Featured on the LITFL Review #163 – Thanks to Mat Goebel and the LITFL Review group for the shout out!
Authors: Sandra Isnasious (MS-IV at UCLA David Geffen School of Medicine) and Manpreet Singh, MD (EM Chief Resident at Harbor-UCLA Medical Center – @MPrizzleER) // Editor: Alex Koyfman, MD (@EMHighAK, EM Attending Physician, UTSW / Parkland Memorial Hospital)
Introduction
Hypotension is typically defined as SBP < 90 mmHg, MAP < 60 mmHg, a decrease greater than 40 mmHg or 30% from patient’s baseline MAP, or a combination of any of the aforementioned. However, no clear definition of hypotension truly exists because it must be placed in context of the individual patient. What is considered a “normal” blood pressure may be dangerously low in a chronically hypertensive patient.
A good approach when dealing with hypotension at the bedside includes using the following systematic four step evaluation, which relies heavily on our bedside physical examination and ultrasound skills to evaluate each individual component:
- Heart Rate
- Volume Status
- Cardiac Performance
- Systemic Vascular Resistance
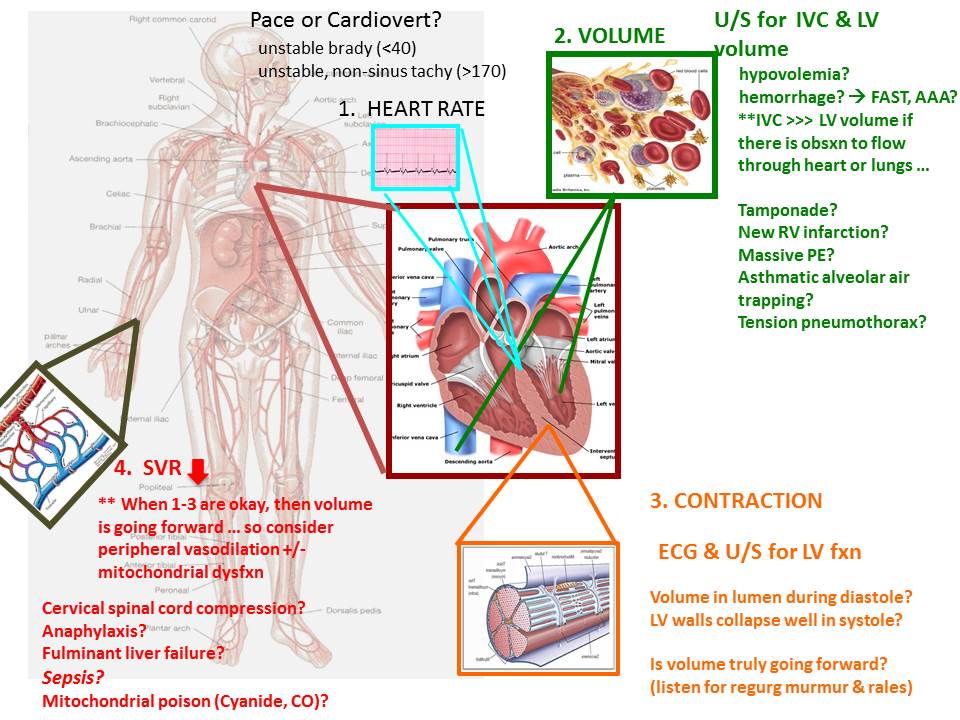
In general, hypotension results from a dysfunction in one or more of these components, so systematically going through these components and addressing them one at a time is a great way to understand the underlying disease pathophysiology our hypotensive ED patient faces.
- Heart Rate (HR):
- Approach: Look at the HR on the monitor.
- Increased or decreased HR can lead to hypotension.
- Tachycardia: In general, unstable, non-sinus HR > 170 (threshold varies with compliance of LV and age of pt) can result in hypotension.
- Physiology:
- ↑ HR -> ↓ stroke volume because there is less time for diastolic filling -> ↓ Cardiac Output (HR x SV) -> hypotension
- Additionally, since less time is spent in diastole, the ventricular myocardium has inadequate relaxation time to allow flow through intramyocardial perforating coronary branches. This leads to ischemia of the LV subendocardium. Ischemia can progress from the subendocardium to more superficial layers of the LV myocardium and result in poor contractile function -> hypotension
- Also, diffuse ischemia can produce heterogeneous myocyte repolarization patterns -> re-entrant arrhythmia or fibrillation.
- The key is to differentiate between tachycardia as a response to hypotension or tachycardia as the cause of hypotension.
- Typically HR > 170 starts to affect diastolic filling and can result in hypotension -> suspect tachycardia as the cause of hypotension.
- Typically HR < 170 does not affect diastolic filling -> suspect tachycardia as the response to hypotension.
