Authors: Alin Gragossian, DO (EM Resident Physician, Drexel University), Matthew A. Varacallo, MD (Orthopedics Resident Physician, Drexel University), and Richard J. Hamilton, MD (EM Professor and Chair, Drexel University) // Edited by: Erica Simon, DO (@E_M_Simon) & Alex Koyfman, MD (@EMHighAK, EM Attending Physician, UT Southwestern Medical Center / Parkland Memorial Hospital)
A 31-year-old male, the victim in a low-speed MVC versus pedestrian, arrives to the trauma bay via EMS. As the stretcher rolls by you see an alert patient, yelling in pain. A c-collar is in place, and a splint supports what appears to be a mangled right hand and an open right forearm fracture. As your trauma team hurriedly connects monitors, you note initial VS: HR 110, BP 132/96, RR 14, SpO2 98% RA.
You’re reassured by your primary survey: ABCs are intact; the radial and ulnar pulses of both upper extremities are palpable. Your secondary survey is significant for what appears to be a serious injury to the dorsal aspect of the distal right upper extremity: a large skin avulsion revealing extensor tendons of the hand and an open distal radius fracture.
CT imaging and radiographs demonstrate that the patient is without additional injuries, save those identified on your exam. After administering analgesia, cefazolin, and updating a tetanus, the patient wheels off to the OR for washout, re-approximation, and repair. As you complete the trauma paperwork, you replay the hand examination in your mind. Was there anything that your team overlooked?
If it’s been a while since you’ve treated a patient with a hand complaint, let’s review some high-yield material.
Epidemiology
Hand complaints represent nearly 12% of injury-related visits to ED setting.1,2 Trauma involving the hands imparts a significant burden on healthcare systems given the frequent requirement for referral, and potential necessity for surgical intervention. According to a 2009 study of 134 patients presenting for the evaluation of hand lacerations secondary to electric saws, mean treatment costs per injury (including hospitalization) were $30,704, with an average loss of 64 productive work days.3 As limitations in dexterity can significantly impact activities of daily living and quality of life, the early identification and treatment of neurovascular, tendon, and bone injuries of the hand are paramount.4
History & Physical
History
When obtaining a history, question patients regarding the type of injury (burn, laceration, injection injury, etc.), the mechanism, time elapsed between injury and evaluation, and the possibility of occupational exposures. Hand dominance, prior hand injury, and prior hand surgeries should be documented.5
Physical Exam
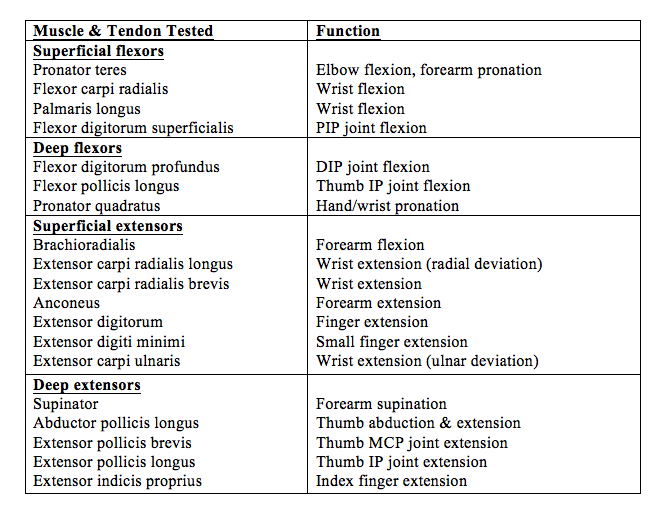
Table 1 offers a quick reference guide for use when performing muscle and tendon function evaluation of the hand and wrist.6,7
Nerves
Examination of the hand should include an assessment of nerve function:
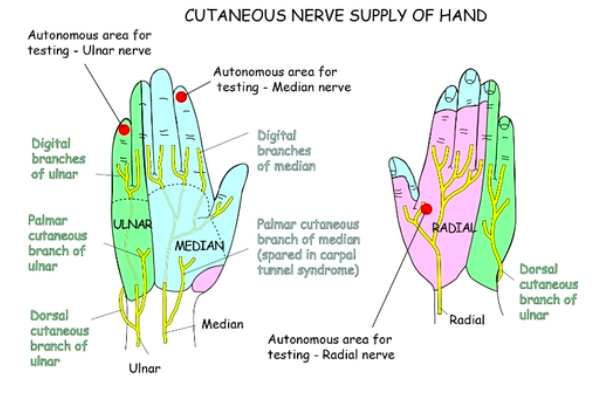
Median Nerve
- Motor: thumb abduction and opposition => test by asking the patient to place his hands in anatomic position. Apply resistance to the thumbs while prompting the patient to move them towards the ceiling.
