
Author: David R. Bussé, MD/MBA (EM Resident Physician, UTSW / Parkland) // Edited by: Alex Koyfman, MD (@EMHighAK) and Brit Long, MD (@long_brit)
Case
A 31-year-old African American male with a past medical history of hypertension is brought in by EMS into the trauma bay of your emergency department. It is the 4th of July, and per EMS, they were called by the patient’s wife when she noticed that he had sustained burns to both of his hands and face after having gone to inspect a mortar on the ground that had failed to ignite. Initial vital signs are T 36.8 C, HR 112, BP 147/98, SpO2 98%. Initial primary survey confirms patient stability. The patient does not endorse voice changes or shortness of breath. He does, however, state that he is having marked blurry vision. Your secondary survey reveals superficial partial thickness burns to the face as well as singed facial hairs. You note a chemotic left orbit with significant clear fluid building along the lower eyelid. You also note bilaterally open dislocations to both of his thumbs at the IP joints. After confirming that he is neurovascularly intact, you send him for bilateral hand radiographs, and request fluorescein to further examine his eyes.
Introduction
While exhilarating and entertaining, fireworks displays and the hazards they pose are a common cause of morbidity and mortality nationwide. In 2017, the United States Consumer Product Safety Commission reported that an estimated 12,900 people were treated in hospital EDs for firework-related injuries. To date, this has been the peak year for firework-related injuries of this decade, surpassing both 2015 (11,900) and 2013 (11,400) [1, 2, 3]. Nonetheless, this is a trend that has persisted since 1999. Most commonly affected are males, particularly in the 25-44 year age group. 65% of injuries occurred during the 4th of July holiday [1].

As demonstrated in Figure 1, firework-related injuries commonly result from legal fireworks and disproportionately affect children and males [2]. More specifically, children are most affected by rocket injuries. Not surprisingly, teenagers and young adults tend to be most affected by homemade fireworks. Shells/mortars are the most common cause of injuries in adults, followed closely by sparklers [2, 4]. Bystanders are most frequently affected by aerial-type fireworks.
Following initial evaluation in an emergency department, the majority of injuries (81%) are discharged directly, requiring only thorough cleaning and primary suturing [2, 3, 5]. For those requiring an inpatient stay, Figure 1 also demonstrates the distribution of disposition decisions. Among those injuries requiring hospitalization, the majority were attributable to federally illegal devices or homemade devices [2].

According to the 2018 fireworks annual report, the most common firework-related injuries include burns to the fingers, hand, and wrist (28%) followed by injuries to the eye (19%), then by open injuries to the hand and wrist (7%) [1, 3, 6]. The dominant hand tends to sustain more injuries as the patient holds the device in that hand after lighting it in order to place or throw it [5].
Mechanism of Injury
Firework injuries result from multiple causes. Injury may result from misuse (holding a firework in one’s hand while it explodes), device malfunction, failure to withdraw quickly enough from the blast, or from simply being a bystander. These may range from superficial burns to mangling injuries that involve skin, muscle, tendon, nerve, blood vessel, and bone, even resulting in traumatic amputations. However, even fairly superficial injuries may be complex. Both explosive pressure and released particles driven into tissues cause damage [5, 6]. In addition, tissues will react differently to blast injuries; bones may be crushed while nerves and vessels may be stretched and contused. Fractures will occur when the vibration of the blast component causes the phalanges to break while the distal volar plates of the interphalangeal joints (IPJs) give way, resulting in dislocations and avulsion fractures [5].

Figure 3. Blast injury to left 1st volar webspace with amputation of 2nd and 3rd digits proximal to the PIP joints following premature explosion of a firecracker. https://radiopaedia.org/cases/blast-injury-to-hand?lang=us
The explosive device is typically held in the patient’s dominant hand. This frequently results in a pattern of hyperextension and hyperabduction most commonly affecting the thumb, radial palm, and digits [4, 5, 6]. Severe soft tissue injury to the first webspace and palm are often associated with soft tissue avulsion and amputation. Shells/mortars cause the highest proportion of severe injuries, disproportionately injuring the face, brain, and hands [2]. They also result in more permanent impairment than other firework types as a result of eye and hand injuries.
