Author: Erica Simon, DO, MHA (@E_M_Simon, EM Chief Resident at SAUSHEC, USAF) // Edited by: Alex Koyfman, MD (@EMHighAK, EM Attending Physician, UTSW Medical Center / Parkland Memorial Hospital) and Brit Long, MD (@long_brit, EM Attending Physician at SAUSHEC)
A 16 year-old male status post MVC rolls into the trauma bay. While EMS personnel bag the patient, they identify him as the front seat passenger in an auto vs. semi. Per witness reports, the young male was ejected nearly 200 feet from his vehicle. Attempts at endotracheal intubation in the field failed secondary to his severe facial trauma. Remarkably, the patient has a pulse; a c-collar and pelvic binder encircle his small frame. A nurse calls out a manual BP of 72/41, a HR of 147, and your team goes to work.
Within minutes the patient is intubated and ventilated. A compression dressing has slowed the bleeding from his large galeal avulsion to an ooze. The rapid infuser is pumping in a unit of O+ PRBCs, and your EFAST exam identifies a right-sided hemopneuomothorax.
Suddenly, the patient’s BP plummets. The head of the bed reports left tracheal deviation and a right hemithorax absent breath sounds. You quickly perform a needle decompression. As you puncture the pleura to place a chest tube, blood pours onto the floor for what seems like hours. You know immediately that this is a massive hemothorax. What do you do next? Let’s take a few minutes to review.
Epidemiology of Hemothoraces
A hemothorax, or a collection of blood in the pleural space, most commonly occurs secondary to penetrating or blunt chest wall trauma.1-5 In the United States, 70-80%1 of hemothoraces are due to motor vehicle collisions causing injury to mediastinal structures (the heart, major vessels, thoracic spine, intercostal or mammary arteries), the diaphragm, or the lung parenchyma.1-5
Diagnosing a Hemothorax
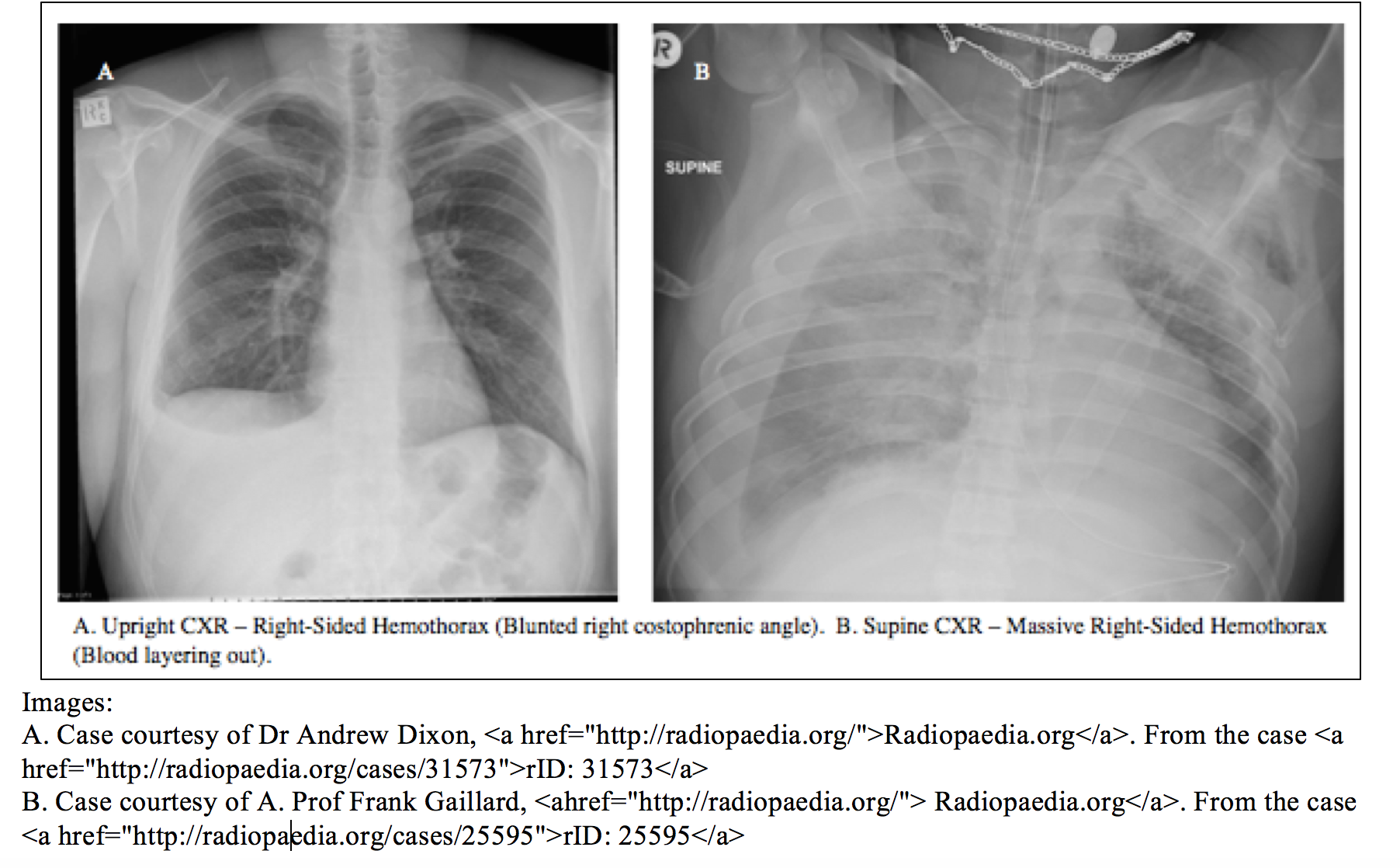
Patient presentations of hemothoraces range from shortness of breath (25% of hemothoraces are associated with concomitant pneumothoraces6), to hemodynamic instability secondary to hemorrhagic shock.4 In the hemodynamically stable patient, a hemothorax is most commonly identified on CXR.4-5 Ideally, the CXR should be performed in the upright position in order to detect blunting of the costophrenic angle (equating to 150-300 mL of blood in the pleural space).4-6 See image A below.
Note: An inadequate upright CXR, or CXR performed in the supine position is often misleading secondary to posterior diaphragmatic layering of blood. It is no surprise then that the sensitivity of a supine CXR in the detection of a hemothorax is reportedly 40-60%.5 In fact, studies have demonstrated only vague opacification of the hemithorax as detectable on supine CXR despite >1,000 mL of intrathoracic blood collection.5,6 See image B below.