- Sensory: innervates the central aspect of the palm and terminates distally in the radial 3.5 digits of the hand => test sensation by assessing two-point discrimination. Normal two-point discrimination is 5mm at the volar fingertips. Sensory testing should be repeated 2-4 times on each side of each digit.5,6
Radial Nerve
- Motor: thumb extension => test the patient’s thumb extension against resistance.
- Sensory: the superficial branch of the radial nerve and its terminal branches provide sensation to the central and radial aspects of the dorsum of the hand, and the dorsal-radial aspect of the thumb => test sensation by performing two-point discrimination on the dorsum of the thumb.5,6
Ulnar Nerve
- Motor: innervates the adductor pollicis muscles and controls thumb adduction => test by asking the patient to cross her fingers, or abduct her fingers against resistance.
- Sensory: provides sensation to the dorsal-ulnar aspect of the hand and into the fingertips of the fourth and fifth digits => test ulnar nerve sensation by assessing two-point discrimination of the fourth and fifth digits.5,6
O’Rahilly R. Basic Human Anatomy: Chapter 10: The Hand. 2008. Available from: https://www.dartmouth.edu/~humananatomy/about/credits.html
Vascularity
The radial and ulnar arteries perfuse the hand. The radial artery forms the deep palmar arch, and the ulnar artery forms the superficial palmar arch.5,7 Vascularity may be evaluated through palpation (temperature and pulses), Doppler (if required), and capillary refill. While some advocate the use of the Allen’s test during the vascular examination, it is important to note that this test lacks sensitivity and specificity as findings vary according to the time employed (e.g. – injury transecting the radial artery may initially present with a normal Allen’s test, however subsequent radial artery vasospasm and thrombosis may result in an later abnormal Allen’s test), and operator experience.8
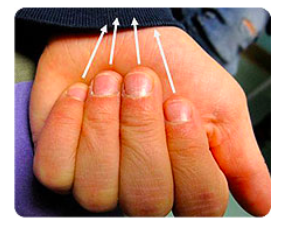
Alignment
When it comes to hand injuries, malrotation resulting from fracture is an indication for ED reduction. When the fingers are flexed, a cascade directed towards the scaphoid tubercle should be observed (Figure 2). If abnormalities in alignment are identified, radiographs and consultation are advised.
Steinman S. Seattle Children’s Hospital Finger Fractures: Don’t Forget the Malrotation. 2017. Available from: http://www.seattlechildrens.org/healthcare-professionals/resources/case-studies/finger-fractures-dont-forget-rotation/
Special Examinations
Carpal Tunnel
Tinel’s and Phalen’s tests may be utilized to assess for the presence of carpal tunnel syndrome. A positive Tinel’s sign is elicited when the examiner taps the median nerve as it passes through the carpal tunnel, eliciting a report of paresthesias in median nerve distribution. A positive Phalen’s test occurs when paresthesias are experienced in median nerve distribution after > 60 seconds of maximum wrist flexion.8
Ulnar Motor Weakness
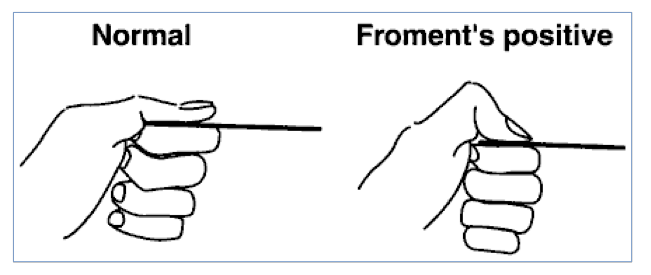
Froment’s test identifies ulnar nerve motor dysfunction (specifically, a weakness of the adductor pollicis). The patient is instructed to grasp a thin object between the thumb and radial aspect of the index finger. If the examiner is able to remove the thin object, or the patient flexes the IP joint (flexing the flexor pollicis longus, innervated by the anterior interosseous nerve) to increase the grasping force, the test is said to be positive. If the patient simultaneously hyperextends the first metacarpophalangeal joint, this is said to be a positive Jeanne’s test, again indicating ulnar motor weakness.9
Ujash S. Physical Exam of the Hand. 2017. Available from: http://www.orthobullets.com/hand/6008/physical-exam-of-the-hand

Ujesh, S. Physical Exam of the Hand. 2017. Available from: http://www.orthobullets.com/hand/6008/physical-exam-of-the-hand
Imaging
In the ABCs of Emergency Radiology, Chan and Touquet offer a number of excellent recommendations on the basics of ED radiographs:
The Rules of Two:1
- Two views: one view is one too few
- Two joints: image the joint above and below a long bone
- Two sides: compare the other side if unsure of pathology
- Two abnormalities: look for a second abnormality
- Two occasions: compare current films and old films (if available)
- Two visits: repeat films before and after procedures
- Two specialists: if possible, obtain a formal radiology report
- Two examination modalities: US, CT, or MRI should be considered as appropriate to the clinical scenario
Speaking of imaging, ultrasound is quickly becoming a popular mechanism for identifying foreign bodies. Prior to the employment of US, epidemiological studies estimate that nearly 38% of non-radiopaque foreign bodies went unidentified during initial ED encounters (1982 publication).11 A recent study by Saboo and colleagues demonstrated sensitivities of 94–98% for ultrasound detection of both radiolucent and radiopaque foreign bodies (n =123 patients, 7.5 MHz transducer).12 As US may be difficult to perform on the small surfaces of the hands, a water bath may be utilized with a high frequency linear transducer to generate high resolution images.