- Of note: AFib w/ RVR may result in hypotension at lower HR thresholds because short diastolic filling is compounded by loss of atrial contraction, and hence LV filling is solely passive. In this setting, non-compliant LVs may fail to fill at HRs as low as 140.
- Physiology:
- Bradycardia: In general, unstable HR < 50 can result in hypotension.
- Physiology: ↓ Heart Rate -> ↓ Cardiac Output -> Hypotension
- Differential: Know your tachyarrhythmias and bradyarrhythmias, but in general treat appropriately -> cardiovert or pace the patient.
- Volume Status:
- Assess this after you’ve determined that the HR is a result of hypotension, not the cause (since rapid heart rates impair diastolic filling and will enlarge the IVC as volume remains peripherally).
- Physiology: ↓ Volume Status -> ↓ Stroke Volume -> ↓ Cardiac Output -> Hypotension
- Approach: Do a quick bedside physical examination, then grab your ultrasound probe to assess the inferior vena cava (IVC) and left ventricle (LV) volume.
- Physical examination:
- Look at the patient’s face.
- Dry mucous membranes?
- Sunken eyes?
- Feel the extremities.
- Abnormal skin turgor (ie tenting when pinched)?
- Poor capillary refill (ie > 2 seconds)?
- Weak pulse?
- Cool extremities?
- Look at the patient’s face.
- IVC/LV Ultrasound
- Flat/collapsed IVC (anteroposterior diameter of the IVC < 2 cm in size with > 50% collapse with respiratory variation) with hyperdynamic LV.
- Differential: Hypovolemia vs. Hemorrhage.
- Is this due to hypovolemia from dehydration?
- Hemorrhage from a ruptured AAA/ectopic/GI Bleed?
- FAST the patient
- Abdominal aorta > 3 cm indicates AAA
- Abdominal or pelvic free fluid
- Serial bedside HGB testing
- FAST the patient
- Treatment: Fluid/blood resuscitation
- Differential: Hypovolemia vs. Hemorrhage.
- Plethoric / plump, non-compressible IVC, which is significantly greater than LV volume.
- Ask yourself if there is an obstruction to the flow through the heart or the lungs? -> Obstructive shock
- Differential: Cardiac tamponade vs. RV infarction vs. severe pulm HTN/massive pulmonary embolism (PE) vs. asthmatic alveolar air trapping vs. tension pneumothorax (PTX)
- Ultrasound findings to look for:
- Anechoic fluid surrounding heart with diastolic collapse -> cardiac tamponade
- RV strain (RV/LV ratio > 0.9, “D sign”) -> Pulmonary HTN of some cause (massive PE? Alveolar air trapping?)
- Lack of lung sliding or “bar code” sign -> PTX
- Treatment: Depends on underlying cause
- Ultrasound findings to look for:
- Differential: Cardiac tamponade vs. RV infarction vs. severe pulm HTN/massive pulmonary embolism (PE) vs. asthmatic alveolar air trapping vs. tension pneumothorax (PTX)
- Ask yourself if there is an obstruction to the flow through the heart or the lungs? -> Obstructive shock
- Distended, non-collapsing IVC with dilated LV
- Move on to cardiac cause in step 3
- Normal IVC with diameter >2cm but <50% collapse with respiration
- May trial a small bolus of volume if lung auscultation is clear
- Move on to cardiac cause in step 3
- Flat/collapsed IVC (anteroposterior diameter of the IVC < 2 cm in size with > 50% collapse with respiratory variation) with hyperdynamic LV.
- Physical examination:
- Cardiac Performance:
- Assess this after you’ve determined that step 1 and 2 are normal. That is, the HR is not the cause of diastolic limitations to myocardial blood flow, intravenous volume is adequate, and there is no obstruction to flow through the thoracic circuit.
- Physiology: ↓ Cardiac Contractility -> ↓ Stroke Volume -> ↓ Cardiac Output -> Hypotension
- Approach: Assess myocardial performance by cardiopulmonary physical examination, ECG, and bedside ultrasound to assess left ventricular (LV) function.
- Physical examination
- High-pitched holosystolic murmur radiating to axilla?
- Diastolic murmur at RUSB radiating to LLSB?
- Systolic murmur at RUSB radiating to neck?
- Crackles/rales?
- Elevated JVP or obvious JVD?
- Peripheral edema?
- Ultrasound – Short axis parasternal view
- Do the LV walls collapse well in systole?
- If not, there is decreased LV contractility/EF
- Treatment: inotropy to move blood forward +/- vasopressors to increase SVR/diastolic pressure and hence coronary perfusion.
- Is volume truly going forward? -> Acute mitral regurgitation (MR) or acute aortic regurgitation (AR)
- Murmur and rales on exam with multiple B lines on lung sonography
- If not, there is decreased LV contractility/EF
- Do the LV walls collapse well in systole?