What does this mean for the trauma patient for whom a supine CXR is likely to be performed?
If patient vital signs (hypoxia, persistent hypotension), mechanism of injury (penetrating injury), or physical exam (multiple palpable rib fractures, flail segment, significant chest wall ecchymosis or tenderness to palpation) lead you to suspect a hemothorax à Do not let the supine CXR convince you otherwise.
In the hemodynamically unstable patient, the EFAST or Extended Focused Assessment with Sonography for Trauma is most commonly utilized to identify a hemothorax given its speed of employment. Several studies have identified the sensitivity of ultrasound in the detection of hemothoraces as comparable to chest radiographs:
In their 1996-2007 MEDLINE search, utilizing the OVID interface, McEwan and Thompson7 cite the following:
| Author | Patient Population | Study Design | Outcomes | Key Result | Study Limitation |
| Rothlin et al., 1993, Switzerland8 | Adults (15-88yrs) with blunt thoracic or abdominal injuries. US performed by surgeons and compared to CXR & CT. | Prospective Study | Utility of US to detect hemothorax. | Sn = 81% | 5 of 11 False negative reports ultimately identified as operator error. |
| Ma et al., 1995, U.S.9 | 245 Adults (18+) presenting to the ED with blunt or penetrating torso trauma. US compared to CT, supine CXR, formal echo or chest tube. | Diagnostic Cohort | Utility of US to detect hemothorax. | Sn = 96% Sp = 100% | Composite gold standard. |
| Ma et al., 1997, U.S.10 | 240 Adults (18+) presenting to the ED with blunt or penetrating torso trauma. US compared to CT, supine CXR, formal echo or chest tube. | Retrospective Analysis of 1995 Study | Clinical utility of ultrasound vs. plain supine CXR. | Sn US = 96.2% vs. CXR = 96.2%; Sp US = 99.6% vs. CXR = 99.6% | Patient population from 1995 study utilized. |
| Sisley et al., 1998, U.S.11,12 | 360 trauma patients presenting to the ED with blunt or penetrating torso trauma. | Prospective Study | Clinical utility of US vs. supine CXR | Sn US = 97.5% vs. CXR = 92.5%; Sp US = 99.7% vs. CXR = 99.7% | Results compared to supine CXR vs. independent gold standard (CT). |
| Abboud & Kendall, 2003. U.S.13 | 155 trauma patients who underwent CT scan during their evaluation. | Prospective Study | Clinical utility of US | Sn = 92%, Sp = 100% | Composite gold standard. |
Table adapted from McEwan and Thompson’s Emergency Medicine Journal article, 2007.7 Sn = Sensitivity. Sp = Specificity.