Lin, Michelle. Tricks of the Trade: Underwater Ultrasonography. 2011. Available from: https://www.aliem.com/2011/tricks-of-trade-underwater/
Urgent or Emergent Surgical Intervention
The following offers a review of hand conditions requiring urgent or emergent ED attention.
Acute Compartment Syndrome
Compartment syndrome of the hand is relatively uncommon, but may occur secondary to trauma, insect bites, snake bites (2-8%13), high-pressure injection, contrast infusion, and crush injuries.12 The hand is anatomically separated into ten compartments; those most commonly at risk for the development of elevated intra-compartmental pressures include: the interossei (dorsal and palmar), the thenar and hypothenar, the adductor, and the finger compartments.14 Symptoms associated with acute compartment syndrome are classically characterized as the “six Ps” – pain, pallor, paresthesias, poikilothermia, pulselessness, and paralysis. The most reliable indicator is pain out of proportion to physical examination findings.12 It is paramount that fasciotomy be performed within 8 hours of the onset of symptoms as axonal and myocyte damage may be irreversible outside of this time frame.15-17
Replantation
Replantation, the surgical reattachment of a finger, hand, or arm that has been severed, is a topic best discussed with the orthopedic/hand specialist – patient outcomes depend upon the skill of the surgical team, patient co-morbidities, and the extent of the injury.18 Primary indications for replantation after trauma include amputations to the thumb at any level, involvement of multiple digits, amputations through the palm, amputations at or proximal to the wrist, and almost all amputated parts in the pediatric patient.18 Consideration for replantation should be given for individual digit amputations distal to the insertion of flexor digitorum superficialis, ring avulsion injuries, and amputations through or above the elbow.18
Primary contraindications to replantation include patients with severe vascular disorders, crush injuries, or injuries with mangling of the severed limb.18
Flexor tenosynovitis
Flexor tenosynovitis is an infection of the flexor tendon sheath that is characterized by Kanavel’s Signs: finger held in flexion, pain with passive extension, pain with palpation of the flexor tendon sheath, and fusiform swelling.19 Flexor tenosynovitis may result from minor trauma as the distance from the volar dermis to the flexor sheath is 1-2 millimeters.19 If suspected, initiate broad-spectrum antibiotic therapy, and consult for surgical intervention.19
High-Pressure Injection Injuries
Patients utilizing high-pressure injection equipment often present to the ED for the evaluation of an injury to the non-dominant hand (equipment most commonly held in the dominant hand).20,21 Injury severity is dependent upon the force of injection, volume of material injected, and the composition of the material injected.20 While injuries may initially appear relatively benign, specialty consultation is a must as tracking of the injected material may ultimately result in gross contamination of subcutaneous tissue and deep muscle. Upon ED arrival, imaging should be performed to assess for the presence of foreign bodies, and parenteral antibiotic therapy initiated.20,21 In terms of morbiditiy, as compared to all other finger injuries, those due to high-pressure injection are three times as likely to require amputation.19
Pearls:
- A rapid hand exam can be performed in the following manner:
- As the patient make an “OKAY” sign with thumb and first finger (median nerve). Spread the fingers apart maximally (ulnar nerve). Dorsiflex the wrist fully (radial nerve). These can be combined into an OKAY sign with remaining fingers spread apart and the wrist dorsiflexed to get an all-in-one motor exam.
