
Authors: Forrest Turner, MD (PGY-3, Emergency Medicine, Carolinas Medical Center); Bryant Allen, MD (@bryantkallen, Attending Physician, Emergency Medicine, Carolinas Medical Center) // Reviewed by Marina Boushra, MD; Alex Koyfman, MD (@EMHighAK); Brit Long, MD (@long_brit)
Case:
A 42-year-old male presents following a front-end high-speed motor vehicle collision. He was traveling approximately 50 mph when he lost control of the vehicle. He was unrestrained and there was ejection into a guardrail. On the scene, he was placed in a cervical collar and transported by EMS. On arrival, he has obvious facial injury, with active bleeding from the midface/nares and oral gurgling blood. Breath sounds are rhonchus but symmetric and there is no other obvious external bleeding or evidence of trauma. Prehospital vital signs are maximal heart rate 119 beats per minute, lowest blood pressure 135/80 mmHg, respiratory rate 26 breaths per minute, SpO2 94% on 15L non-rebreather, GCS is 9 (E1V2M6) as he follows commands but is intermittently combative.
Introduction
Traumatic injuries to the face present a broad set of challenges to emergency physicians. The burden of disease can range from minor facial lacerations to life-threatening airway compromise. While injuries to the head, face, neck account for nearly 5% of emergency department visits, the majority are not severe and are discharged home.1 Of the more severe cases, as many as 42% will require intubation, requiring cautious and expeditious airway management.1 In these severe cases, case series have shown an associated incidence of 44% for intracerebral hemorrhage, 6% for vision loss, and a 9% mortality rate.2,3 This, when considered alongside the importance of the face in appearance, speech, vision, mastication, and sensation, suggests a significant risk of morbidity with these important aspects of the primary survey in patients with maxillofacial trauma as well as the evaluation and management of frontal, orbital, nasal, midface, and mandibular injuries.
Airway and Breathing – Examination and Preparation
The primary survey provides a framework to quickly assess and intervene on immediate life threats. In the case of significant facial trauma, this usually directs attention to securing the airway if necessary.
Careful examination of the airway can provide valuable information as to what challenges may be faced. Significant hemorrhage, whether venous or arterial, can result from facial fractures. Large bore suction (preferably two sources) is invaluable. Avulsed dental fractures, dentures, vomitus, and fragments of soft tissue or bone are just some of the potential surprises that can obstruct intubation attempts; a ringed forceps or similar instrument may be a useful adjunct. If digital manipulation of the oropharynx is necessary, the finger should be swept laterally just inside the cheek and hooked medially and out; a centrally-inserted finger runs the risk of pushing foreign bodies further into the airway. Facial fractures are prone to swelling and edema of the upper airway, so physicians must be especially vigilant in cases with a delayed presentation or who are being observed. Mandibular fractures can compromise the anterior insertion of the tongue, displacing it posteriorly if the patient is supine. Dry gauze, a towel clip, or #0 suture (placed transversely through the dorsum of the tongue) can help control these structures. Additionally, raising the head of bed, spinal precautions permitting, is helpful in preventing blood, foreign objects, and traumatized structures from falling into the airway and reducing the risk of aspiration.4,5
Nasal pharyngeal airway (NPA) devices can be helpful when bag-valve-mask (BVM) ventilation is difficult. However, NPA is contraindicated in cases of facial trauma and basilar skull fracture, based on two case reports documenting malposition of nasal airways into the central nervous system (CNS).6,7 Further, nasal hemorrhage and fracture can make the placement of an NPA more difficult. Maxillary fractures can also displace the midface posteroinferiorly, completely occluding the nasal airway.5
Video laryngoscopy has shown superiority when compared to direct laryngoscopy in multiple studies, especially in cases where cervical motion is to be minimized.8,9 Multiple adjuncts and backup devices such as supraglottic devices and gum elastic bougies can contribute to success. Aggressive preoxygenation and the use of apneic oxygenation (using some combination of nasal cannula, non-rebreather mask, and BVM) can increase the time to desaturation. In cases where assisted BVM ventilation is necessary, the two-person technique is often required to obtain a good seal in cases where the normal contour of the face is distorted. Preparation should be made in advance to anticipate a “cannot intubate, cannot ventilate” scenario, in which case surgical cricothyrotomy is indicated. In preparation, physicians should examine the neck and have equipment for a surgical airway ready at the bedside (double setup). While rapid sequence intubation (RSI) is usually the preferred method of airway management, if time permits, patients with facial trauma and anticipated difficult airways are excellent candidates for awake intubation using either ketamine or etomidate, in addition to topicalization with anesthetic.4,9
Circulation – Hard to Reach Bleeds
