Authors: Wes Trueblood, MD (EM Resident at SAUSHEC, USAF) and Erica Simon, DO, MHA (@E_M_Simon, EM Chief Resident at SAUSHEC, USAF) // Edited by: Alex Koyfman, MD (@EMHighAK, EM Attending Physician, UTSW / Parkland Memorial Hospital) and Brit Long, MD (@long_brit, EM Staff Physician at SAUSHEC)
You’re working a busy pediatrics pod shift, seeing a seemingly endless stream of febrile toddlers, when a nurse calls you bedside to evaluate a 17 year-old male presenting with abdominal pain and rectal bleeding. VS include HR 110, RR 14, BP 120/82, T 101.4. Review of systems is notable for three episodes of non-bloody, non-billious emesis prior to presentation. Although the patient reports a history of similar episodes over the previous eight months duration, he attributes his failure to seek treatment to the episodes’ self-resolving nature. The patient’s mother, present during the interview, notes a family history of “bowel disease.”
What is the next step in the evaluation and treatment of this patient? Should you order a CT abdomen and pelvis? Let’s take a minute to review Inflammatory Bowel Disease (IBD).
Background
IBD is comprised of Crohn’s Disease (CD) and Ulcerative Colitis (UC). Crohn Disease is characterized by transmural inflammation of the bowel wall anywhere from mouth to anus.1 Ulcerative Colitis is inflammation limited only to the colonic mucosa, in a continuous fashion from the rectum to the cecum.2
Epidemiology of IBD
The incidence of CD is reported as 20.2 per 100,000 person years in the U.S., 12.7 per 100,000 person-years in Europe, and 5.0 per 100,000 person-years in Asian and Middle Eastern Countries.3
The incidence of UC is 19.2 per 100,000 person-years in the U.S., 24.3 per 100,000 person-years in Europe, and 9.3 per 100,000 person years in Asian and Middle Eastern Countries.3 Literature notes geographic variation in both the U.S. and Europe, with a high prevalence of IBD in more northern latitudes.4 Cigarette smoking, Jewish ethnicity, and obesity have all been implicated as factors that influence the risk of developing IBD.4
The Role of the Emergency Physician
Patients with IBD frequently present to the emergency department for the treatment of flares. It is the role of the emergency physician to resuscitate and restore fluid and electrolyte balance, evaluate and control pain/fever/nausea, and to identify manifestations of IBD requiring urgent and emergent intervention (obstruction, intra-abdominal abscess and fistula formation, life-threatening hemorrhage, and toxic megacolon).5
Stabilizing the Patient
The evaluation of any emergency department patient begins with an assessment of the ABCs. In extreme cases, patients with complications of IBD may require intervention to address an acute abdomen, severe sepsis, altered mental status, or hemodynamic instability secondary to GI hemorrhage.5
Obtaining an Appropriate Medical History
Once acute life threats have been addressed, history taking begins with a review of the patient’s presenting symptoms. Typical symptoms of IBD include abdominal pain, anorexia, diarrhea with hematochezia, fever, and weight loss.1,2 Because of the relapsing and remitting nature of IBD, symptoms are often present and intermittent for months to years before a formal diagnosis is made.6 It is important to note that a small minority of patients with CD may report oral, esophageal, and gastric symptoms, which may clinically be mistaken for gastritis or peptic ulcer disease.1
The presentation of UC is variable and ranges from intermittent soft stools with small blood to daily diarrhea with continuous bleeding.2 The severity of presenting symptoms is commonly proportional to the extent of colonic involvement, with pancolitis being the most severe manifestation.2,5,6
Extra-intestinal manifestations occur with similar frequency in both CD and UC (50% of cases.)1,2 Patients may experience complications associated with: joints (sacroiliitis), vision (uveitis, episcleritis), integumentary system (erythema nodosum, pyoderma gangrenosum), hepatobiliary system (primary sclerosing cholangitis, hepatitis, pancreatitis, cholangiocarcinoma), vascular system (thromboembolic disease), the kidneys (nephrolithiasis), and the hematopoietic system (anemia).1-4
Physical Exam
Elements of the physical exam should include an assessment of:5
- The patient’s general appearance, evidence of acute or systemic toxicity, or sepsis.
- Complete vital signs noting the presence of fever, tachycardia, and hypotension.
- Physical examination with particular focus on the abdomen and areas where extra-intestinal manifestations of IBD are known to occur +/- visual rectal examination.
