Authors: Tim Montrief, MD (@EMinMiami); Jonathan Auerbach, MD (University of Miami/Jackson Memorial Hospital Emergency Medicine Residency Program) // Edited by: Alex Koyfman, MD (@EMHighAK) and Brit Long, MD(@long_brit)
Background
While the term necrotizing soft tissue infections (NSTIs) comprises a wide variety of severe infections, the term necrotizing fasciitis in particular refers to any NSTI involving the fascial planes.1A NSTI extending into the perineal, perianal, and genital area is termed Fournier’s gangrene (FG).2 FG has an incidence of 1.6 per 100,000 men in the United States, which peaks between the ages of 50-79 years (3.3 per 100,000) with the highest rates occurring in the South (1.9 per 100,000).3 In comparison, women have an incidence of 0.25 per 100,000.3 However, the incidence of FG is rising, likely due to an increase in the mean age of the population, in addition to increasing numbers of patients on immunosuppressive therapy or suffering from human immunodeficiency virus (HIV).3,4
The overall case fatality rate ranges from 7.5% to upwards of 50%.3,5,6 This is likely due to the fact that many of the published literature tends to be from tertiary referral centers reflecting a more severely ill population.5 Most hospitals (approximately 66% overall) care for no patients with FG during a given year, and only 1% of hospitals cared for ≥5 cases per year.5

Anatomy
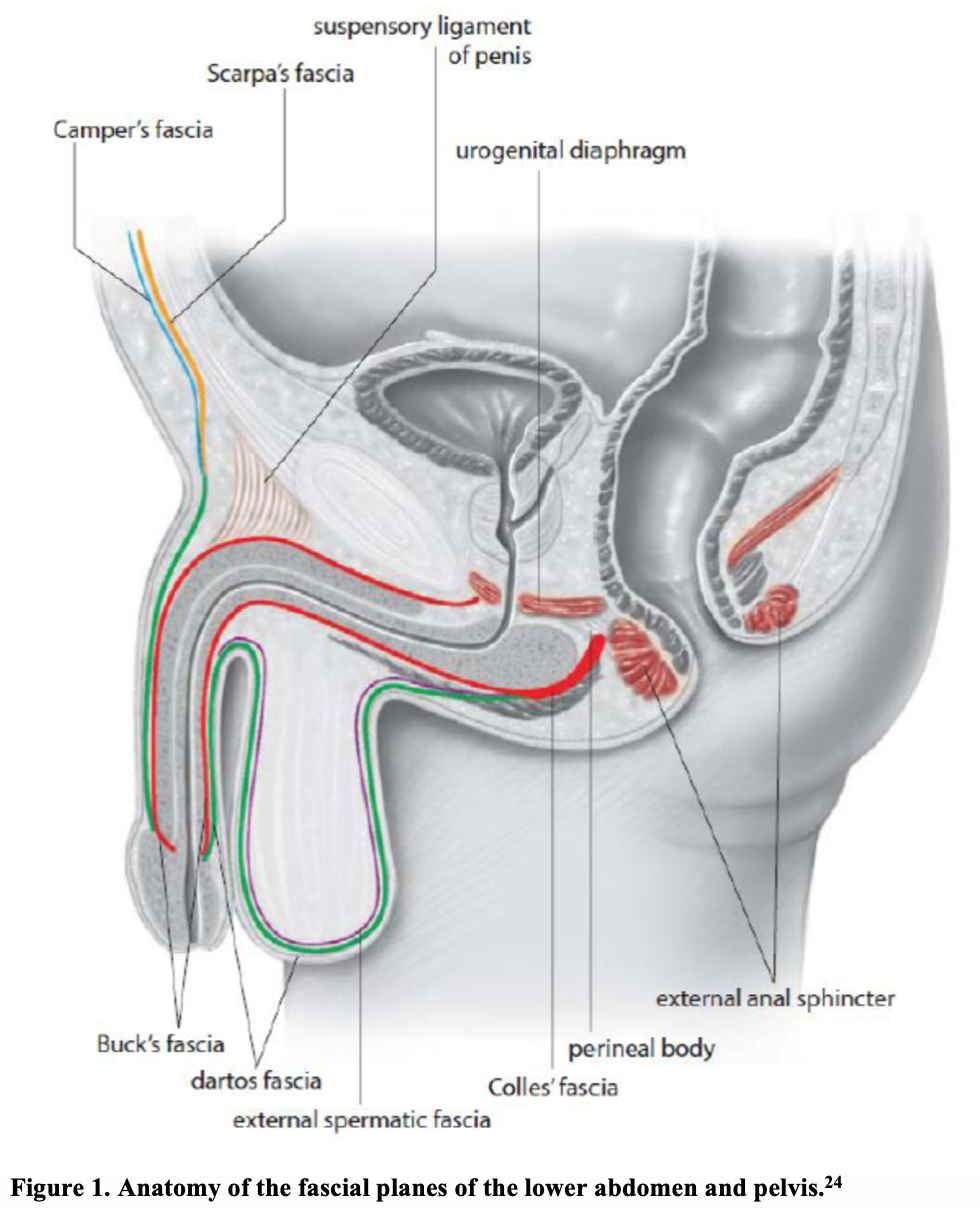
Understanding the fascial anatomy of the perineum allows a better understanding of how NSTIs that originate in the urogenital and perianal region (e.g. FG) spread to involve the abdomen, flank, and chest (Figure 1). As FG spreads across the superficial and deep fascial planes of the urogenital and perianal regions, this deep tissue infection leads to local vascular occlusion, ischemia, and tissue necrosis.15 This hypoxia leads to infarction of surrounding nerves that initially is painful, but eventually causes localized anesthesia.16 The superficial skin is often spared during the initial stages of infection, whereas the necrotizing process spreads along the fascial planes at a rate reaching 2–3 cm/hour, masking the true extent of the disease.17
The infection in FG tends to spread along the fascial planes with initial involvement of the superficial (Colles fascia) and deep fascial planes of the genitalia.18 FG preferentially spreads to the overlying perineum and subcutaneous tissue, sparing the deeper muscle layers which are protected by the fascial planes themselves.19 For instance, the Colles fascia attaches to the pubic ramus, as well as the sphincter urethrae and deep transverse perineal muscles, thereby limiting bacterial spread outside of these areas.15 It is important to note, however, that Colles fascia remains continuous with other surrounding fascial planes, facilitating rapid spread towards the abdomen and thorax (via Scarpa’s fascia), as well as the scrotum (via Buck’s and Dartos fascia). Deeper infection extending below the fascial plane involving myonecrosis is not classily thought to be a feature of FG, although it has been described.20
In addition to fascial spread, vascular supply plays an important role in local involvement. The external and internal pudendal arteries arise from the retroperitoneum and supply the testicles, which accounts for the limited testicular involvement seen in FG.2,21 Conversely, the inferior epigastric and circumflex iliac arteries must pierce Camper’s fascia in order to supply the abdominal wall are therefore at an increased risk of thrombosis.19,22 Therefore, involvement of the testicles suggests a retroperitoneal origin or spread of infection, and involvement of the abdominal wall implies involvement of Camper’s fascia.6,23