The importance of achieving hemostasis in cases of maxillofacial trauma is two-fold: to reduce airway obstruction as discussed above and to reduce hemorrhagic volume loss. While life-threatening hemorrhage from facial fractures is uncommon, it may be present in as many as 10% of cases of severe facial injury. Primary sources of hemorrhage include branches of the internal carotid such as the ophthalmic and ethmoid arteries, as well as branches of the external carotid such as the maxillary artery. In cases of external or intraoral hemorrhage, direct pressure, packing, and suture are usually sufficient. In cases of epistaxis, routine techniques for anterior epistaxis can be used: direct pressure, various tamponade devices, tampon/other packing, topical tranexamic acid (TXA). If posterior packing is required, the use of a posterior tamponade device (i.e. Rhino Rocket) or Foley catheter bulb technique in combination with anterior nasal and intraoral packing is recommended. Use caution with posterior packing for reasons mentioned above regarding NPA insertion, as basilar skull fracture can result in malposition intracranially. Inserting a Foley catheter or other posterior packing device until directly visualized in the oropharynx and then applying traction can assist with appropriate placement. When bleeding persists beyond these techniques, it is important to seek specialist consultation with interventional radiology, ENT, or surgery to perform arterial embolization, fracture reduction, or external carotid artery ligation, respectively.4,10
Secondary Survey
Once immediate life threats have been addressed, a thorough top-to-bottom evaluation of the extent of facial injuries is required followed by deciding to proceed with imaging. In general, CT of the face is the gold standard for imaging of facial fractures, with axial, coronal, and sagittal as well as 3-D reconstructions maximizing sensitivities for most types of fracture to greater than 90%.4,11,12 When suspicion is low, a CT of the head provides a look at the facial structures but is only 80% sensitive for facial fracture.13 In settings where access to CT is limited, a single Waters view is a valid screening tool, although one study demonstrated plain radiography missing as many as 38% of fractures.14 While data discussing injuries missed on initial facial CT is limited, clinical acumen and physical examination should not be neglected. For example, isolated pterygoid fractures were associated with occult mandible fractures in all seven patients in one case series.15
Frontal Bone Fracture
Evaluation – Being the strongest of the facial bones, frontal bone fractures are associated with high energy mechanisms and concomitant injuries including intracranial injury, orbital injury, basilar skull fractures, and temporal bone injury. Physicians should evaluate for signs of cranial nerve injury such as paresthesia, hearing or vision loss/changes, as well as rhinorrhea or otorrhea which suggests cerebrospinal fluid (CSF) leak. Lacerations will usually overlie frontal sinus fractures; crepitus may also suggest sinus involvement. CT imaging should be obtained both to investigate for intracranial injury and evaluate the anterior and posterior tables of the frontal sinus.
Management – Isolated anterior table fracture can be managed as an outpatient by a facial surgeon (e.g. ENT, plastic surgery). All sinus fractures have historically been managed using antibiotic prophylaxis, with first-generation cephalosporins or amoxicillin-clavulanic acid being the most commonly used choices. Involvement of the posterior table, which forms part of the anterior cranial fossa and is attached to the dura, is associated with CSF leaks, pneumocephalus, and CNS infection, warranting neurosurgical consultation and repair.4,16,17
Orbital Fracture
Evaluation – Seven bones form the orbit, with the medial and inferior walls being the weakest (Figure 1). Orbital fractures are often associated with frontal, zygomatic, and maxillary fractures. The examination should include palpation of the entire orbital rim, evaluation for crepitus, and assessment for the presence of enophthalmos (eye sunken back), subtle ocular motility deficits, diplopia, blurry vision, numbness to the cheek, or eyelid swelling. During the examination, the patient should be instructed to fully open their eyes; if eye-opening is easy and symmetric (or smooth with little resistance against the examiner’s finger) this is reassuring against significantly elevated intraocular pressure.
Figure 1: The bones forming the orbit

Fracture of the orbital floor is the most common type of orbital injury. Inferior rectus entrapment with subsequent superior gaze deficit and infraorbital nerve paresthesia are common associated findings. Nausea, vomiting, and bradycardia, symptoms usually associated with increased intracranial pressure, are possible due to reflexes associated with the trigeminal nerve.18 The second most common site of injury is the medial wall of the orbit, which is associated with orbital emphysema from ethmoid sinuses, telecanthus, tear outflow obstruction, and bleeding from the ethmoidal arteries brisk enough to cause a retrobulbar hematoma. When investigating the orbit for injury, as discussed above, facial CT with multiplanar reconstructions is highly sensitive.11,12
When concerned for trauma around the eye, physicians should perform a thorough eye exam, especially before worsening swelling can make it more difficult later. As many as 15% of orbital fractures are associated with ophthalmologic emergencies with morbidity often superseding that seen with orbital fractures. 4,19 This discussion will not cover ocular injuries (see: http://www.emdocs.net/core-em-traumatic-ocular-injuries/) but corneal abrasions, globe ruptures, iritis, retinal/vitreous injuries, and optic nerve injury can be subtle and vision threatening.4,19
Management – Orbital fractures usually warrant discussion with a facial surgeon. Most orbital blowouts can be followed up as an outpatient. Linear or trapdoor fractures can cause entrapment of extraocular muscle. While entrapment can resolve spontaneously, tissue ischemia is possible and demands urgent consultation.