- Physical examination
- Differential: Cardiogenic shock (Decompensated heart failure, acute MI, acute MR, acute AR)
- Systemic Vascular Resistance:
- If 1-3 are okay, then the pt is hypotensive despite a HR allowing diastolic filling of LV lumen and coronary arteries, adequate intravenous volume, no obstruction through the pulmonary circuit and hence adequate LV diastolic volume, and adequate contractile function with forward flow out the aortic root. In this setting, there must be a component of peripheral vasodilation to explain low intravascular tone at the measured artery.
- Physiology: Since blood pressure is a balance of cardiac output and systemic vascular resistance, decreasing SVR can result in hypotension.
- Approach:
- Physical examination
- How do the extremities feel? Are they warm and vasodilated? Or are they cold, clamped and vasoconstricted?
- Physical examination
- Differential: Distributive shock (sepsis, anaphylaxis, vasodilatory medication overdose, neurogenic shock, fulminant liver failure, and other causes of severe acidemia including toxic ingestion, inherent metabolic disturbance, or mitochondrial poisons like cyanide, hydrogen sulfide, & carbon monoxide).
- Treatment: Depends on underlying cause
Bottom Line/Pearls & Pitfalls
Treat the patient, not the number. A blood pressure of 120/80 mmHg in a chronically hypertensive patient can be dangerously low. Whatever the HPI may suggest, unbiased implementation of the bedside physical examination and sonography are crucial in the workup of unexplained hypotension. The four step systematic approach of sequentially assessing heart rate, volume status, cardiac performance, and systemic vascular resistance can narrow the differential and guide management. Furthermore, recent RCT evidence has shown that goal-directed ultrasound can lead to “fewer viable diagnostic etiologies and a more accurate physician impression of final diagnosis.”
We highly recommend EM physicians read and implement the following various available bedside ultrasound examinations into their practice:
- RUSH protocol (Rapid Ultrasound in Shock and Hypotension)
- ALiEM
- emCrit podcast
- EM Curious
- emDocs post – Yes, shameless plug
- CORE scan (Concentrated Overview of Resuscitative Efforts)
- FAST exam (Focused Assessment with Sonography in Trauma)
- ACES protocol (Abdominal and Cardiac Evaluation with Sonography in Shock)
Acknowledgement
We would like to thank Dr. Ravi Morchi for allowing us to share this approach to hypotension. He came up with this method and has been teaching this technique to the emergency medicine residents at Harbor-UCLA Medical Center since 2009.
References // Further Reading
- Atkinson PRT, McAuely DJ, Kendall RJ. Abdominal and Cardiac Evaluation with Sonography in Shock (ACES): an approach by emergency physicians for the use of ultrasound in patients with undifferentiated hypotension. Emergency Medicine Journal. 2009; 26: 87-91
- Klabunde, RE. The Pharmacologic Treatment of Hypotension. Cardiovascular Pharmacology Concepts, 2007.
- Jones AE., et al. “Randomized, controlled trial of immediate versus delayed goal-directed ultrasound to identify the cause of nontraumatic hypotension in emergency department patients*.” Critical care medicine 32.8 (2004): 1703-1708.
- Morchi, R. Lecture in Undifferentiated Hypotension. 2014.
- Perera P, Mailhot T, Riley D, Mandavia D. The RUSH exam: rapid ultrasound in shock in the evaluation of the critically ill. Emergency Medicine Clinics of North America. 2010; 28(1): 29–56.
- Weekes AJ, Zapata RJ, Napolitano A. Symptomatic hypotension: ED stabilization and the emerging role of sonography. EM Practice 2007, Nov 1;9(11).
- Weingart SD, Duque D, Nelson B. Rapid ultrasound for shock and hypotension (RUSH-HIMAPP). 2009; http://emedhome.com/.
- Wu, Teresa. The CORE Scan: Concentrated Overview of Resuscitative Efforts. Critical Care Clinics. January, 2014.






6 thoughts on “The Hypotensive ED Patient: A Sequential Systematic Approach”
I missed this, but thanks to Dr. Kline (@klinelab) for relaying this RCT from 2004: http://www.ncbi.nlm.nih.gov/m/pubmed/15286547/ -> Goal-directed ultrasound can lead to fewer viable diagnostic etiologies and a more accurate physician impression of final diagnosis. Updated post with this info.
Pingback: LITFL Review #163 - LITFL
Pingback: Undifferentiated hypotension | First10EM
Pingback: Why your patient might be hypotensive | FOAM links
Pingback: emDOCs.net – Emergency Medicine EducationEM Educator Series: Challenging Diagnosis of Cardiogenic Shock - emDOCs.net - Emergency Medicine Education
Pingback: LITFL Review 163 • LITFL Medical Blog • FOAMed Review