What about CT?
CT remains the gold standard in the diagnosis and evaluation of hemothoraces. In their 2007 retrospective study of 141 blunt chest trauma patients presenting to a Level 1 trauma center, Traub et al. noted a hemothorax as detectable in 25% of patients, having been previously diagnosed with a negative supine CXR.14
Managing a Hemothorax
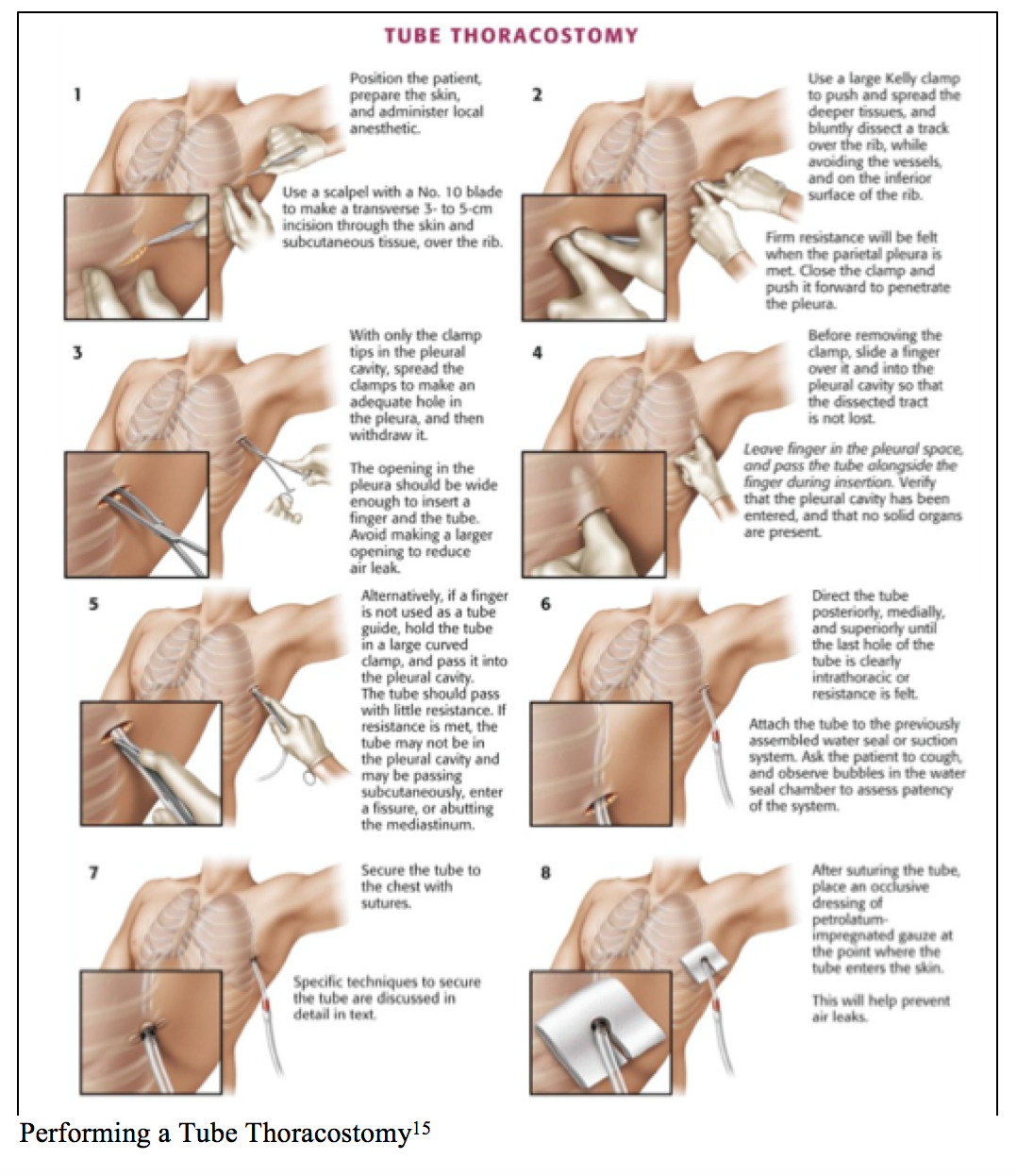
Volume resuscitation remains the #1 priority. Transfusion should be initiated as appropriate. Early consultation for penetrating chest trauma is recommended.4 As the majority of hemothoraces arise from injured lung parenchyma and are commonly self-limited, management with chest tube thoracostomy is frequently adequate.5 The placement of a chest tube is therapeutic in that expansion of the lung with apposition of the visceral and parietal pleural aids in hemostasis.4 Drainage of blood from the parietal cavity also prevents the common complication of empyema or fibrothorax.4,5
To perform tube thoracostomy, a large-bore tube (32F to 40F) should be placed in the 4th or 5th intercostal space at the anterior axillary line, and connected to water seal and suction (20-30 mL H20).5 Re-expansion of the lung parenchyma and resolution of the hemothorax should be monitored with serial CXRs.5
What is of major concern is the management of a massive hemothorax, defined as an immediate blood loss of >1,500 mL upon chest tube thoracostomy, or blood loss of >200 mL/hr (3mL/kg/h) over 2-4 hours post thoracostomy procedure.16,17 These, in addition to the conditions listed below, are recommended considerations for urgent thoracotomy:
- Increasing hemothorax demonstrated on repeat CXRs.5
- Hypotension despite adequate blood replacement (when other sites of blood loss have been ruled out).5
- Patient decompensation after initial response to volume resuscitation.5
An urgent/emergent thoracotomy should be performed as follows:
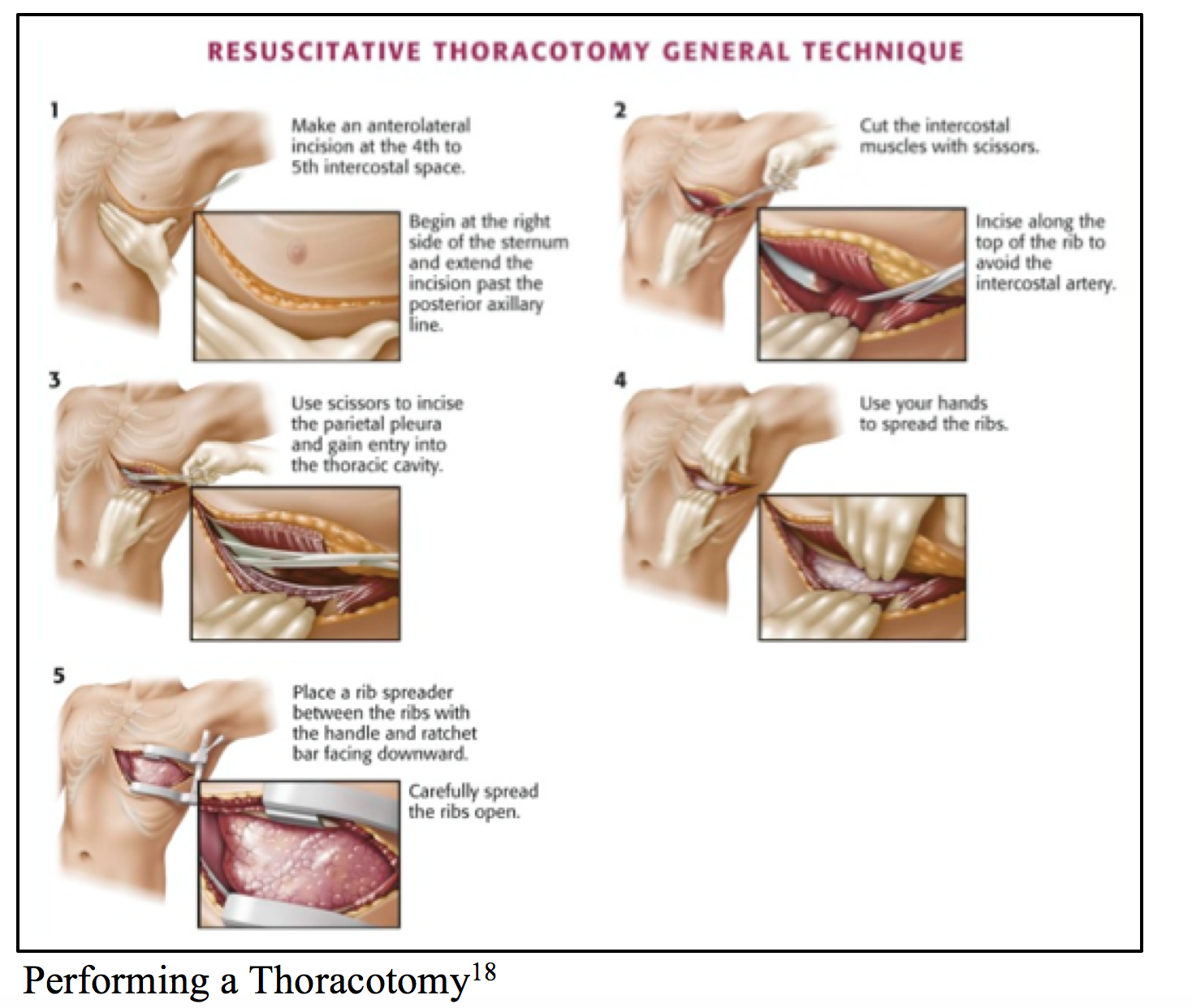
