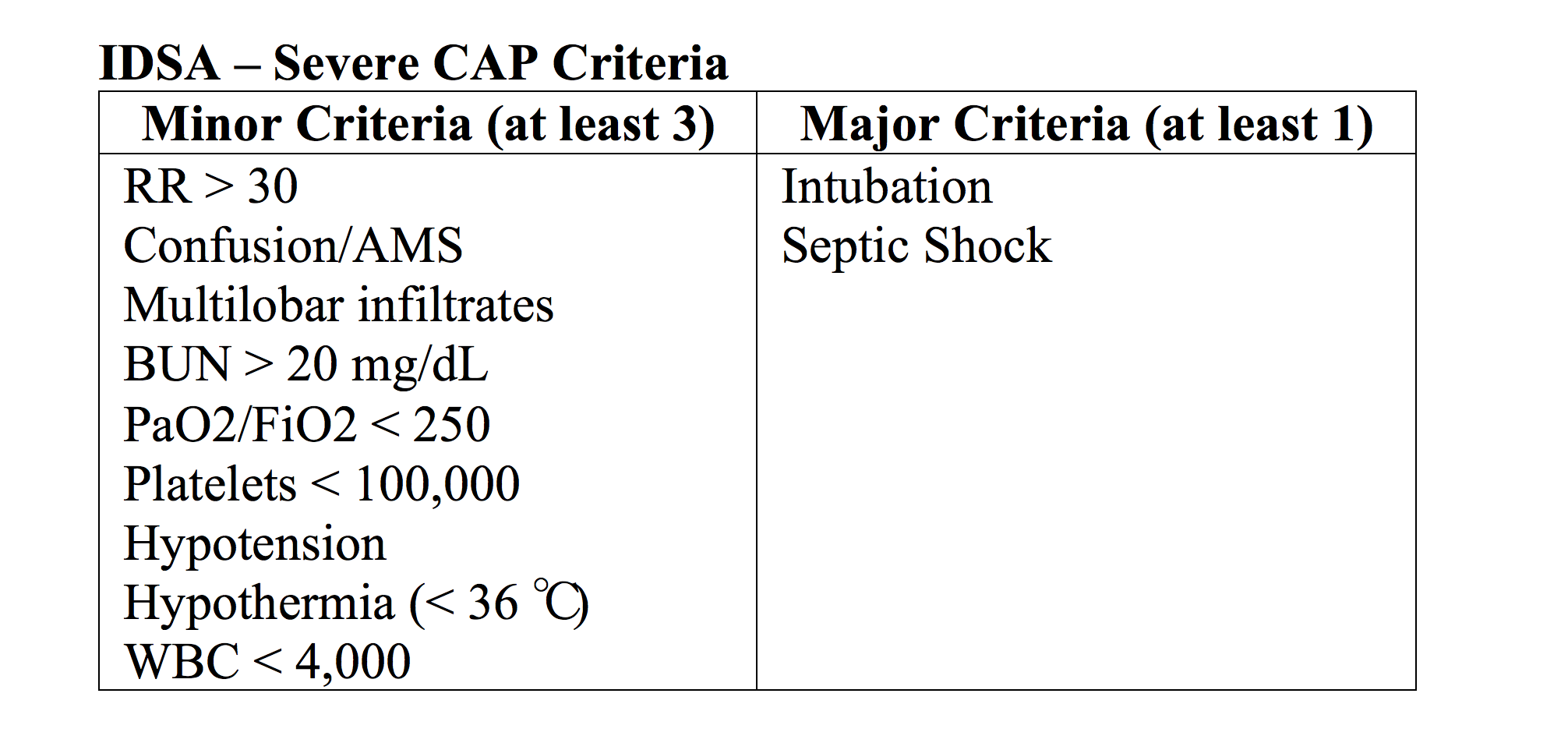
– Recent literature suggests benefit of adjuvant corticosteroid treatment for CAP. Steroids may be initiated in the ED, especially for severe CAP (Table 1 for severe CAP).8
– In severe CAP, steroids can reduce treatment failure and mortality. They may decrease length of stay, need for mechanical ventilation, and ARDS.
– Treatment with steroids for patients with CAP not meeting criteria for severe PNA is more controversial. Steroids may reduce mortality, length of stay, ARDS, and mechanical ventilation, but more study is needed.
– Contraindications for initiating treatment include diabetes, immunodeficiency from HIV, cancer, immunomodulatory medications, vasculitis, chronic peptic ulcers, and recent upper GI bleed.
– Proposed treatment should be discussed with the intensivist during the consultation and admission process. Further study is required for outpatient therapy.
References/Further Reading
- Wu W, Fang Q, He G. Efficacy of corticosteroid treatment for severe community-acquired pneumonia: a meta-analysis. American Journal of Emergency Medicine 2017; doi: 10.1016/j.ajem.2017.07.050.
- Bi J, Yang J, Wang Y, et al. Efficacy and safety of adjunctive corticosteroids therapy for severe community-acquired pneumonia in adults: an updated systematic review and meta-analysis. PloS ONE 2016; doi: 10.1371/journal.
- Siemieniuk R, Meade M, Alonso-Coello P, et al. Corticosteroid therapy for patients hospitalized with community-acquired pneumonia: a systematic review and meta-analysis. Ann Intern Med 2015; 163:519-528.
- Shafiq M, Mansoor M, Khan A, et al. Adjuvant steroid therapy in community-acquired pneumonia: a systematic review and meta-analysis. JHM 2013; 8(2):68-75.
- Blum CA, Nigro N, Briel M, et al. Adjunct prednisone therapy for patients with community-acquired pneumonia: a multicentre, double-blind, randomised, placebo-controlled trial. Lancet 2015;385:1511-1518.
- Torres A, Sibila O, Ferrer M, et al. Effect of corticosteroids on treatment failure among hospitalized patients with severe community-acquired pneumonia and high inflammatory response: a randomized clinical trial. JAMA 2015; 313(7):677-686.
- Hay A, Little P, Harnden A, et al. Effect of oral prednisolone on symptom duration and severity in nonasthmatic adults with acute lower respiratory tract infection: a randomized clinical trial. JAMA 2017; 318(8):721-730.
- Mandell LA, Wunderink RG, Anzueto A, et al; Infectious Diseases Society of America; American Thoracic Society. Infectious Diseases Society of America/American Thoracic Society consensus guidelines on the management of community-acquired pneumonia in adults. Clin Infect Dis. 2007 Mar 1;44 Suppl 2:S27-72.





2 thoughts on “Corticosteroids for Pneumonia: Ready for Primetime?”
Pingback: SGEM#216: Pump It Up – Corticosteroids for Patients with Pneumonia Admitted to Hospital | The Skeptics Guide to Emergency Medicine
Pingback: Emergency Management of Community Acquired Pneumonia | EM Cases