Differential Diagnosis
In a patient presenting with abdominal pain, fever, diarrhea or bloody/mucoid stools, it is important to consider the following differential diagnoses:1,2
- Appendicitis
- Diverticulitis
- Diverticular colitis
- Ischemic colitis
- Obstructing carcinoma
- Invasive diarrhea
- Medication associated colitis (NSAIDS)
- Lymphoma
- Endometriosis
- Carcinoid
Laboratory Testing
Laboratory testing in acute IBD is aimed at differentiating IBD from IBS, determining a diagnosis of IBD, and differentiating CD from UC.7 Laboratory studies to be obtained in patients suspected of having an acute flare of IBD, extra-intestinal manifestation of IBD, or a surgical complications of IBD include:7
- CBC, BMP, LFTs, ESR, CRP, and lipase +/- lactate
- Common basic lab abnormalities include normocytic or microcytic anemia, leukocytosis, thrombocytosis, elevated ESR and CRP, and mild elevations in AST/ALT.
- For patients presenting with bloody diarrhea consider: stool culture and leukocytes, ova and parasite analysis, antigen testing for Clostridium Difficile, Shigella, Coli, Yersinia, Campylobacter, Giardia, and Entameoba.8
Imaging Evaluation
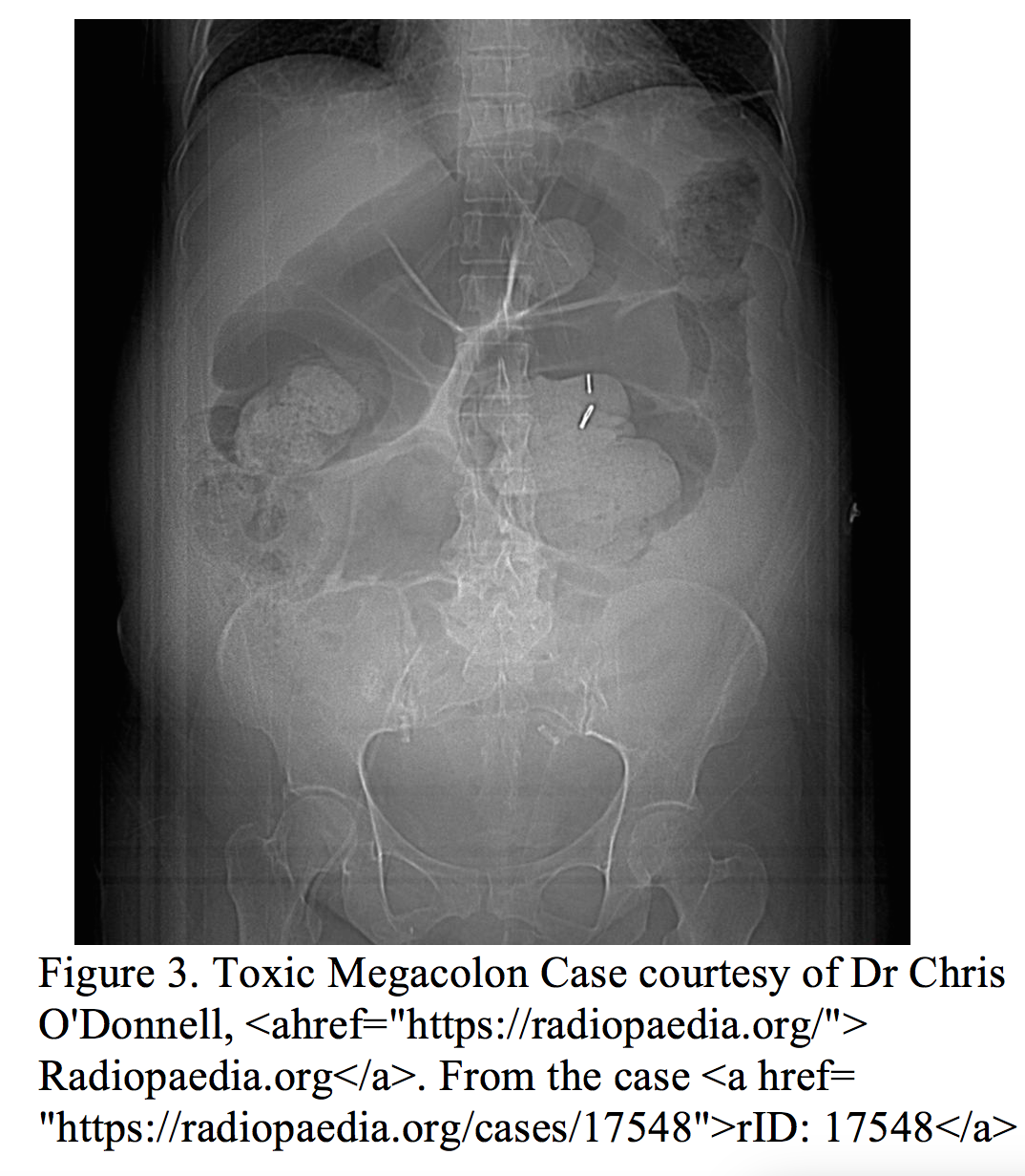
While plain radiography w/wo contrast, MRI, ultrasound, capsule endoscopy, and nuclear medicine techniques have all been utilized in the outpatient evaluation of IBD, the availability, ease, cost, and diagnostic capability of computed tomography have made it the imaging modality of choice to assess for emergency complications of IBD (specifically abscess, tumor, stricture, obstruction, fistula, and intestinal perforation).9 The main utility of plain radiography in the acute setting is in the diagnosis of obstruction (air fluid levels) and toxic megacolon ( dilated loops of bowel > 6 cm, loss of haustral markings, +/- thumb printing from mucosal edema – Figure 3) in clinically unstable patients for whom transfer to CT is considered unsafe.9 Plain films should include an upright chest and abdomen to evaluate for free air, and a supine KUB to assess the diameter of bowel loops. 9,10