Patients with orbital fractures should be prescribed oral decongestants and instructed to avoid nose blowing until seen for follow-up. Orbital emphysema can create a compartment syndrome similar to a retrobulbar hematoma, so patients should be counseled on return precautions including worsening orbital pain or diminished vision. Cold packs are a useful adjunct for analgesia and swelling. If the fracture extends into a sinus, prophylactic antibiotics may be given to prevent orbital cellulitis, although evidence for this practice remains weak. Amoxicillin-clavulanate is first-line.4,12
Nasal Fracture
Evaluation – Nasal fractures account for the majority of facial fractures. External evaluation involves close inspection and palpation for deformity or crepitus. The examiner should rock the bridge of the nose to evaluate for midface for stability. Periorbital ecchymoses is often associated with nasal bone fracture. A driver’s license or cell phone picture can help provide a reference for the pre-injury shape of the patient’s nose. Epistaxis is common but vigilance for clear rhinorrhea suggesting CSF leak is of utmost importance. Internal exam requires close inspection for septal hematoma, but patient discomfort, blood clot, and dried blood can make for a suboptimal exam. Warm saline irrigation should be considered, with the addition of topical anesthetic vasoconstricting agents, i.e. phenylephrine, cocaine, oxymetazoline.20
Plain films are usually unnecessary as most isolated nasal fractures can be diagnosed clinically. If there is concern for other facial fractures, CT is the diagnostic modality of choice. CT imaging for naso-orbitoethmoid (NOE) fractures should be considered if there is suspicion for high-energy mechanism.4
Management – Fractures with associated lacerations, whether externally or internally, should be treated as an open fracture. Septal hematomas require incision and drainage to prevent saddle deformity or abscess formation. Following decompression, the nares should be packed with next-day ENT follow-up and a prescription for antibiotics (amoxicillin-clavulanate).4
Ice and head elevation are simple measures to improve pain and swelling for nasal fractures. For simple, unilateral fractures that present to the ED within 4-6 hours, prior to edema setting in, it is reasonable to attempt closed reduction in the emergency department if the physician is comfortable doing so and the patient is appropriately counseled, consented, and anesthetized. Helpful graphics can be found in the literature.21 Whether reduced or not, the patient should follow up with ENT in 3-10 days.4,22
Midface Fracture
Evaluation – On inspection, zygoma fractures can demonstrate flattening of the malar eminence. Trismus is an associated feature. Zygomaticomaxillary (also called tripod or quadripod) fractures involve the orbit and sinuses and are associated with ocular findings and crepitus.
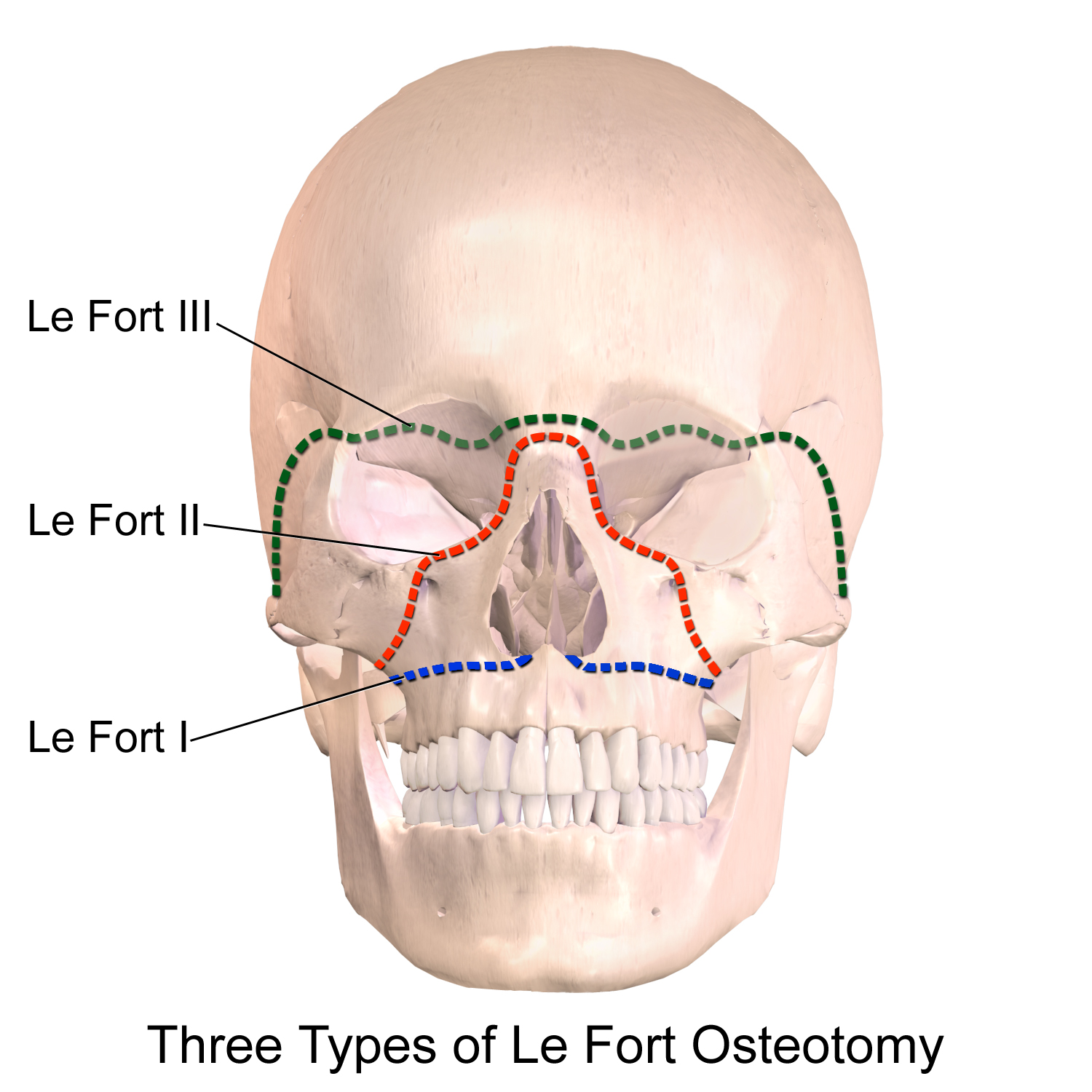