Primarily an infectious process, FG has several predisposing factors, and theoretically, any condition that impairs host immune response or microcirculation may predispose a patient to FG(Table 1).3,7-14
Etiology
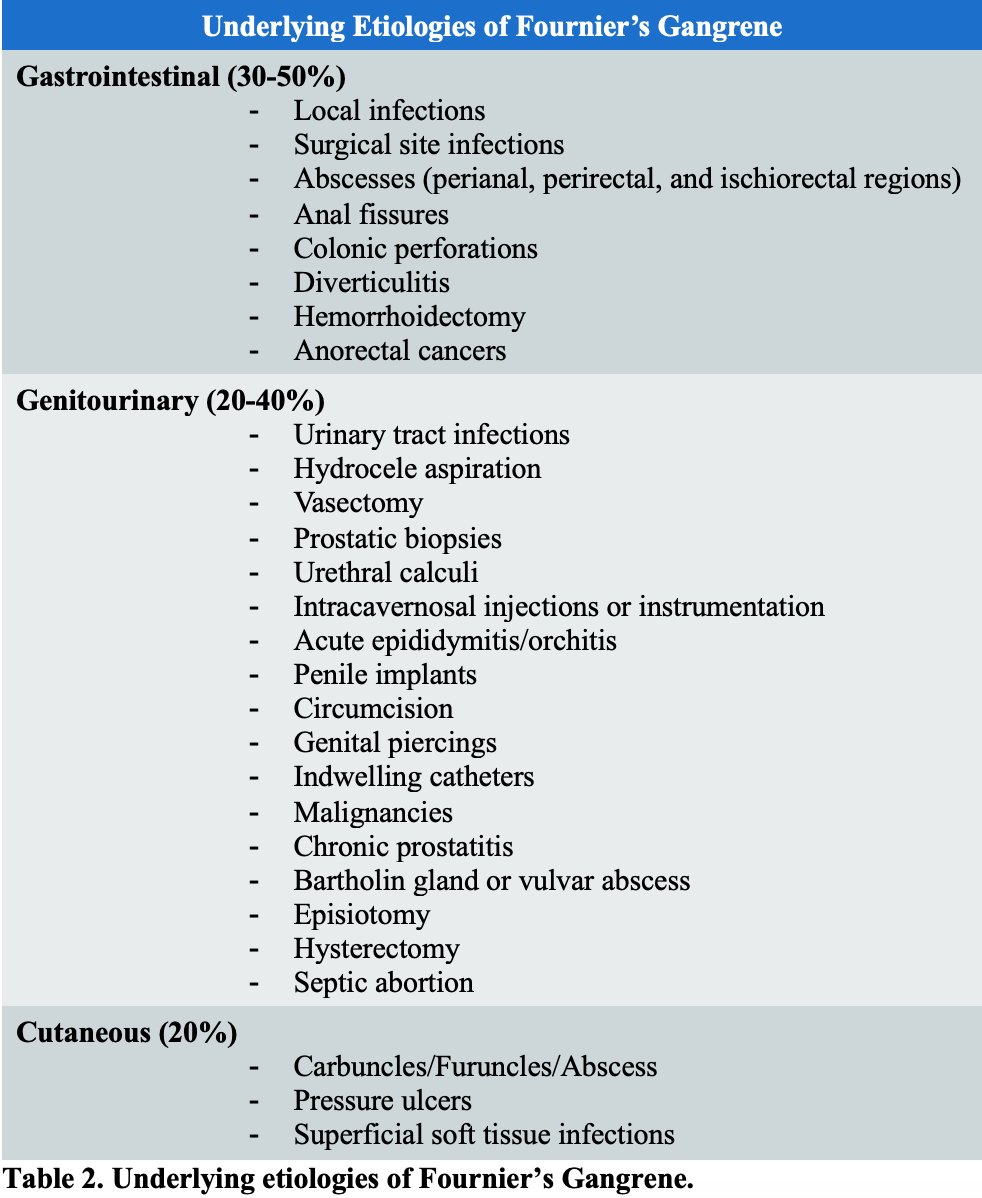
The most common sources of Fournier’s gangrene arise from the gastrointestinal tract (30-50%), genitourinary tract (20-40%), and cutaneous injuries (20%).6 Local trauma is frequently associated with the underlying source of infection.6 Potential sources are provided in Table 2.7,13,15,19,25-29 Special attention must be paid to insect bites, burns, and circumcision as sources of pediatric FG.19,30
Microbiology
Characteristic of many NSTIs, FG severity is derived from the synergism of multiple bacteria that are not highly aggressive when encountered alone, though 80% of cases are polymicrobial.31 Typically, upwards of 4 organisms are cultured from each FG patient.15,32
The organisms most commonly found in FG are species that normally exist below the pelvic diaphragm in the perineum and genitalia.6 These include aerobic microorganisms (e.g. Escherichia coli, Klebsiella pneumoniae, and Staphylococcus aureus), as well as anaerobic microorganisms (e.g. Bacteroides fragilis, Clostridium species).31,33,34 Other species isolated include Vibrio, Streptococcus, Enterococcus, Pseudomonas, Proteus, Klebsiella pneumonia, and Corynebacterium.2 More recently, resistant strains of bacteria, including methicillin-resistant Staphylococcus aureus (MRSA), as well as extended-spectrum beta lactamase resistant E. coli have been reported.35 Likewise, fungal sources such as Candida albicans and Zygomycetes have been reported.36-40 Within the subset of patients with monomicrobial FG, Group A streptococcus is the most commonly isolated organism.29
History and Physical
FG is a clinical diagnosis based on the presence of fluctuance, crepitus, exquisite tenderness, and wounds of the genitalia and perineum.19 Although the diagnosis is straightforward in the classic presentation, failure to examine the perineal area, especially in the older or obtunded patient, can result in misdiagnosis. Furthermore, the early symptoms of FG and NSTIs are not characteristic; hence, FG is often misdiagnosed as cellulitis or abscess in 75% of cases.41,42
The clinical presentation of FG varies widely depending on the extent of infection as well as patient comorbidities. Typically, the infection begins as a localized cellulitis adjacent to the portal of entry, commonly in the perineum or perianal region, with an insidious presentation. Early presenting features are often non-specific and common to other infectious etiologies. In one study of NSTIs, the most common initial chief complaints were swelling (80.8%), pain (79%), and erythema (70.7%).41 Bullae (26%), overlying skin necrosis (24%), and crepitus (20%) were less common upon initial examination, but associated with later stages of necrotizing fasciitis.41
Presence of subcutaneous gas and crepitus are highly specific for clostridial infections.1,43 Fever and tachycardia are present in 40% and 61% of these patients, respectively.12,41,44 The affected area may also appear swollen, dusky, and/or present with a characteristic purulent “dishwater” discharge with associated feculent odor, attributable to the presence of anaerobes.45,46 The presence of hypotension and septic shock is a late and ominous sign, occurring in roughly 21% of patients with NSTIs, but associated with high specificity (93.3%).41,47 This has a strong correlation with mortality, and, along with associated multiorgan failure, is the principal cause of death in patients with NSTIs.19,48