In terms of imaging, there is a higher proportion of clinically actionable findings in patients presenting with new or worsening gastrointestinal symptoms secondary to CD as compared to UC.11 In a 2014 retrospective review of 354 patients with a known diagnosis of IBD presenting to the ED with new or worsening gastrointestinal symptoms, the yield of abdominal CT for clinically actionable findings (defined as abscess or tumor, bowel perforation, bowel obstruction, fistulae, diverticulitis, choledocholithiasis, or appendicitis) was 32.1% for CD and 12.8% for UC (p<0.01) (NNT = 3).11
Among the study participants, patients with CD and clinically actionable findings on CT were more likely to be African American, possess a lower BMI, less frequently utilize 5-ASA medications, and exhibit higher WBC and CRP levels.11 There were no significant predictive factors associated with surgical findings in UC.11
The European societies for Crohn’s and Colitis (ECCO) and for abdominal and gastrointestinal radiology (ESGAR) have developed joint guidelines for emergency radiologic evaluation of inflammatory bowel disease based on symptomatology:
- Acute gastrointestinal bleeding => endoscopy or capsule endoscopy (s/p stabilization and admission)
- IBD patient with acute abdominal pain => CT is 85% sensitive for diagnosis of intestinal perforation12
- When abdominal CT is used, IV contrast and water soluble oral contrast are recommended.12
It is important to note that lymphoma, chronic ischemia, endometriosis, and carcinoid can all give a radiologic and clinical picture that may be confused with CD of the small bowel.1,2
Treatment
The challenge for the emergency clinician is to differentiate an acute IBD flare from the more serious surgical complications detailed above.