Patient Evaluation
The examination must begin with a basic primary survey. Once the patient has been stabilized, fully examine the body to identify signs of injury. Understanding the energy of the blast is critical to predicting and evaluating the full extent of injury [6]. This begins with a detailed history. Question the patient or witnesses about the nature of the device, as well as to how the device was used. Be sure to also inquire about the patient’s occupation and hand dominance as this will impact the treatment plan.
While outside the scope of this article, a thorough HEENT exam should be performed, as injuries to the face and eye are common. For a review of the exam as well as injury management, please see the following Mayo Clinic article as well as these two brief summaries from Life in the Fast Lane. In brief, a teardrop pupil, hyphema, proptosis, or extraocular movement limitation on exam signal the presence of serious pathology requiring emergent management [7].
Physical examination of the injured extremities follows. For a brief review of how to perform an examination of the distal upper extremity, please see this emDocs article. As with any injury of an extremity, be systematic in the evaluation and communication of these injuries. Among operative hand injuries, fireworks most commonly fracture the thumb, destabilize the thumb CMC joint, and deeply damage the first web space [4]. Partial and complete amputations are described by the digits involved and the level at which they occur. Examine each digit individually for digital nerve or artery injury. Consider the total surface area involved, including how proximal or distal lacerations extend and whether the injuries are palmar, dorsal, or both. Finally, assess the depth of injury. Is there exposed subcutaneous tissue, tendon, muscle or bone? If intact soft tissue appears deeply contused, suspect deeper injury [6].
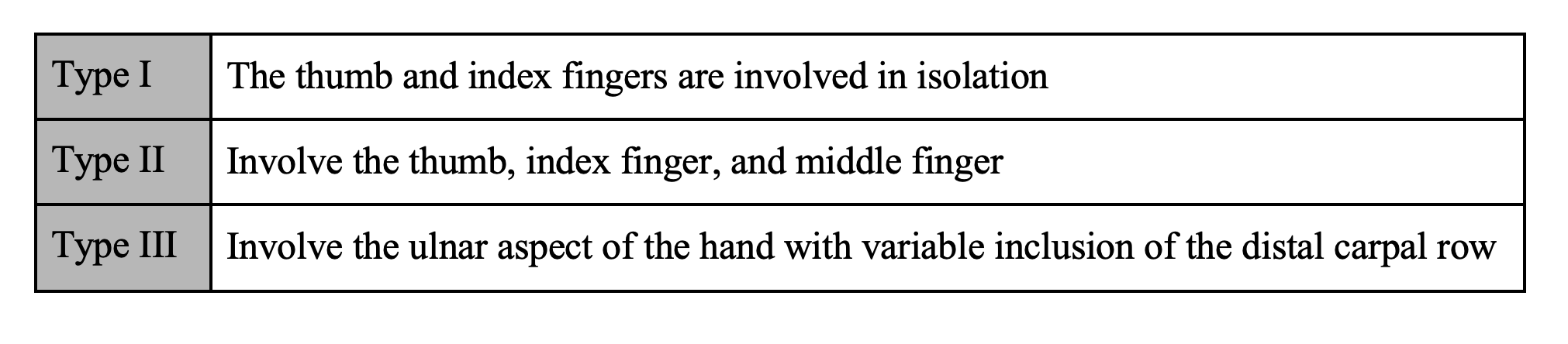
Among injury classification schemes, a system proposed by Yasmeh et al. classifies injuries based on the extent of involvement of the hand [1]. They propose that such a classification system makes for expedited communication with a hand surgeon.
Radiographs are a necessary component of any distal extremity evaluation, looking specifically for fractures and dislocations. Large zones of soft tissue avulsion or laceration serve as harbingers of potential joint instability [6], for which evaluation under fluoroscopy by a surgeon is recommended. Moreover, the degree of comminution at the fracture sites, especially those about joints, may influence the decision for salvage [6].