The presenting tenderness, erythema, and swelling may mimic less severe infections including erysipelas and cellulitis. However, a key feature of FG is pain out of proportion to physical examination and should alert the clinician to the possibility of FG. However, this is not always present, as local anesthesia may develop secondary to local nerve ischemia or due to a preexisting neuropathy (e.g. diabetic neuropathy).16 Furthermore, cellulitis and erysipelas often present with well-demarcated areas of inflammation and erythema. In contrast, FG may present with areas of poorly demarcated erythema, as well as blisters and bullae during the later stages of infection.2 While cellulitis and erysipelas may present with symptoms of generalized infection, including malaise and fever, FG can result in severe systemic toxicity with associated multiorgan failure. Furthermore, as FG may spread rapidly along fascial planes, areas of tenderness and erythema may extend as far up as the clavicle.49
The extent of necrosis is an important prognostic factor as some studies have shown that patients with a necrotic area less than 3% of total body surface area rarely die, while patients presenting with involvement of > 5% total body surface area have a worse prognosis.10,23,50,51
Laboratory Investigations
While no single laboratory test has adequate sensitivity and specificity to discern NSTIs from other soft tissue infections, The Laboratory Risk Indicator for Necrotizing Fasciitis (LRINEC) score may suggest the presence of NSTI (Table 3); however, it should not be used to exclude the diagnosis. The original data examined age, gender, serum potassium, platelet count, C-reactive protein(CRP), leukocyte count, hemoglobin, sodium, creatinine, and glucose from 89 consecutive patients with NSTIs compared to 225 control patients.52 Patients were stratified into low-risk (≤5), intermediate-risk (6-7), and high-risk (≥8) categories, corresponding to a probability of <50%, 50%-75%, and >75% for the development of a NSTI, respectively. A score ≥ 6 was found to have 92% positive predictive value and a 96% negative predictive value for presence of a NSTI.52
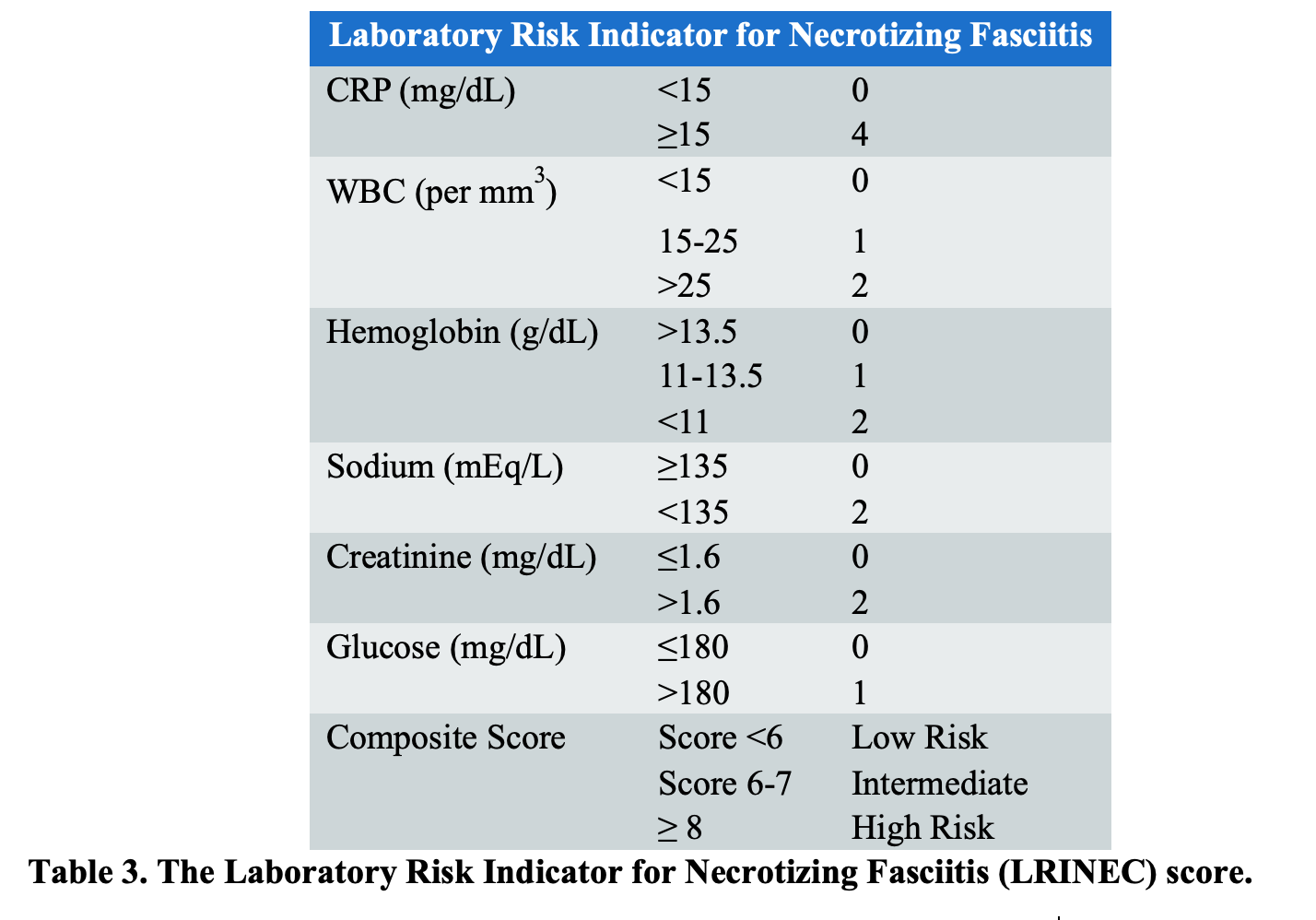
Criticisms of the LRINEC scoring system include its retrospective development and poor sensitivity among ED patients.53 The score was not explicitly designed to exclude NF in patients with a low-risk score, and subsequent studies externally validating the score have thus far failed to replicate the high sensitivity and negative predictive value reported in the initial paper. The LRINEC score, applied in isolation to ED patients, would miss over 20% of cases of NSTIs, with an associated sensitivity between 68% and 80%.47,53-55 There have also been cases of NSTI with LRINEC scores of 0.56 As the LRINEC score has limited sensitivity, it should not be used as the sole determinant of clinical decision-making for the diagnosis of FG.
Imaging
The diagnosis of FG is primarily clinical, and in many cases, imaging is not necessary, nor is it desirable if it leads to a delay in surgical management.19 However, imaging is a useful adjunct in those cases in which the presentation is atypical, or when there is concern regarding the true extent of the disease.