Le Fort injuries of the maxilla are high-energy injuries, carrying an increased incidence of cervical, intracranial, and ocular injuries.23,24 Associated findings include significant edema, bleeding, CSF leaks, and bilateral periorbital ecchymoses. Palpation of the midface and pulling on the hard palate will demonstrate instability. Fracture patterns are characterized by location transversely through the body of the maxilla (Le Fort I), pyramidally through the hard palate and above the nose (Le Fort II), through the entirety of the midface across the orbits (Le Fort III), or higher with frontal bone involvement (Le Fort IV) (Figure 2).23,24
Figure 2: Le Fort fracture patterns
Management – Zygomatic arch fractures can usually follow up as an outpatient. Tripod injuries often require admission for IV antibiotics and operative repair.
Le Fort fractures will require control of bleeding and often the airway, use nasal and oral packing as described above. Nasopharyngeal airways and nasotracheal intubation are contraindicated. These patients are usually admitted for antibiotics and surgery.4
Further discussion on Le Fort fractures including diagrams of injury patterns can be found here: http://www.emdocs.net/em3am-le-fort-fractures/” http://www.emdocs.net/em3am-le-fort-fractures/
Mandibular Fracture
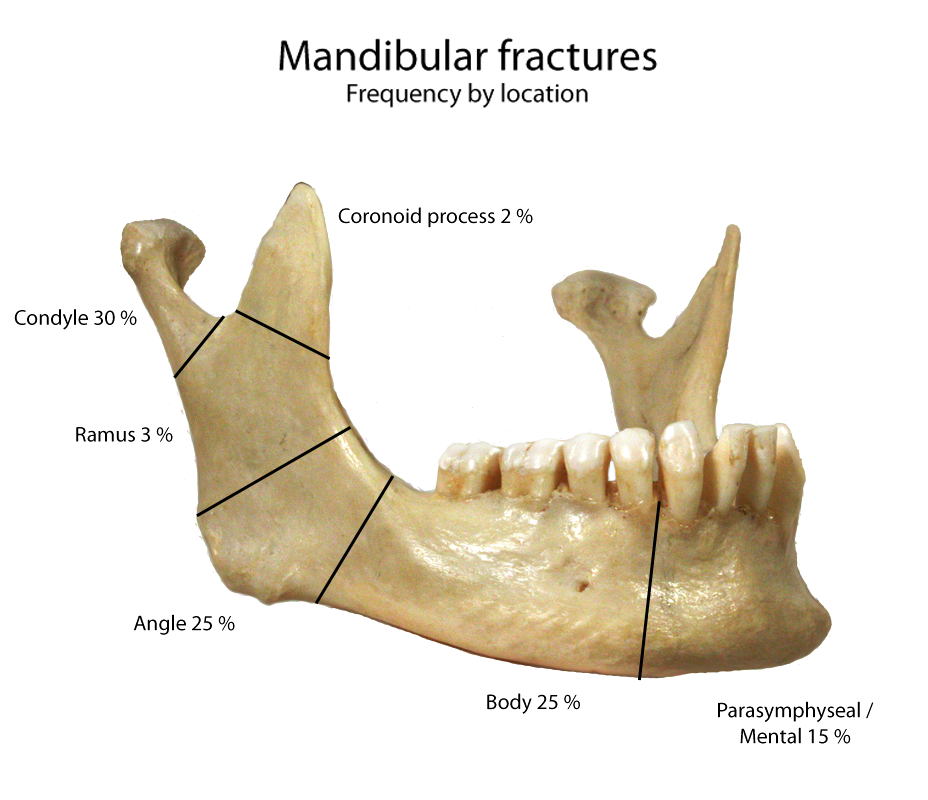
Evaluation – Mandibular fractures are the second most common facial bone fracture. The mandible forms a dynamic ring with the temporomandibular joints (TMJs) bilaterally. Fractures often occur in 2 or more locations, although as many as 63% are single fractures (Figure 3).25,26 Patients should be asked about jaw malocclusion as well as paresthesia to the chin, lip, or teeth. When there is suspicion for a mandibular fracture, a thorough intraoral exam should be performed. Even small breaks in the mucosa should be considered an open fracture. The examination should include evaluation for sublingual hematomas, which may suggest occult fracture or may develop into an airway issue. The TMJs should be palpated and the examiner should inspect for hemotympanum or auditory canal trauma to suggest easy-to-miss condyle fractures.4,27
Figure 3: Frequency of mandibular fractures by anatomic location
The “tongue blade test” is 95% sensitive for fracture. If a patient can break a tongue depressor held between their teeth on both sides without too much discomfort, fracture is unlikely.28,29
Panoramic mandibular radiography (Panorex), in addition to anteroposterior mandible films, is a reasonable test, especially when suspicion is low, although CT is gold standard with sensitivity approaching 100%.4,30,31,32
Management – Physicians should be wary of injuries that may result in airway compromise. If there is no evidence of impending airway compromies, a Barton’s bandage can be used to splint the fracture and provide patient comfort. Antibiotics that cover for oral flora are indicated for open fractures. Penicillin G or clindamycin are recommended.4,33 Most open fractures require admission. Patients with closed fracture can consider discharge with close (<72 hour) facial surgeon follow-up.4,33
Further discussion on mandibular fractures can be found here: http://www.emdocs.net/mandibular-fractures-pearls-and-pitfalls/
Dental Trauma
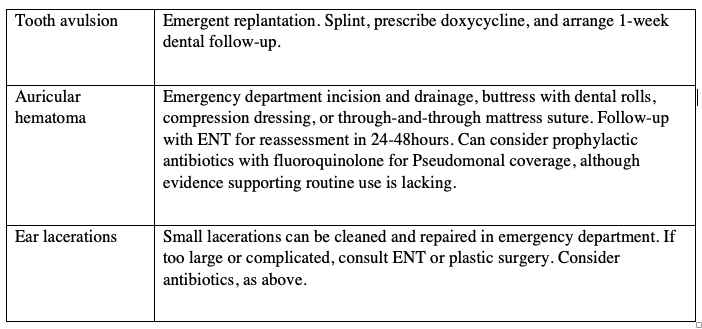