Acute Flares
Acute flares of IBD are generally treated with intravenous fluids (for optimal correction of electrolyte abnormalities), high dose IV corticosteroids (e.g. solumedrol 1 mg/kg q12), and antibiotics if there is clinical concern for infectious colitis. A typical antibiotic regimen for an acute uncomplicated IBD flare is parenteral ciprofloxacin (1.0-1.5 mg/kg/day) and metronidazole (10-20 mg/kg/day).8
Continuation of maintenance medications should be a decision made in conjunction with a gastroenterologist. In general the immunomodulators (6-mercaptopurine or azathioprine) along with the anti-TNF agents (infliximab or adalimumab) are continued during acute flares.8 The salicylate agents sulfasalazine, mesalamine, and olsalazine are generally held during acute flares as they may paradoxically worsen symptoms in the acute time frame.8
IBD Complications
The treatment for bowel obstruction or ileus secondary to IBD includes NPO status, nasogastric suction and decompression, intravenous medications for pain and nausea, and correction of fluid and electrolyte abnormalities. Abdominal/pelvis CT is valuable in identifying the etiology of the obstruction (mass, abscess, stricture, fistula).11,12 If an intra-abdominal abscess or perforation is identified, broad spectrum antibiotic coverage should be initiated, and general surgery should be consulted.1,2
Toxic Megacolon
Toxic megacolon is a surgical emergency discovered in approximately 1% of patients with IBD presenting acutely with worsening abdominal pain, distention, signs of peritonitis, and systemic illness.8 Broad spectrum antibiotics, intravenous fluids, and expedited surgical consultation are imperative if toxic megacolon is suspected. Feared complications of toxic megacolon include perforation, peritonitis, sepsis, and hemorrhage.8
Disposition and Follow-Up
The disposition of IBD patients presenting with new or worsening symptoms is largely dependent on the presence or absence of surgical complications and the severity of the acute flare.8 Occasionally, mild exacerbations without surgical pathology may be treated on an outpatient basis with pain control and PO steroids; however, this should only be undertaken in consultation with a gastroenterologist.1,2,5 The majority of acute exacerbations will require admission and inpatient treatment.1,2,8
Key Pearls
- The role of the ED physician is to resuscitate, stabilize as necessary, evaluate for surgical pathology, and consult for further management.
- Imaging modality of choice for an IBD patient with abdominal pain => Abdominal/pelvis CT with IV and oral contrast
- Unless concern for perforation/megacolon => acute abdominal series to expedite management
- ED treatment priorities: pain/nausea control, correction of electrolyte imbalances +/- antibiotics given the clinical scenario
- Disposition => outpatient vs. inpatient in consultation with GI consult
References / Further Reading
- Peppercorn M, Kane S. Clinical manifestations, diagnosis and prognosis of Crohn disease in adults. UpToDate. 2016. Available from: https://www.uptodate.com/contents/clinical-manifestations-diagnosis-and-prognosis-of-crohn-disease-in-adults?source=search_result&search=irritable%20bowel%20disease&selectedTitle=3~150#H12689134
- Peppercorn M, Kane S. Clinical manifestations, diagnosis and prognosis of ulcerative colitis in adults. UpToDate. 2016. Available from: https://www.uptodate.com/contents/clinical-manifestations-diagnosis-and-prognosis-of-ulcerative-colitis-in-adults?source=search_result&search=ulcerative%20colitis&selectedTitle=1~150
- Molodecky NA, Soon IS, Rabi DM, Ghali WA, Ferris M, Chernoff G, Benchimol EI, Panaccione R, Ghosh S, Barkema HW, Kaplan GG. Increasing incidence and prevalence of the inflammatory bowel diseases with time, based on systematic review. Gastroenterology. 2012;142(1):46.
- Loftus EV Jr. Clinical epidemiology of inflammatory bowel disease: Incidence, prevalence, and environmental influences. Gastroenterology. 2004;126(6):1504
- Kman N, Werman H. Tintinalli’s Emergency Medicine. Ch 76 p 536-540.
- Farmer R, Hawk W, Turnbull R. Clinical patterns in Crohn’s disease: a statistical study of 615 cases. Gastroenterology. 1975;68:627.
- Cappello, Maria; Morreale, Gaetano. The Role of Laboratory Testing in Crohn’s Disease. Clin Med Insights Gastroenterol. 2016;9:51–62.
- Huang et al. Pediatric Inflammatory Bowel Disease in the Emergency Department: Managing Flares and Long Term Complications. Pediatr Emerg Med Pract. 2014;7(11):1-16.
- Israeli et al. The Impact of Abdominal Computed Tomography in a Tertiary Referral Centre Emergency Department on the Management of Patients with Inflammatory Bowel Disease. Alimentary Pharmacology and Therapeutics. 2013;38:513-521.
- Morgan M, Clopton D, et al. Toxic megacolon. Radiopedia.org. Available from: https://radiopaedia.org/articles/toxic-megacolon
- Yarur et al. Predictive Factors for Clinically Actionable Computed Tomography Findings in Inflammatory Bowel Disease Patients Seen in the Emergency Department with Acute Gastrointestinal Symptoms. J Crohns Colitis. 2014;8(6): 504-512.
- Panes et al. Imaging techniques for assessment of inflammatory bowel disease: Joint ECCO and ESGAR evidence-based consensus guidelines. J Crohns Colitis. 2013;7(7):556-585.