After the parietal pleura has been accessed, clamping of the lung hilum (pulmonary vasculature) may allow for the attainment of hemostasis.5
It is important to recognize that persistent hypotension, despite intervention to address bleeding from the lung parenchyma/hilum, points to additional injury. Perform a thorough patient assessment. Consider clamping the aorta if the patient remains hemodynamically unstable (the patient may later undergo trans-esophageal echocardiogram to assess aortic injury in the OR).5,6
Special Topics – Auto-Transfusion
To date, one French case study detailed the use of pre-hospital autologous blood transfusion in the setting of life-threatening hemothorax.19 In the study, 18 patients with life-threatening hemothoraces received autologous blood obtained from the thorax; 13 survived to the hospital setting. Post transfusion laboratory studies and vital signs for the 13 patients revealed: Hct decrease from 24 +/- 3 to 19 +/- 3 and SBP increase from 78 +/- 11 to 88 +/- 12 mm Hg. Platelet count was noted as 90,800 +/- 21,400/cu mm, prothrombin time 48 +/- 3%, partial thromboplastin time 197 +/- 18%, and serum potassium levels 3.6 +/- 0.5 mmol/L. According to the authors, no serious complications related to auto-transfusion were deemed crucial to the patients’ survival.19
This is an area that requires further study as researchers have now determined the following:
- There is a statistically significant increase in pro-inflammatory cytokines (IL-6, IL-8, TNFα, GM-CSF) in shed pleural blood when compared with samples from healthy controls (P <0.05). Cytokine levels in unprocessed shed pleural blood are approximately 10- to 100-fold higher compared with healthy control venous samples.20 Thus, these pro-inflammatory cytokines may inhibit healing and stimulate transfusion reactions through systemic inflammatory cascades.