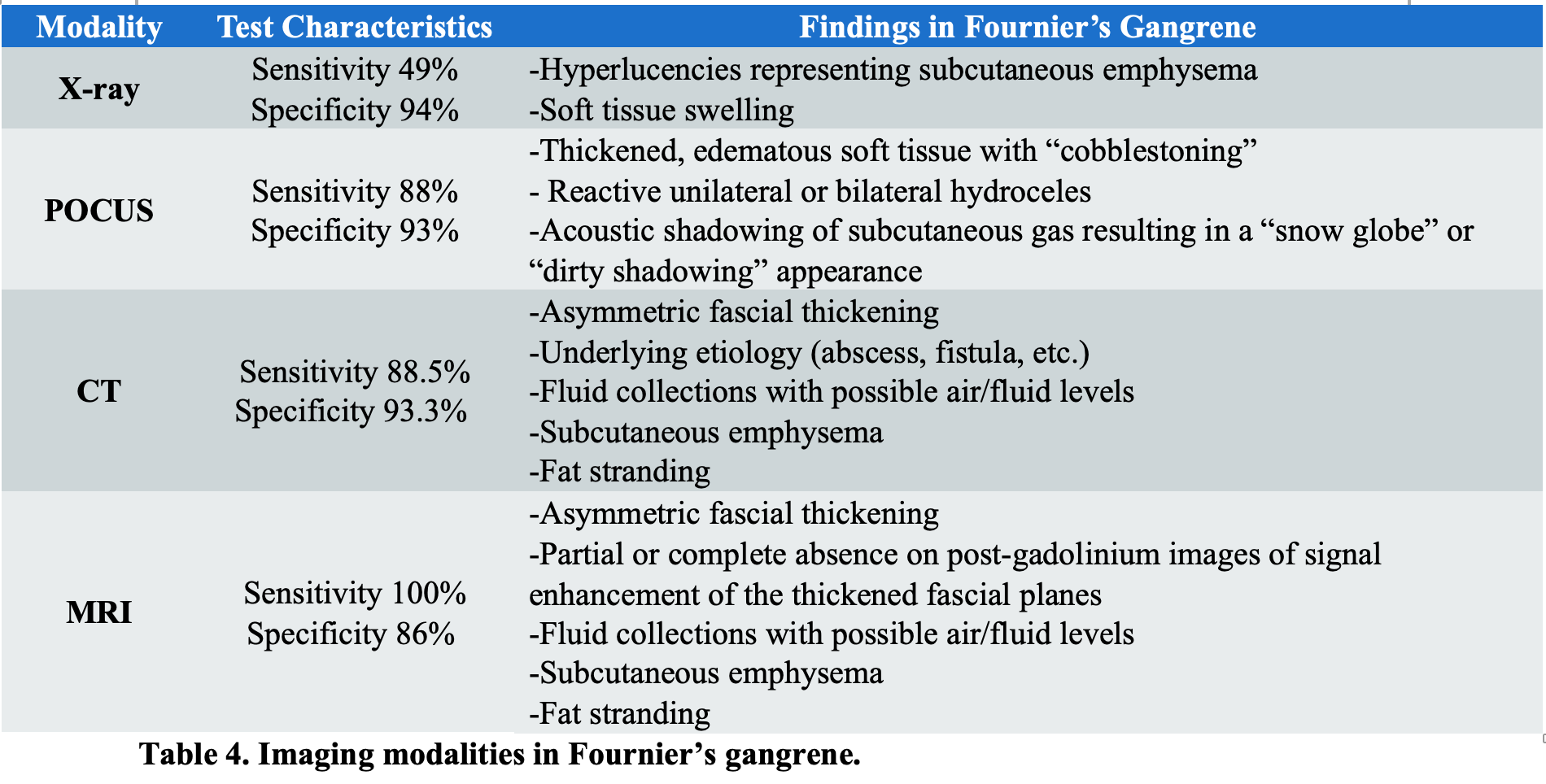
Conventional radiography can be used to detect the presence of soft tissue swelling as well as gas in the perineal fascial planes before crepitus is noted on exam (Figure 2).19 Subcutaneous emphysema may extend from the scrotum and perineum to the inguinal regions, anterior abdominal wall, and thighs. Evidence of gas formation is present in nearly half of all patients with FG and is highly specific (94%). However, the absence of gas formation on imaging should not exclude the diagnosis due to poor sensitivity (49%).16,47,57

Point-of-care ultrasound (POCUS) allows for the evaluation of soft tissue inflammation, collections/abscesses, as well as identification of subcutaneous gas.58,59 Characteristic findings include thickened perineal tissue caused by inflammation and edema, as well as a “cobblestone” appearance throughout the subcutaneous tissue. Acoustic shadowing of subcutaneous gas secondary to bacteria may result in a “snow globe” or “dirty shadowing” appearance caused by hyperechoic foci demonstrating reverberation artifacts (Figure 3).60 While POCUS has been shown to be highly specific for NSTIs (up to 93%), it is insufficiently sensitive (approximately 88%) to exclude a diagnosis with such a high morbidity and mortality.61,62

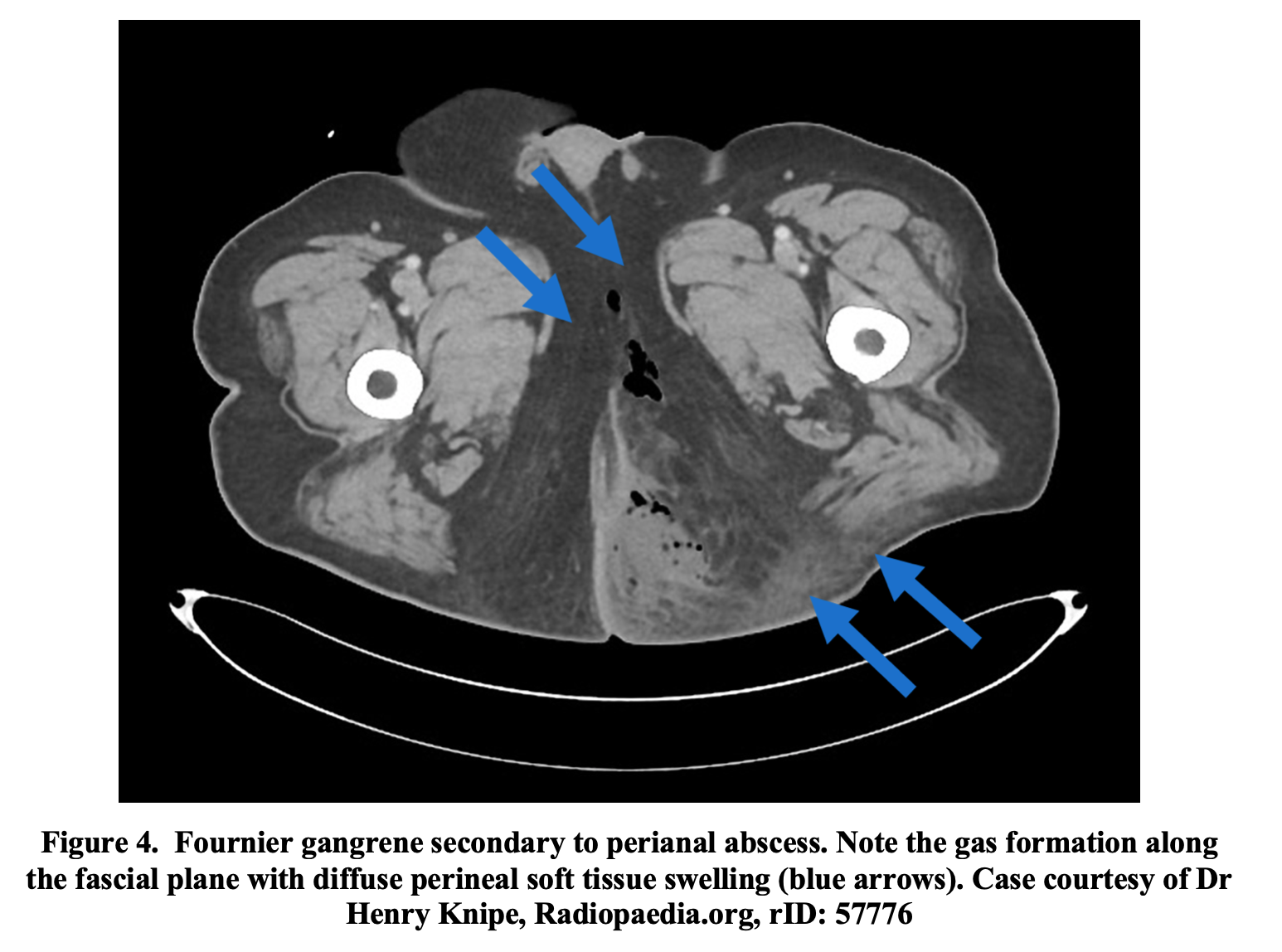
CT imaging plays an important role in the diagnosis of FG and to evaluate the extent of the disease. Intravenous contrast can further characterize the soft tissue and should be used if possible.64,65 Characteristic findings include asymmetric fascial thickening, fluid collections, abscess formation, fat stranding around involved structures, and evidence of subcutaneous emphysema (Figure 4).60,66,67 CT may uncover the underlying etiology of FG, such as a perineal abscess, fistula formation, or any infectious process in the intra-abdominal or retroperitoneal spaces.60,66 It assists in differentiating FG from less severe infections and allows evaluation of both the superficial and deep fascial planes.19 CT has a sensitivity of 88.5% in addition to high specificity (93.3%) for the diagnosis of NSTIs.47
MRI with gadolinium contrast is an excellent imaging modality to characterize soft tissues.68 However, in the ED setting, MRI is of limited value due to its high cost, extended time of examination, and the fact that it requires a clinically stable patient.2 Although it has been shown to have a high sensitivity (100%) and specificity (86%) to diagnose NSTIs, MRI has a limited role for evaluation of FG in the ED (Table 4).2,69
Management
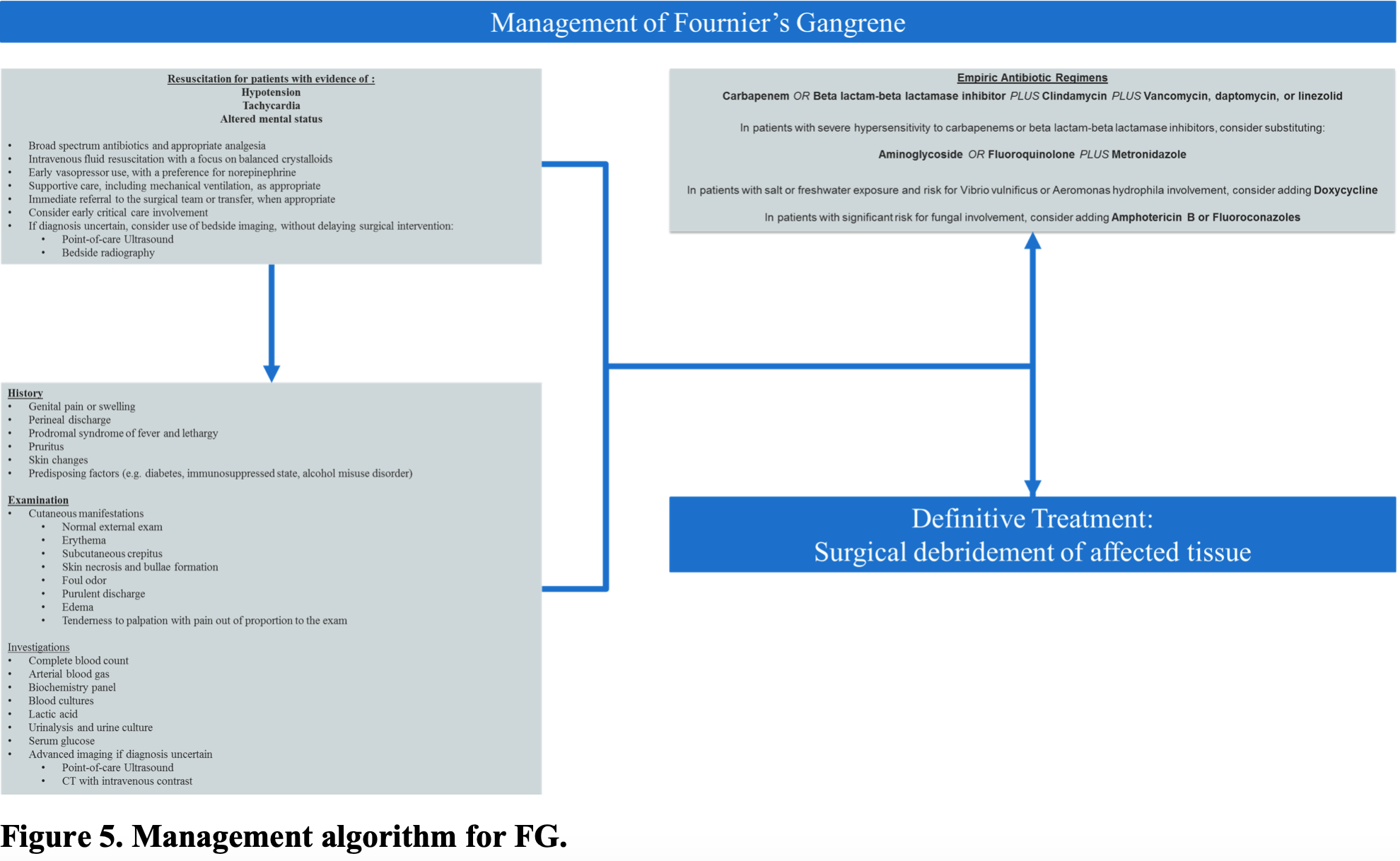
The cornerstones of treatment of FG include emergent surgical debridement of all necrotic tissue, broad-spectrum antibiotics, and hemodynamic resuscitation with intravenous fluids as well as vasoactive medications as needed.6,18,19 As the rate of fascial necrosis has been noted as high as 2–3 cm per hour, FG is considered a surgical emergency necessitating early involvement of the appropriate surgical teams, which decreases mortality.17,70,71 As up to 21% of patients present with symptoms of hypotension and septic shock, hemodynamic resuscitation and patient optimization prior to surgical intervention are important aspects of management.41,47
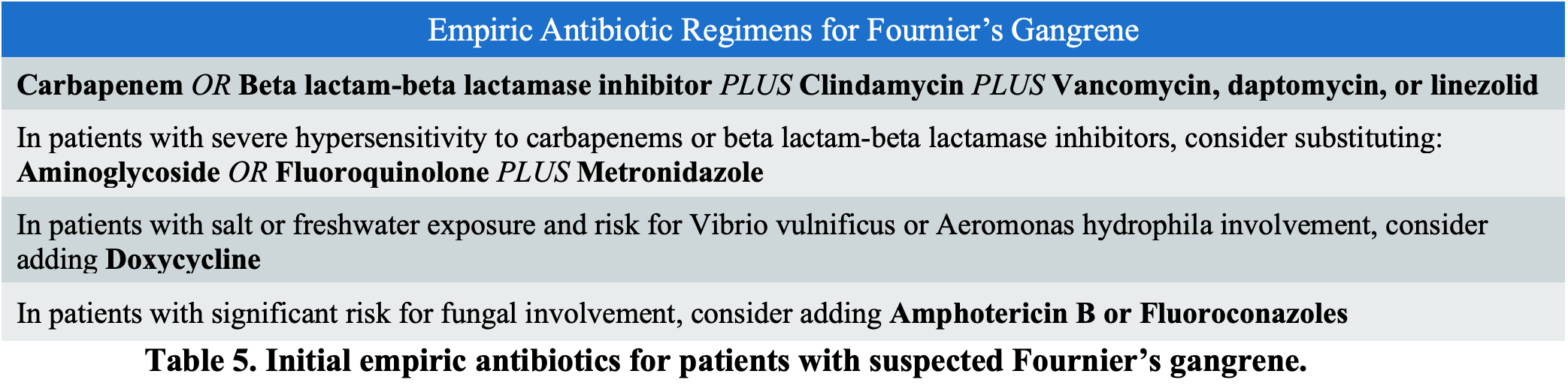
Broad-spectrum parenteral antibiotic therapy is initiated empirically upon diagnosis of FG and then subsequently tailored based on culture results.19 Any initial antibiotic regimen must have a broad range of activity against commonly implicated organisms, most notably staphylococcal and streptococcal species, as well as coliforms, gram-negative bacteria, Clostridium, Bacteroides, and Pseudomonas (Table 5).12 Empiric antibiotics must cover for MRSA, typically with linezolid or vancomycin, which is combined with a carbapenem or beta-lactam-beta-lactamase inhibitor.72 Clindamycin should be added, as it can suppress toxin production and modulate cytokine production, as well as decrease