- Check sensation of the median and ulnar nerve by testing two-point discrimination at the index and small finger pads respectively. Radial nerve sensation can be tested over the dorsum of the thumb.
- For carpal tunnel syndrome, perform Tinel’s and Phalen’s tests. Remember, a positive test occurs when the patient reports paresthesias in median nerve distribution.
- Acute compartment syndrome must go to the OR within 8 hours of onset.
- Kanavel’s Signs are key physical exam findings for flexor tenosynovitis: finger held in flexion, pain with passive extension, pain with palpation of the flexor tendon sheath, and fusiform swelling.
- Beware of high-pressure injection injuries. They look more benign than they truly are, and warrant a careful physical examination of the hand and consultation.
References / Further Reading:
- Niska R, Bhuiya F, Xu J. National Hospital Ambulatory Medical Care Survey: 2007 emergency department summary. Natl Health Stat Report. 2010;(26):1-31.
- Maroukis BS, Chung KC, MacEachern M, Mahmoudi E. Hand trauma care in the United States: a literature review. Plastic and Recon Surg. 2016 Jan; 137(1): 100e-111e.
- Hoxie SC, Capo JA, Dennison DG, Shin AY. The economic impact of electric saw injuries to the hand. J. Hand Surg. 2009 Jun; 34A: 886-889.
- Soucacos P. Indications and selection for digital amputation and replantation. J Hand Surg Br. 2001;26(6):572–581.
- Tintinalli J, Stapczynski J, Cline D, Ma OJ et al. Tintinalli’s Emergency Medicine: A Comprehensive Study Guide, 8th edition. McGraw-Hill Education / Medical; 2015.
- Chung KC. Hand and Wrist Surgery. Elsevier Health Sciences; 2012.
- Morton DA, Foreman K, Albertine KH. eds. The Big Picture: Gross Anatomy New York, NY: McGraw-Hill; 2011.
- Jarvis MA, Jarvis CL, Jones PR, Spyt TJ. Reliability of Allen’s test in selection of patients for radial artery harvest. Ann Thorac Surg. 2000;70(4):1362-5.
- Ujash S. Physical Exam of the Hand. 2017. Accessed 15 March 2017. Available from: http://www.orthobullets.com/hand/6008/physical-exam-of-the-hand#
- Chan O and Touquet R. General Principles: How to Interpret Radiographs. In ABC of Emergency Radiology. 3rd 2013. West Sussex, UK. Wiley-Blackwell Publishing.
- Lewis D, Jivraj A, Atkinson P, Jarman R. My patient is injured: identifying foreign bodies with ultrasound. Ultrasound. 2015;23(3):174-80.
- Saboo S, Saboo SH, Soni SS, et al. High-resolution sonography is effective in detection of soft tissue foreign bodies. J Ultrasound Med 2009; 28: 1245–9.
- Anz A, Schweppe M, Halvorson J, Bushnell B, Sternberg M, Andrew Koman L. Management of venomous snakebite injury to the extremities. J Am Acad Orthop Surg. 2010 Dec; 18(12): 749-59.
- Chandraprakasam T and Kumar R. Acute compartment syndrome of forearm and hand. Indian J Plast Surg. 2011; 44(2):212-218.
- Oak NR, Abrams RA. Compartment Syndrome of the Hand. Orthop Clin North Am. 2016;47(3):609-16.
- Whitesides TE, Heckman MM. Acute compartment syndrome: update on diagnosis and treatment. J Am Acad Orthop Surg 1996;4(4):209–18. 21.
- Von keudell AG, Weaver MJ, Appleton PT, et al. Diagnosis and treatment of acute extremity compartment syndrome. Lancet. 2015;386(10000):1299-310.
- Sabapathy SR, Venkatramani H, Bharathi RR, Bhardwaj P. Replantation surgery. J Hand Surg Am. 2011;36(6):1104-10.
- Ong YS, Levin LS. Hand infections. Plast Reconstr Surg. 2009;124(4):225e-233e.
- Eroglu O, Sari E, Vural S, Coskun F. Warning: This may be as dangerous as firearm injuries; “grease-gun injury”: A case report. The Pan African Medical Journal. 2015;20:40. doi:10.11604/pamj.2015.20.40.5892.
- Hogan CJ, Ruland RT. High-pressure injection injuries to the upper extremity: a review of the literature. J Orthop Trauma. 2006;20(7):503-11.





2 thoughts on “The Hand: An Expedited Examination and Key Points Regarding ED Diagnoses”
Pingback: Handundersökning – Mind palace of an ER doc
Pingback: Christmas edition, December 27th 2019