Dental injuries are commonly associated with facial trauma. Assessment of malocclusion and close inspection and percussion of teeth is required for evaluation, with the goal of determining the necessity for close dental follow-up. Cracks in the enamel (infractions) or fractures isolated to the enamel (Ellis class I fractures) do not require urgent dental consultation. If the dentin is involved, this is an Ellis class II fracture, characterized by yellow tissue and sensitivity to air or temperature. These cases require ionomer dental cement application to the exposed dentin and dental evaluation within 24-48 hours. If a pink blush to the dentin (suggesting dentin <0.5mm thick) or if bleeding pulp is seen (Ellis class III), a base of calcium hydroxide should be applied prior to dental cement. Fractures involving the root, alveolar ridge fractures, and luxation injuries require repositioning as well as possible, splinting in the emergency department, and urgent dental evaluation in 24-48 hours. Avulsed teeth should be placed in a physiologic solution (milk, saline, saliva, Hank’s solution) and replanted as soon as possible regardless of dry time, although best prognosis is <60 min dry time. The avulsed tooth should be splinted and patients should receive antibiotic prophylaxis with doxycycline as well as dental follow-up within 1 week.4,34,35
Auricular Injuries
The external ear is an exposed structure and is prone to injury in the setting of head trauma. Auricular hematomas and small lacerations with exposed cartilage are within the scope of emergency physicians, with the goal to minimize risk of ischemia or infection of the cartilage to preserve form and cosmesis of the auricle. Auricular hematomas should be drained by incision and drainage, which is preferred over needle aspiration for its lower risk of recurrence. The area is then buttressed with dental rolls, compression dressing, or through-and-through mattress sutures. Patients should be referred to ENT for revaluation in 24-48 hours.36,37 Ear lacerations less than 2 cm can be considered for primary closure if good approximation of the skin and cartilage can be achieved without too much tension. Larger lacerations or those with difficulty achieving good approximation or coverage of cartilage will need to be referred to ENT or plastics specialist for more advanced techniques. 4-0 or 5-0 absorbable sutures should be used to gently approximate the fragile cartilage, although this is often not necessary if good approximation is achieved with skin sutures.37,38 No evidence supports the use of empiric prophylactic antibiotics in either of the above cases, although it is reasonable to consider prophylactic antibiotics in cases of soiled wounds, exposed cartilage, or immunocompromised patients. Pseudomonal coverage is needed, with ciprofloxacin being the most common oral choice.39
Case Recap
The patient with significant facial trauma was quickly evaluated for other immediate life threats and determined to be suitable for an awake intubation with ketamine. The team was prepared for a surgical airway, but the patient was successfully intubated on the first pass with video laryngoscopy and copious suctioning. Anterior nasal and intraoral packing were used to help control bleeding.