mortality from NSTIs.12,73 In those patients with severe penicillin hypersensitivity, clindamycin or metronidazole combined with an aminoglycoside or fluoroquinolone should be administered.72 Additionally, many have suggested adding penicillin for treatment of streptococci and, in particular, when Clostridium species are suspected.72 Doxycycline should be considered for those patients with significant risk for Vibrio vulnificus and Aeromonas hydrophila involvement, including exposure to marine exposure, and exposure to seafood.72 Special consideration should be given to initiating early antifungal therapy with amphotericin B or fluoroconazoles in those patients with a history of fungal infections and immunocompromised patients, as fungal sources are now an emerging cause of NSTIs.74,75
Hemodynamic resuscitation and optimization of the patient’s comorbidities play an integral role in ED management. Patients may present hypotensive or in septic shock characterized by hypoperfusion, which can result in organ dysfunction. Aggressive fluid resuscitation and hemodynamic support are often required, as evidence of end-organ dysfunction is associated with increased mortality.76 As many patients with FG have underlying comorbidities that may exacerbate underlying FG, most commonly diabetes mellitus, it is important to treat these underlying comorbidities. While few data exist concerning optimizing patient comorbidities in those with FG, a treatment strategy may be extrapolated from current critical care literature. Insulin therapy for glycemic control for a target blood glucose level of 140-200 mg/dl has been suggested in critically ill patients, which is reasonable for patients presenting with hyperglycemia.77 These patients may also present with an episode of diabetic ketoacidosis (DKA) secondary to FG and should be managed in accordance with current guidelines.78 Up to 50% of patients with FG have an underlying alcohol use disorder and may be suffering from concomitant alcohol withdrawal or delirium tremens. These patients should be treated with adequate supportive care, as well as benzodiazepines administered in a symptom-triggered fashion, guided by the Clinical Institute Withdrawal Assessment of Alcohol scale, revised (CIWA-Ar).79
Prompt surgical consultation is recommended for all patients in whom FG is suspected and should not be delayed by laboratory or imaging investigations (Figure 5).19,72 Depending on local practice patterns, as well as individual patient characteristics, this may involve physicians from the general surgery, urology, or obstetrics and gynecology services, or a combination. The most important variable affecting mortality in patients with NSTIs is time to admission and debridement.70 One study suggests that survival decreases from 93.2% to 75.2% with a delay in debridement from 24 to 48 hours.41 Similarly, in another study, the average time from admission to operation was 90 hours in non-survivors versus 25 hours in survivors, making early surgical intervention imperative.80
Hyperbaric Oxygen Therapy (HBOT)is used as an adjunctive therapy for the optimization of infected tissue oxygenation and for its bactericidal and bacteriostatic effects, especially in the post-surgical period.81 However, the lack of randomized controlled studies limits the use of HBOT to patients unresponsive to conventional surgical and intensive care management.82,83 As such, HBOT is not routinely recommended prior to surgical debridement, and consultation with a hyperbarics specialist is typically not a consideration in the ED.
Disposition