- Unprocessed shed hemothorax blood (USHB) is significantly depleted of coagulation factors as compared to venous blood: In a study of 22 patients undergoing sampling of hemothorax blood and venous blood s/p traumatic injury: the INR of USHB was >9 as compared to a venous blood INR of 1.1 (p< .001), the aPTT of USHB was >180 in contrast to 28.5 seconds in the venous blood sample (p< .001), and the fibrinogen of USHB was <50 in comparison to 288 mg/dL in the venous blood sample (p< .001).21 Therefore, it would seem that little benefit in terms of hemostasis may be achieved in the transfusion of USHB.
- Also of note, in the same study, the mean Hct of USHB was found to be 26.4 in contrast to 33.9 for venous blood (p = .003); Hgb was 9.3g/dL in comparison to a venous blood level of 11.8 g/dL (p = .004), and the platelet count of the USHB was 53 in contrast to 174 K/μL in the venous blood sample (p < .001). Ultimately, a hemothorax volume of 726 mL was calculated to be equivalent to 1 U of red blood cells.21
Summary
The emergency physician’s role in addressing a hemothorax is first to make the diagnosis utilizing CXR, US or CT. Hemothoraces should be managed with the placement of a chest tube to avoid the later complications of empyemas and fibrothorax. Massive hemothoraces warrant volume resuscitation, consultation with a trauma surgeon, and performance of a thoracotomy. Early identification and intervention is the key to limiting the morbitidy and mortality associated with hemothoraces.4-6
Key Pearls
- Hemothorax presentation is variable
- Step 1: Diagnose the hemothorax with CXR vs. US definitively with CT
- If the mechanism suggests hemothorax = rule out hemothorax despite CXR findings (CT if patient hemodynamically stable)
- Hemothorax Treatment = Chest tube
- Massive Hemothorax Treatment = Transfuse, consult, thoracotomy PRN
- If the patient is persistently hypotensive despite control of pulmonary bleeding => look for other etiologies
- Auto-transfusion of unprocessed shed hemothorax blood => additional research needed
References / Further Reading
- Shorr R, Crittendenn M, Indeck M, Hartunian S, Rodriguez A. Bunt thoracic trauma. Analysis of 515 patients. Ann Surg. 1987;206(2):200-205.