Management
Treatment should focus on debridement of non-viable tissue and maximizing long-term function [5, 6], which does not necessarily require salvage of all parts. Begin by irrigating the wound, administering IV antibiotics, and updating tetanus status as needed. Attempt to control bleeding with compression rather than an extremity tourniquet [6].
Depending on the extent of injury, patients may require transfer for management under the direction of a hand surgeon. For patients presenting with denuding and degloving injuries of the fingers with exposed bone, the patient should undergo revision (trimming) of the amputation to ensure that there is sufficient skin and soft tissue coverage of the bone [5]. Dislocation reduction and splinting may also be required. Prior to transfer, efforts should be made to cover all white structures (bone, tendon, nerve, vessel) where possible [6]. Treatment begins in the ED, but the patient should be made aware that treatment will likely occur in several stages under the guidance of a specialized surgeon, with several weeks to months of rehabilitation and recovery.
Case Conclusion
Upon fluorescein staining of the patient’s eyes, you note a positive Seidel’s sign in the left eye. X-rays confirm bilateral open dislocations of patient’s thumb at the 1st IP joints without evidence of fracture or foreign body. While consulting ophthalmology for what you suspect is a ruptured globe, you administer a liter of normal saline, update the patient’s tetanus vaccine, and start cefazolin and cefepime. You also administer fentanyl and perform a digital nerve block of the patient’s thumbs bilaterally. Thorough irrigation of both thumbs is performed with normal saline mixed with betadine. You quickly reduce both thumb dislocations and perform a close, widely spaced closure of the overlying laceration to keep the underlying bone from desiccating. Thumb spica splints are placed on each of the patient’s forearms just in time for ophthalmology to whisk him away to the operating room.
Key Points
- Firework-related injuries are a major source of ED visits nationwide.
- All patient evaluations begin with a thorough history and physical exam once stabilized.
- Obtain radiographs to evaluate for fractures and dislocations. Large areas of soft tissue injury should signal sites of possible joint instability.
- Thoroughly irrigate all wounds. Administer IV antibiotics and update tetanus as needed.
- Thorough cleaning and primary suturing are sufficient management strategies for the majority of these injuries.
- For patients with more extensive injuries, perform amputation revisions as needed in order to provide sufficient skin coverage to exposed bone. Similarly, provide skin coverage to tendons, nerves, and blood vessels to prevent desiccation.
- Reduce and splint any joint/fracture dislocations.
- Transfer for more specialized hand care when necessary.
References/Further Reading
- Yasmeh, S., et al. Firework-related hand injuries: A novel classification system. The American Journal of Emergency Medicine. 2018 May; 36(5): 897-899.
- Sandvall, B.K., et al. Fireworks type, injury pattern, and permanent impairment following severe fireworks-related injuries. The American Journal of Emergency Medicine. 2017 October; 35(10): 1469-1473.
- Tu, Y. and J. Ng. Fireworks-Related Deaths, Emergency Department-Treated Injuries, and Enforcement Activities During 2018. 2018 Fireworks Annual Report. 2019 June.
- Sandvall, B.K., et al. Severe Hand Injuries From Fireworks: Injury Patterns, Outcomes, and Firework Types. The Journal of Hand Surgery. 2017 May; 42(5): 385-393.
- Pilling, T. and P. Govender. Profile and management of the firework-injured hand. South African Family Practice. 2016 Jan; 58(2): 48-53.
- Saucedo, J. M. and N. B. Vedder. Firework-Related Injuries of the Hand. The Journal of Hand Surgery. 2015 Feb; 40(2): 383-387.
- Bellew, S. Save face: Managing facial trauma in the emergency department. EM Blog Mayo Clinic. 2014 Nov. <https://emblog.mayo.edu/2014/11/10/save-face-managing-facial-trauma-in-the-emergency-department/>