Further examination revealed telecanthus, midface instability, and deformity of the mandible with mucosal tears adjacent to the inferior alveolar ridge. Following CTs of the head and maxillofacial skeleton, the patient was found to have a combination Le Fort I/II fracture, left medial orbital blowout fracture, and comminuted mandibular fracture as well as some areas of hemorrhagic cerebral contusion. Prophylactic antibiotics for open mandibular and sinus fractures was initiated with IV clindamycin. The patient was subsequently admitted to the surgical ICU with neurosurgical and plastic surgery consultations.
Summary/Learning Points
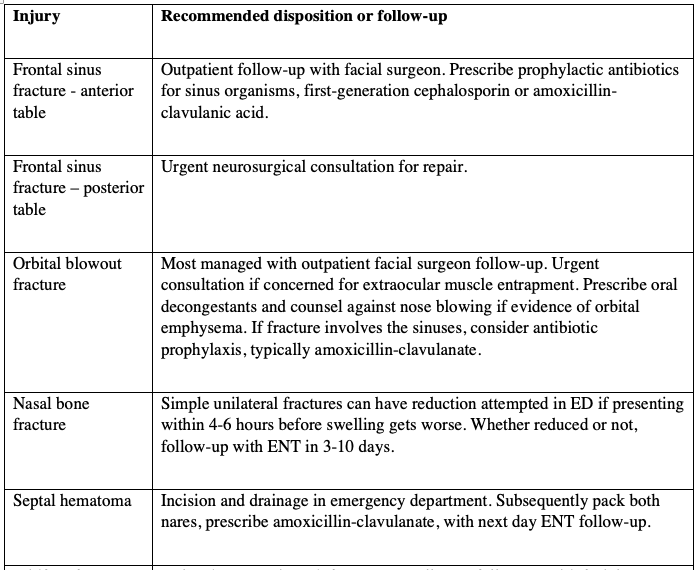
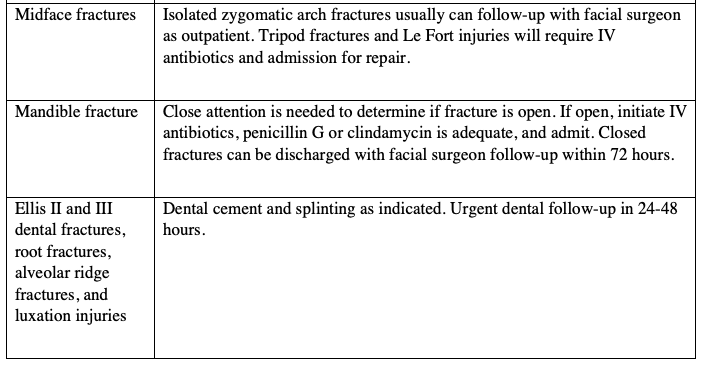
- Table 1 summarizes the recommended disposition and management of patients with maxillofacial injuries.
- Anticipate a difficult airway and try to predict challenges based on injury pattern. Be prepared for cricothyrotomy. Consider awake intubation.
- Anterior nasal, posterior nasal, and intraoral packing are mainstays of hemorrhage control. Use caution when placing anything through the nose to avoid malposition intracranially.
- Facial CT is the imaging modality of choice for the facial skeleton.
- In cases of frontal bone fracture, pay closest attention to the posterior table of the frontal sinus.
- Orbital bone fractures require close inspection for associated injuries to the eye or other orbital structures. Extraocular muscle entrapment warrants urgent consultation.
- Nasal injury requires a good internal exam for septal hematoma.
- Le Fort fractures are high-mechanism injuries; they will usually be admitted for IV antibiotics and surgery.
- Mandibular fractures require a thorough internal exam to rule out open fracture. The tongue blade test is a useful bedside screening tool.
- Open fractures or those with sinus involvement require antibiotic prophylaxis. Amoxicillin-clavulanate is usually a good choice.