- Meyer D. Hemothorax related to trauma. Thorac Surg Clin. 2007;17:47-55.
- Roodenburg B, Roodenburg O. Chest trauma. Anaesth Intensive Care. 2014; 15(9):411-414.
- Bernardin B, Troquet J. Initial management and resuscitation of severe chest trauma. Emerg Med Clin N Am. 2012;30:377-400.
- Eckstein M, Henderson S. Thoracic Trauma. Rosen’s Emergency Medicine. Ch 45, 431-458.e3.
- Meyer D. Hemothorax related to trauma. Thorac Surg Clin. 2007;47.
- McEwan K, Thompson P. Ultrasound to detect heamothorax after chest injury. Emerg Med J. 2007; 24(8):581-582.
- Rothlin M, Naf R, Arngwerd M, Candinas D, Frick T, Trentz O. Ultrasound in blunt abdominal and thoracic trauma. J Trauma. 1993; 34(4):488-495.
- Ma O, Mateer J, Ogata M, Kefer M, Witmann D, Aprahamian C. Prospective analysis of a rapid trauma ultrasound examination performed by emergency physicians. J Trauma. 1995; 38(6):879-885.
- Ma O, Mateer J. Trauma ultrasound examination versus chest radiography in the detection of hemothorax. Ann Emerg Med. 1997; 29(3):312-315.
- Sisley A, Rozycki G, Ballard R, Manias N, Salomone J, Feliciano D. Rapid detection of traumatic effusion using surgeon-performed ultrasonography. J Trauma. 1998; 44(2):291-297.
- Noble V, Nelson P. Manual of emergency and critical care ultrasound. (2011). Cambridge University Press, New York.
- Abboud P, Kendall J. Emergency department ultrasound for hemothorax after blunt traumatic injuy. J Emerg Med. 2003;25(3):181-184.
- Traub M, Stevenson M, McEvoy S, Briggs G, Lo S, Leibman S. Joseph T. The use of chest computed tomography versus chest x-ray in patients with major blunt trauma. Injury. 2007; 38(1):43-47.
- Kirsch T, Sax J. Tube Thoracostomy. Chapter 10. Roberts and Hedges’ Clinical Procedures in Emergency Medicine. p.189-211. Elsevier Saunders, Philadelphia, PA.
- Kortbeek J, Al Turki S, Ali J, Antoine J, Bouillon B, Brasel K, et al. Advanced trauma life supports, 8th editions, the evidence for change. J Trauma. 2008:64(6):1638-1650.
- Legome E, Shockley L. Trauma: A comprehensive emergency medicine approach. 2011. Cambridge University Press, New York.
- Jones R, Rivers E. Resuscitative Thoracotomy. Chapter 18. Roberts and Hedges’ Clinical Procedures in Emergency Medicine. p.325-339. Elsevier Saunders, Philadelphia, PA.
- Barriot P, Riou B, Vlars P. Prehospital autotransfusion in life-threatening hemothorax. Chest. 1988;93(3):522-526.
- Salhanick M, Sams V, Pidcoke H, Fedyk C, Scherer M, et al. Shed pleural blood from traumatic hemothorax contains elevated levels of pro-inflammatory cytokines. Shock. 2016;46(2):144-148.
- Salhanick M, Corneille M, Higgins R, Olson J, Michalek J, et al. Autotransfusion of hemothorax blood in trauma patients: is it the same as fresh whole blood? Am J Surg. 2011;202(6):817-821.






5 thoughts on “Managing a Massive Hemothorax: A Guide to Stabilizing Your Patient”
Great review – thanks for posting!
dont forget the TXA in any trauma patient presenting within 3 hours of initial injury with an elevated shock index (among other TXA administration criteria), overall great review
Wonderful information!Thanks for sharing these information in this post.
Wonderful summary!! Thank you, I have taken note of all the little details. ?
Wonderful summary!! Thank you, I have taken note of all the little details. ?