Early surgical consultation and involvement of the critical care team facilitates timely management and coordinated handoff to ensure the best patient care possible, as prolonged boarding in the ED has been associated with increased risk of mortality.42 Level of care is dependent on the patient’s underlying pathophysiology, hemodynamic status, need for invasive monitoring, and underlying comorbidities, but typically these patients will require admission to the intensive care unit. Additional considerations for under-resourced hospitals include transfer to a higher level of care, as up to 66% of hospitals in the United States do not encounter cases of FG, and adequate surgical capabilities may not be present.3 However, the decision to transfer should be made in consultation with the receiving facility’s surgical team, as well as the transferring facility’s surgeon, as interhospital transfer has been associated with increased mortality, although this remains controversial.84,85
Take Home Points
- Fournier’s gangrene is most likely to present in an obese male patient between the ages of 50 and 79 years of age, with one or more risk factors –immunosuppression, alcohol use disorder, or diabetes.
- Fascial anatomy plays an important role in the pathophysiology of Fournier’s gangrene. The Colles fascia remains continuous with other surrounding fascial planes, facilitating rapid spread towards the abdomen and thorax (via Scarpa’s fascia), as well as the scrotum (via Buck’s and Dartos fascia).
- The most common sources of Fournier’s gangrene arise from the gastrointestinal tract (30-50%), genitourinary tract (20-40%), and cutaneous injuries (20%).
- Up to 80% of FG cases are polymicrobial, with an average of four organisms per patient.
- FG is often misdiagnosed as cellulitis or abscess in 75% of cases, and any crepitus, pain out of proportion, or ecchymosis should clue you in to possible FG.
- The Laboratory Risk Indicator for Necrotizing Fasciitis (LRINEC) score may suggest the presence of NSTI, however, it should not be used to exclude the diagnosis of FG.
- CT has a sensitivity of 88.5% and specificity of 93.3% for the diagnosis of Fournier’s gangrene. MRI is more sensitive but may not be available and takes longer to obtain.
- The cornerstones of treatment of FG include emergent surgical debridement of all necrotic tissue, broad-spectrum antibiotics, and hemodynamic resuscitation with intravenous fluids as well as vasoactive medications as needed.
FOAMed Resources:
- emDOCs- Necrotizing Fasciitis
- emDOCs- EM@3AM: Necrotizing Fasciitis
- emDOCs- Necrotizing Fasciitis Pearls and Pitfalls
- EM Cases- Best Case Ever 69 Necrotizing Fasciitis
- Life in the Fast Lane- Necrotising Fasciitis
- Taming the SRU- Necrotizing Fasciitis and the Spectrum of Soft Tissue Infections
- MDCalc- LRINEC Score
References/Further Reading:
- Hakkarainen TW, Kopari NM, Pham TN, Evans HL. Necrotizing soft tissue infections: review and current concepts in treatment, systems of care, and outcomes. Curr Probl Surg. 2014;51(8):344-362.
- Voelzke BB, Hagedorn JC. Presentation and Diagnosis of Fournier Gangrene. Urology.2018;114:8-13.
- Sorensen MD, Krieger JN, Rivara FP, et al. Fournier’s Gangrene: population based epidemiology and outcomes. J Urol. 2009;181(5):2120-2126.
- Ugwumba FO, Nnabugwu, II, Ozoemena OF. Fournier’s gangrene — analysis of management and outcome in south-eastern Nigeria. S Afr J Surg. 2012;50(1):16-19.
- Sorensen MD, Krieger JN. Fournier’s Gangrene: Epidemiology and Outcomes in the General US Population. Urol Int. 2016;97(3):249-259.
- Eke N. Fournier’s gangrene: a review of 1726 cases. Br J Surg. 2000;87(6):718-728.
- Aridogan IA, Izol V, Abat D, Karsli O, Bayazit Y, Satar N. Epidemiological characteristics of Fournier’s gangrene: a report of 71 patients. Urol Int. 2012;89(4):457-461.
- Martinschek A, Evers B, Lampl L, Gerngross H, Schmidt R, Sparwasser C. Prognostic aspects, survival rate, and predisposing risk factors in patients with Fournier’s gangrene and necrotizing soft tissue infections: evaluation of clinical outcome of 55 patients. Urol Int. 2012;89(2):173-179.
- Morpurgo E, Galandiuk S. Fournier’s gangrene. Surg Clin North Am. 2002;82(6):1213-1224.
- Clayton MD, Fowler JE, Jr., Sharifi R, Pearl RK. Causes, presentation and survival of fifty-seven patients with necrotizing fasciitis of the male genitalia. Surg Gynecol Obstet. 1990;170(1):49-55.