Table 1: Summary of common maxillofacial injuries with recommended disposition and follow-up
References / Further Reading
- Alvi A, Doherty T, Lewen G. Facial Fractures and Concomitant Injuries in Trauma Patients. The Laryngoscope. 2003;113(1):102-106. doi:10.1097/00005537-200301000-00019
- Sethi RKV, Kozin ED, Fagenholz PJ, Lee DJ, Shrime MG, Gray ST. Epidemiological Survey of Head and Neck Injuries and Trauma in the United States. Otolaryngology–Head and Neck Surgery. 2014;151(5):776-784. doi:10.1177/0194599814546112
- Stewart RM. ATLS: Advanced Trauma Life Support: Student Course Manual. Chicago: American College of Surgeons; 2018.
- Tintinalli JE. Tintinalli’s Emergency Medicine. New York: McGraw-Hill Medical; 2020.
- Hutchison I, Lawlor M, Skinner D. ABC of major trauma. Major maxillofacial injuries. British Medical Journal. 1990;301(6752):595-599.
- Muzzi DA, Losasso TJ, Cucchiara RF. Complication from a Nasopharyngeal Airway in a Patient with a Basilar Skull Fracture. Anesthesiology. 1991;74(2):366-367. doi:10.1097/00000542-199102000-00026
- Schade K, Borzotta A, Michaels AA. Intracranial Malposition of Nasopharyngeal Airway. The Journal of Trauma: Injury, Infection, and Critical Care. 2000;49(5):967-968. doi:10.1097/00005373-200011000-00032
- Hirabayashi Y, Fujita A, Seo N, Sugimoto H. Cervical spine movement during laryngoscopy using the Airway Scope compared with the Macintosh laryngoscope. Anaesthesia. 2007 Oct;62(10):1050-5. doi: 10.1111/j.1365-2044.2007.05188.x. PMID: 17845658.
- Brown CA, Sakles JC, Mick NW. The Walls Manual of Emergency Airway Management. Philadelphia, PA: Wolters Kluwer; 2018.
- Jose A, Nagori SA, Agarwal B, Bhutia O, Roychoudhury A. Management of maxillofacial trauma in emergency: An update of challenges and controversies. J Emerg Trauma Shock. 2016;9(2):73-80. doi:10.4103/0974-2700.179456
- Myga-Porosiło J, Skrzelewski S, Sraga W, Borowiak H, Jackowska Z, Kluczewska E. CT Imaging of facial trauma. Role of different types of reconstruction. Part I – bones. Pol J Radiol. 2011;76(1):41-51.
- Boyette JR, Pemberton JD, Bonilla-Velez J. Management of orbital fractures: challenges and solutions. Clin Ophthalmol. 2015;9:2127-2137. Published 2015 Nov 17. doi:10.2147/OPTH.S80463
- Marinaro J, Crandall CS, Doezema D. Computed tomography of the head as a screening examination for facial fractures. Am J Emerg Med. 2007 Jul;25(6):616-9. doi: 10.1016/j.ajem.2006.11.029. PMID: 17606084.
- Goh SH, Low BY. Radiologic screening for midfacial fractures: a single 30-degree occipitomental view is enough. J Trauma. 2002 Apr;52(4):688-92. doi: 10.1097/00005373-200204000-00012. PMID: 11956383.
- Truong AQ, O’Brien DC, Strong EB, Dublin A. Lateral pterygoid plate fractures associated with mandible fractures. JAMA Facial Plast Surg. 2014 Nov-Dec;16(6):437-9. doi: 10.1001/jamafacial.2014.645. PMID: 25211530.
- Sutton-Ramsey D. Facial Fractures. Core EM. https://coreem.net/core/facial-fractures/. Published 2018. Accessed December 14, 2020.
- Jeyaraj P. Frontal bone fractures and frontal sinus injuries: Treatment paradigms. Ann Maxillofac Surg. 2019;9(2):261-282. doi:10.4103/ams.ams_151_19
- Vasudev S, Reddy KS. Trigemino-cardiac reflex during orbital floor reconstruction: a case report and review. J Maxillofac Oral Surg. 2015 Mar;14(Suppl 1):32-7. doi: 10.1007/s12663-011-0271-4. Epub 2011 Aug 10. PMID: 25861181; PMCID: PMC4379254.
- Roth FS, Koshy JC, Goldberg JS, Soparkar CN. Pearls of orbital trauma management. Semin Plast Surg. 2010;24(4):398-410. doi:10.1055/s-0030-1269769
- Kucik CJ, Clenney T, Phelan J. Management of acute nasal fractures. Am Fam Physician. 2004 Oct 1;70(7):1315-20. PMID: 15508543.
- Fusetti S, Cornelius C, Gellrich N et al. Closed reduction for Nasal bone. Surgeryreference.aofoundation.org. https://surgeryreference.aofoundation.org/cmf/trauma/midface/nasal-bone/closed-reduction. Published 2020. Accessed December 18, 2020.
