
Here’s another case from Medical Malpractice Insights – Learning from Lawsuits, a monthly email newsletter for ED physicians. The goal of MMI-LFL is to improve patient safety, educate physicians, and reduce the cost and stress of medical malpractice lawsuits. To opt in to the free subscriber list, click here.
Chuck Pilcher, MD, FACEP
Editor, Med Mal Insights
Mesenteric ischemia: An overlooked cause of abdominal pain
6 months of abdominal pain and weight loss
Facts: A 49-year-old married mother of 2 sees her PCP for recurrent bouts of post-prandial abdominal pain, occasional vomiting, and diarrhea. She is referred to a gastroenterologist who orders an upper GI series and does both a UGI endoscopy and a colonoscopy, interpreting them as normal. (Later review by others note that the studies are consistent with the possibility of mesenteric ischemia.) The patient’s pain continues, sometimes leaving her writhing on the floor, and is unrelieved by opioids. Her weight  drops 35% to 65 pounds. She is seen in the ED 3 times over a 6 month period for abdominal pain and weight loss. Another gastroenterologist on-call for her GI doc sees her 3 times during that period and suggests the correct diagnosis of recurrent chronic bowel ischemia. The primary gastroenterologist, PCP, and an endocrinologist disregard that opinion. On the final admission, the covering gastroenterologist and the surgeon he consults prevail. A mesenteric angiogram is ordered and the diagnosis confirmed, but the entire bowel is now infarcted. After several surgeries, the patient expires 3 months later. An attorney is consulted and a lawsuit filed.
drops 35% to 65 pounds. She is seen in the ED 3 times over a 6 month period for abdominal pain and weight loss. Another gastroenterologist on-call for her GI doc sees her 3 times during that period and suggests the correct diagnosis of recurrent chronic bowel ischemia. The primary gastroenterologist, PCP, and an endocrinologist disregard that opinion. On the final admission, the covering gastroenterologist and the surgeon he consults prevail. A mesenteric angiogram is ordered and the diagnosis confirmed, but the entire bowel is now infarcted. After several surgeries, the patient expires 3 months later. An attorney is consulted and a lawsuit filed.
Plaintiff: My PCP, gastroenterologist, and endocrinologist all ignored my symptoms and didn’t listen to the one GI doc who knew what was going on. If any of you had paid attention, listened to my complaints – the pain, the post-prandial vomiting and diarrhea, the weight loss – and thought of the possibility of mesenteric ischemia, then done the right test earlier, I would be alive today. You were so sure of yourselves that you didn’t listen.
Defense: We considered mesenteric ischemia but didn’t think the likelihood was high enough to get the angiogram earlier. You had other issues going on.
Result: The covering gastroenterologist was dismissed from the suit and a “substantial” pre-trial settlement was reached with the other defendants.
Takeaways:
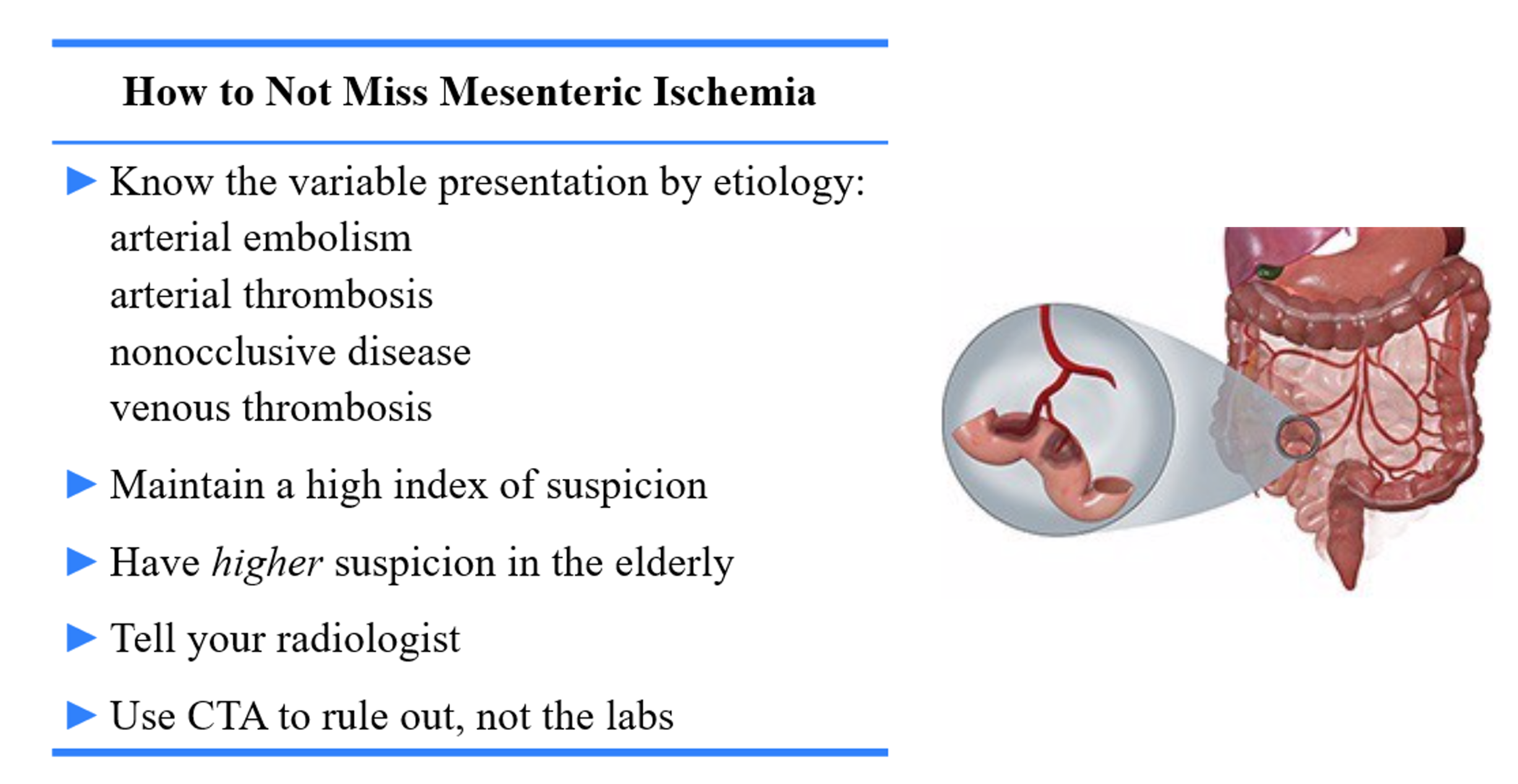
- A mesenteric infarct is most often an acute presentation, but like heart disease it can present with “angina” as well as an acute MI.
- Keep in mind the various types and how they present (see tables below).
- Chronic mesenteric ischemia is unusual but must be considered in patients with episodic abdominal pain, especially post-prandial.
- Sudden onset abdominal pain in anyone over 50 should suggest mesenteric infarct, among other diagnoses (e.g., volvulus).
- If confirmed, stenting or bypass can be performed.
For a great take on improving the ED diagnosis of mesenteric ischemia, please see this emDocs post, as well as this EM@3AM post.

References:
- Alrayes A. Chronic Mesenteric Ischemia. Medscape eMedicine. Updated Oct 29, 2019. https://emedicine.medscape.com/article/183683-overview
- Dang C. Acute Mesenteric Ischemia. Medscape eMedicine. Updated Mar 26, 2020. https://emedicine.medscape.com/article/189146-overview