- Ayan F, Sunamak O, Paksoy SM, et al. Fournier’s gangrene: a retrospective clinical study on forty-one patients. ANZ J Surg. 2005;75(12):1055-1058.
- Mallikarjuna MN, Vijayakumar A, Patil VS, Shivswamy BS. Fournier’s Gangrene: Current Practices. ISRN Surg. 2012;2012:942437.
- Backhaus M, Citak M, Tilkorn DJ, Meindl R, Schildhauer TA, Fehmer T. Pressure sores significantly increase the risk of developing a Fournier’s gangrene in patients with spinal cord injury. Spinal Cord. 2011;49(11):1143-1146.
- Malik AM, Sheikh S, Pathan R, Khan A, Sheikh U. The spectrum of presentation and management of Fournier’s gangrene–an experience of 73 cases. J Pak Med Assoc. 2010;60(8):617-619.
- Thwaini A, Khan A, Malik A, et al. Fournier’s gangrene and its emergency management. Postgrad Med J. 2006;82(970):516-519.
- Misiakos EP, Bagias G, Patapis P, Sotiropoulos D, Kanavidis P, Machairas A. Current concepts in the management of necrotizing fasciitis. Front Surg. 2014;1:36.
- Safioleas M, Stamatakos M, Mouzopoulos G, Diab A, Kontzoglou K, Papachristodoulou A. Fournier’s gangrene: exists and it is still lethal. Int Urol Nephrol. 2006;38(3-4):653-657.
- Corman JM, Moody JA, Aronson WJ. Fournier’s gangrene in a modern surgical setting: improved survival with aggressive management. BJU Int. 1999;84(1):85-88.
- Chennamsetty A, Khourdaji I, Burks F, Killinger KA. Contemporary diagnosis and management of Fournier’s gangrene. Ther Adv Urol. 2015;7(4):203-215.
- Rye BA, Seidelin C, Dueholm S. Perineal progressive myonecrosis following Thiersch’s operation for rectal prolapse. Ann Chir Gynaecol. 1987;76(2):136-137.
- Gupta A, Dalela D, Sankhwar SN, et al. Bilateral testicular gangrene: does it occur in Fournier’s gangrene? Int Urol Nephrol. 2007;39(3):913-915.
- Katib A, Al-Adawi M, Dakkak B, Bakhsh A. A three-year review of the management of Fournier’s gangrene presented in a single Saudi Arabian institute. Cent European J Urol. 2013;66(3):331-334.
- Chawla SN, Gallop C, Mydlo JH. Fournier’s gangrene: an analysis of repeated surgical debridement. Eur Urol. 2003;43(5):572-575.
- Meki C. Fournier’s Gangrene: outcome analysis at three tertiary hospitals in Harare Zimbabwe: Surgery, University of Zimbabwe; 2016.
- Ash L, Hale J. CT findings of perforated rectal carcinoma presenting as Fournier’s gangrene in the emergency department.Emerg Radiol. 2005;11(5):295-297.
- Chan CC, Williams M. Fournier gangrene as a manifestation of undiagnosed metastatic perforated colorectal cancer. Int Surg. 2013;98(1):43-48.
- Ulug M, Gedik E, Girgin S, Celen MK, Ayaz C. The evaluation of microbiology and Fournier’s gangrene severity index in 27 patients. Int J Infect Dis. 2009;13(6):e424-430.
- Wroblewska M, Kuzaka B, Borkowski T, Kuzaka P, Kawecki D, Radziszewski P. Fournier’s gangrene–current concepts. Pol J Microbiol. 2014;63(3):267-273.
- Ekelius L, Bjorkman H, Kalin M, Fohlman J. Fournier’s gangrene after genital piercing. Scand J Infect Dis. 2004;36(8):610-612.
- Amendola MA, Casillas J, Joseph R, Antun R, Galindez O. Fournier’s gangrene: CT findings. Abdom Imaging. 1994;19(5):471-474.
- Tang LM, Su YJ, Lai YC. The evaluation of microbiology and prognosis of fournier’s gangrene in past five years. Springerplus. 2015;4:14.
- Addison WA, Livengood CH, 3rd, Hill GB, Sutton GP, Fortier KJ. Necrotizing fasciitis of vulvar origin in diabetic patients. Obstet Gynecol. 1984;63(4):473-479.
- Paty R, Smith AD. Gangrene and Fournier’s gangrene. Urol Clin North Am. 1992;19(1):149-162.
- Yanar H, Taviloglu K, Ertekin C, et al. Fournier’s gangrene: risk factors and strategies for management. World J Surg. 2006;30(9):1750-1754.
- Lin WT, Chao CM, Lin HL, Hung MC, Lai CC. Emergence of antibiotic-resistant bacteria in patients with Fournier gangrene. Surg Infect (Larchmt). 2015;16(2):165-168.
- Crowell W, Roberts R, Tarry S. Fungal Fourniers Gangrene in an Immunocompromised Patient. Urol Case Rep. 2016;4:1-3.
- Johnin K, Nakatoh M, Kadowaki T, Kushima M, Koizumi S, Okada Y. Fournier’s gangrene caused by Candida species as the primary organism. Urology. 2000;56(1):153.
- Temiz M, Cetin M, Aslan A. [Fournier’s gangrene caused by Candida albicans]. Mikrobiyol Bul. 2008;42(4):707-711.
- Jensen P, Zachariae C, Gronhoj Larsen F. Necrotizing soft tissue infection of the glans penis due to atypical Candida species complicated with Fournier’s gangrene. Acta Derm Venereol. 2010;90(4):431-432.
- Tleyjeh IM, Routh J, Qutub MO, Lischer G, Liang KV, Baddour LM. Lactobacillus gasseri causing Fournier’s gangrene. Scand J Infect Dis. 2004;36(6-7):501-503.
- Goh T, Goh LG, Ang CH, Wong CH. Early diagnosis of necrotizing fasciitis. Br J Surg. 2014;101(1):e119-125.
- Wong CH, Chang HC, Pasupathy S, Khin LW, Tan JL, Low CO. Necrotizing fasciitis: clinical presentation, microbiology, and determinants of mortality. J Bone Joint Surg Am. 2003;85-A(8):1454-1460.
- Sudarsky LA, Laschinger JC, Coppa GF, Spencer FC. Improved results from a standardized approach in treating patients with necrotizing fasciitis. Ann Surg. 1987;206(5):661-665.
- Ersay A, Yilmaz G, Akgun Y, Celik Y. Factors affecting mortality of Fournier’s gangrene: review of 70 patients. ANZ J Surg. 2007;77(1-2):43-48.
- Rodriguez Alonso A, Perez Garcia MD, Nunez Lopez A, et al. [Fournier’s gangrene: anatomo-clinical features in adults and children. Therapy update]. Actas Urol Esp. 2000;24(4):294-306.
- Ferreira PC, Reis JC, Amarante JM, et al. Fournier’s gangrene: a review of 43 reconstructive cases. Plast Reconstr Surg. 2007;119(1):175-184.
- Fernando SM, Tran A, Cheng W, et al. Necrotizing Soft Tissue Infection: Diagnostic Accuracy of Physical Examination, Imaging, and LRINEC Score: A Systematic Review and Meta-Analysis. Ann Surg. 2019;269(1):58-65.
- Sutherland ME, Meyer AA. Necrotizing soft-tissue infections. Surg Clin North Am. 1994;74(3):591-607.
- Saijo S, Kuramoto Y, Yoshinari M, Tagami H. Extremely extended Fournier’s gangrene. Dermatologica.1990;181(3):228-232.