- Kelley BP, Downey CR, Stal S. Evaluation and reduction of nasal trauma. Semin Plast Surg. 2010;24(4):339-347. doi:10.1055/s-0030-1269763
- Hasler RM, Exadaktylos AK, Bouamra O, Benneker LM, Clancy M, Sieber R, Zimmermann H, Lecky F. Epidemiology and predictors of cervical spine injury in adult major trauma patients: a multicenter cohort study. J Trauma Acute Care Surg. 2012 Apr;72(4):975-81. doi: 10.1097/TA.0b013e31823f5e8e. PMID: 22491614.
- Phillips BJ, Turco LM. Le Fort Fractures: A Collective Review. Bulletin of Emergency and Trauma. 2017 Oct;5(4):221-230. DOI: 10.18869/acadpub.beat.5.4.499.
- Lee KH. Epidemiology of mandibular fractures in a tertiary trauma centre. Emerg Med J. 2008 Sep;25(9):565-8. doi: 10.1136/emj.2007.055236. PMID: 18723703.
- Escott EJ, Branstetter BF. Incidence and characterization of unifocal mandible fractures on CT. AJNR Am J Neuroradiol. 2008 May;29(5):890-4. doi: 10.3174/ajnr.A0973. Epub 2008 Feb 13. PMID: 18272555.
- Ceallaigh PO, Ekanaykaee K, Beirne CJ, Patton DW. Diagnosis and management of common maxillofacial injuries in the emergency department. Part 2: mandibular fractures. Emerg Med J. 2006;23(12):927-928. doi:10.1136/emj.2006.035956
- Alonso LL, Purcell TB. Accuracy of the tongue blade test in patients with suspected mandibular fracture. J Emerg Med. 1995 May-Jun;13(3):297-304. doi: 10.1016/0736-4679(95)00006-v. PMID: 7673618.
- Lin M. Trick of the Trade: A tongue blade is as mighty as an xray. ALiEM. https://www.aliem.com/trick-of-trade-tongue-blade-is-as/. Published 2010. Accessed December 19, 2020.
- Nair, M.K. and Nair, U.P. (2001), Imaging of Mandibular Trauma: ROC Analysis. Academic Emergency Medicine, 8: 689-695. https://doi.org/10.1111/j.1553-2712.2001.tb00186.x
- Roth FS, Kokoska MS, Awwad EE, Martin DS, Olson GT, Hollier LH, Hollenbeak CS. The identification of mandible fractures by helical computed tomography and panorex tomography. J Craniofac Surg. 2005 May;16(3):394-9. doi: 10.1097/01.scs.0000171964.01616.a8. PMID: 15915103.
- Wilson IF, Lokeh A, Benjamin CI, Hilger PA, Hamlar DD, Ondrey FG, Tashjian JH, Thomas W, Schubert W. Prospective comparison of panoramic tomography (zonography) and helical computed tomography in the diagnosis and operative management of mandibular fractures. Plast Reconstr Surg. 2001 May;107(6):1369-75. doi: 10.1097/00006534-200105000-00008. PMID: 11335803.
- Murray JM. Mandible fractures and dental trauma. Emerg Med Clin North Am. 2013 May;31(2):553-73. doi: 10.1016/j.emc.2013.02.002. PMID: 23601489.
- DiAngelis, A.J., Andreasen, J.O., Ebeleseder, K.A., Kenny, D.J., Trope, M., Sigurdsson, A., Andersson, L., Bourguignon, C., Flores, M.T., Hicks, M.L., Lenzi, A.R., Malmgren, B., Moule, A.J., Pohl, Y. and Tsukiboshi, M. (2012), International Association of Dental Traumatology guidelines for the management of traumatic dental injuries: 1. Fractures and luxations of permanent teeth. Dental Traumatology, 28: 2-12. https://doi.org/10.1111/j.1600-9657.2011.01103.x
- Andersson, L., Andreasen, J.O., Day, P., Heithersay, G., Trope, M., DiAngelis, A.J., Kenny, D.J., Sigurdsson, A., Bourguignon, C., Flores, M.T., Hicks, M.L., Lenzi, A.R., Malmgren, B., Moule, A.J. and Tsukiboshi, M. (2012), International Association of Dental Traumatology guidelines for the management of traumatic dental injuries: 2. Avulsion of permanent teeth. Dental Traumatology, 28: 88-96. https://doi.org/10.1111/j.1600-9657.2012.01125.x
- Eagles, K., Fralich, L. and Stevenson, J., 2013. Ear Trauma. Clinics in Sports Medicine, 32(2), pp.303-316.
- Roy, S. and Smith, L., 2010. A novel technique for treating auricular hematomas in mixed martial artists (ultimate fighters). American Journal of Otolaryngology, 31(1), pp.21-24.
- Falcon-Chevere, J., Giraldez, L., Rivera-Rivera, J. and Suero-Salvador, T., 2013. Critical ENT Skills and Procedures in the Emergency Department. Emergency Medicine Clinics of North America, 31(1), pp.29-58.
- Emergency Medicine Journal, 2012. BET 2: No evidence for prophylactic antibiotics in pinna laceration. 29(9), pp.777.1-777.