- Dahm P, Roland FH, Vaslef SN, et al. Outcome analysis in patients with primary necrotizing fasciitis of the male genitalia. Urology. 2000;56(1):31-35; discussion 35-36.
- Horta R, Cerqueira M, Marques M, Ferreira P, Reis J, Amarante J. [Fournier’s gangrene: from urological emergency to plastic surgery]. Actas Urol Esp. 2009;33(8):925-929.
- Wong CH, Khin LW, Heng KS, Tan KC, Low CO. The LRINEC (Laboratory Risk Indicator for Necrotizing Fasciitis) score: a tool for distinguishing necrotizing fasciitis from other soft tissue infections. Crit Care Med. 2004;32(7):1535-1541.
- Burner E, Henderson SO, Burke G, Nakashioya J, Hoffman JR. Inadequate Sensitivity of Laboratory Risk Indicator to Rule Out Necrotizing Fasciitis in the Emergency Department. West J Emerg Med. 2016;17(3):333-336.
- Hodgins N, Damkat-Thomas L, Shamsian N, Yew P, Lewis H, Khan K. Analysis of the increasing prevalence of necrotising fasciitis referrals to a regional plastic surgery unit: a retrospective case series. J Plast Reconstr Aesthet Surg. 2015;68(3):304-311.
- Swain RA, Hatcher JC, Azadian BS, Soni N, De Souza B. A five-year review of necrotising fasciitis in a tertiary referral unit. Ann R Coll Surg Engl. 2013;95(1):57-60.
- Wilson MP, Schneir AB. A case of necrotizing fasciitis with a LRINEC score of zero: clinical suspicion should trump scoring systems. J Emerg Med. 2013;44(5):928-931.
- Anaya DA, Dellinger EP. Necrotizing soft-tissue infection: diagnosis and management. Clin Infect Dis. 2007;44(5):705-710.
- Kube E, Stawicki SP, Bahner DP. Ultrasound in the diagnosis of Fournier’s gangrene. Int J Crit Illn Inj Sci. 2012;2(2):104-106.
- Kane CJ, Nash P, McAninch JW. Ultrasonographic appearance of necrotizing gangrene: aid in early diagnosis. Urology. 1996;48(1):142-144.
- Levenson RB, Singh AK, Novelline RA. Fournier gangrene: role of imaging. Radiographics.2008;28(2):519-528.
- Yen ZS, Wang HP, Ma HM, Chen SC, Chen WJ. Ultrasonographic screening of clinically-suspected necrotizing fasciitis. Acad Emerg Med. 2002;9(12):1448-1451.
- Castleberg E, Jenson N, Dinh VA. Diagnosis of necrotizing faciitis with bedside ultrasound: the STAFF Exam. West J Emerg Med. 2014;15(1):111-113.
- Guttman J. Fournier Gangrene on Bedside Ultrasound. In. The EM Pulse.Vol 20192016.
- Martinez M, Peponis T, Hage A, et al. The Role of Computed Tomography in the Diagnosis of Necrotizing Soft Tissue Infections. World J Surg. 2018;42(1):82-87.
- Zacharias N, Velmahos GC, Salama A, et al. Diagnosis of necrotizing soft tissue infections by computed tomography. Arch Surg. 2010;145(5):452-455.
- Rajan DK, Scharer KA. Radiology of Fournier’s gangrene. AJR Am J Roentgenol.1998;170(1):163-168.
- Piedra T, Ruiz E, Gonzalez FJ, Arnaiz J, Lastra P, Lopez-Rasines G. Fournier’s gangrene: a radiologic emergency. Abdom Imaging. 2006;31(4):500-502.
- Kim KT, Kim YJ, Won Lee J, et al. Can necrotizing infectious fasciitis be differentiated from nonnecrotizing infectious fasciitis with MR imaging? Radiology.2011;259(3):816-824.
- Malghem J, Lecouvet FE, Omoumi P, Maldague BE, Vande Berg BC. Necrotizing fasciitis: contribution and limitations of diagnostic imaging. Joint Bone Spine. 2013;80(2):146-154.
- Carter PS, Banwell PE. Necrotising fasciitis: a new management algorithm based on clinical classification. Int Wound J. 2004;1(3):189-198.
- Oymaci E, Coskun A, Yakan S, Erkan N, Ucar AD, Yildirim M. Evaluation of factors affecting mortality in Fournier’s Gangrene: Retrospective clinical study of sixteen cases. Ulus Cerrahi Derg. 2014;30(2):85-89.
- Stevens DL, Bisno AL, Chambers HF, et al. Practice guidelines for the diagnosis and management of skin and soft tissue infections: 2014 update by the Infectious Diseases Society of America. Clin Infect Dis. 2014;59(2):e10-52.
- Morgan MS. Diagnosis and management of necrotising fasciitis: a multiparametric approach. J Hosp Infect. 2010;75(4):249-257.
- Chander J, Stchigel AM, Alastruey-Izquierdo A, et al. Fungal necrotizing fasciitis, an emerging infectious disease caused by Apophysomyces (Mucorales). Rev Iberoam Micol. 2015;32(2):93-98.
- Prasanna Kumar S, Ravikumar A, Somu L. Fungal necrotizing fasciitis of the head and neck in 3 patients with uncontrolled diabetes. Ear Nose Throat J. 2014;93(3):E18-21.
- Benjelloun el B, Souiki T, Yakla N, et al. Fournier’s gangrene: our experience with 50 patients and analysis of factors affecting mortality. World J Emerg Surg. 2013;8(1):13.
- Qaseem A, Humphrey LL, Chou R, Snow V, Shekelle P, Clinical Guidelines Committee of the American College of P. Use of intensive insulin therapy for the management of glycemic control in hospitalized patients: a clinical practice guideline from the American College of Physicians. Ann Intern Med. 2011;154(4):260-267.
- Gosmanov AR, Gosmanova EO, Dillard-Cannon E. Management of adult diabetic ketoacidosis. Diabetes Metab Syndr Obes. 2014;7:255-264.
- Sarff M, Gold JA. Alcohol withdrawal syndromes in the intensive care unit. Crit Care Med. 2010;38(9 Suppl):S494-501.
- McHenry CR, Piotrowski JJ, Petrinic D, Malangoni MA. Determinants of mortality for necrotizing soft-tissue infections.Ann Surg. 1995;221(5):558-563; discussion 563-555.
- Rosa I, Guerreiro F. Hyperbaric Oxygen Therapy for the Treatment of Fournier’s Gangrene: A Review of 34 Cases. Acta Med Port. 2015;28(5):619-623.
- Singh A, Ahmed K, Aydin A, Khan MS, Dasgupta P. Fournier’s gangrene. A clinical review. Arch Ital Urol Androl. 2016;88(3):157-164.
- Mindrup SR, Kealey GP, Fallon B. Hyperbaric oxygen for the treatment of fournier’s gangrene. J Urol. 2005;173(6):1975-1977.
- Holena DN, Mills AM, Carr BG, et al. Transfer status: a risk factor for mortality in patients with necrotizing fasciitis. Surgery. 2011;150(3):363-370.
- Ingraham AM, Jung HS, Liepert AE, Warner-Hillard C, Greenberg CC, Scarborough JE. Effect of transfer status on outcomes for necrotizing soft tissue infections. J Surg Res. 2017;220:372-378.





1 thought on “Fournier’s Gangrene: ED presentations, evaluation, and management”
Pingback: Jan ’24 Asynchronous – Lakeland Health EM Blog