
Author: David Cisewski, MD (@PainProfiles – EM Resident Physician, Icahn School of Medicine at Mount Sinai) // Edited by: Manpreet Singh, MD (@MPrizzleER), Alex Koyfman, MD (@EMHighAK), and Brit Long, MD (@long_brit)
Welcome back to the Pain Profiles series from David Cisewski. Today we look at a component of the “headache cocktail” – steroids… Do they make a difference, and what steroid, if any, should we use?
During a previous discussion on optimizing treatment for migraines, one of the more contentious subjects was the inclusion of IV dexamethasone in the migraine treatment regimen. There has been a mixed debate over the last two decades as to the efficacy of corticosteroid use for migraine headaches in the emergency setting – some say yes, some say no, most say ‘I don’t know’. In light of new research published this month covering this exact question, this article serves as a refresher on where we stand in the ED for dexamethasone in the migraine treatment plan.
Starting from scratch – why do we use steroids during migraine headache presentations in the ED?
Steroids during acute migraine attacks have been classically used to prevent headache recurrence. Estimates have reported that up to two-thirds of patients with migraine resolution during an ED visit will have a recurrent headache within 48 to 72 hours post-discharge (1). Not only is this a strain on hospital resources when patients bounce back to the ED, these recurrences are incredibly debilitating to the quality of life of patients suffering such frequent attacks (2).
What is the hypothesized mechanism behind dexamethasone and migraine prevention?
One of the presumed causes of migraines is a state of neurogenic inflammation (3). Corticosteroids such as dexamethasone could mitigate this inflammatory response, thereby decreasing pain and recurrence of migraines.
What data do we have to support dexamethasone use for migraine treatment in the ED setting?
A 2008 meta-analysis (Colman, 2008) including the results of 7 randomized trials assessing dexamethasone for migraine recurrence reduction found a number-needed-to-treat (NNT) = 9 to prevent recurrence within 72 hours (3).
A separate meta-analysis on the same subject, also published in 2008 (Singh, 2008), including the results of 7 randomized trials found a NNT = 10 (4). Not surprising these two studies came to approximately the same conclusion as 6 of the 7 studies included in each meta-analysis were the same (see below).
And finally, a third meta-analysis on the same subject published in 2013 (Huang, 2013), including the results of 8 randomized trials found a NNT = 8 for parenteral dexamethasone, and a NNT=10 for either parenteral or oral dexamethasone (5). The authors of this study noted that Baden, 2006 was not included in their meta-analysis as the study allowed for ‘benign headache’ which may have brought in a large proportion of patients without migraines into the study. [See Table 1 for a comparison of the 3 separate meta-analysis].

What are the current recommended guidelines for dexamethasone use in the ED?
10 mg IV/IM dexamethasone have been the generally accepted standard in combination with traditional migraine headache abortive therapy (e.g. 10 mg IV metoclopramide) to prevent headache recurrence in the week following discharge.
Where did we get 10 mg IV from?
The optimal dose of corticosteroids is still unknown. The choice of 10 mg appears to be an approximation based on the most commonly used dose from the prior meta-analyses (3-5). The doses used in the 9 separate trials ranged from 4 to 24 mg IV, IM, or PO dexamethasone. As noted in the meta-analysis by Huang, 2013, a stronger treatment effect appears among those that received >15 mg dexamethasone (RR=0.58; 95% CI 0.42–0.80) (5). Of the studies included in the meta-analyses, 24 mg IV dexamethasone showed the most significant reduction to headache recurrence (Innes, 1999: 48-72 hr headache recurrence – dexamethasone patients (18%) versus placebo (45%) (odds ratio 0.28; 95% CI 0.11-0.69; p = 0 .005)) (6).
So perhaps 24 mg IV dexamethasone should be the optimal dose?
Uncertain. A separate study conducted by Donaldson, et al (2008) looked at just this question; a total of 115 patients with migraine exacerbation were randomized to receive either 24 mg IV dexamethasone or placebo (7). The results showed a non-statistical trend toward dexamethasone in 72-hour headache recurrence after ED discharge (37% – dexamethasone group; 43% – placebo) but not nearly as promising as previously shown.
What about oral dexamethasone?
Research has also been conducted on the use of 8 mg oral dexamethasone as an adjunct to IV phenothiazine (eg, chlorpromazine) for the prevention of migraine recurrence(8). The headache recurrence rate was 39% in the placebo group (12/31) versus 27% in the dexamethasone group (8/30) (95% CI 0.33-1.45). Whether it was the use of oral versus IV, the smaller dose, or the use of IV phenothiazine (chlorpromazine) as the abortive therapy, the results concluded that a single dose of oral dexamethasone following treatment for migraine in the ED did not reduce the rate of recurrent headaches.
What are the side effects I should consider when deciding whether to administer dexamethasone?
Side effects include restlessness, drowsiness, dizziness, mood changes, nausea/vomiting, numbness/tingling, flushing, and pain at the injection site (3, 4). Fortunately, these side effects have been found to be infrequent, mild, and transient (3, 4). Patients receiving dexamethasone trended toward an increased risk of dizziness versus placebo, which should be discussed with the patient (RR 2.15, 95% CI 0.98-4.74) (3).
Half a decade has passed since the last meta-analyses… any new research on corticosteroids for migraines?
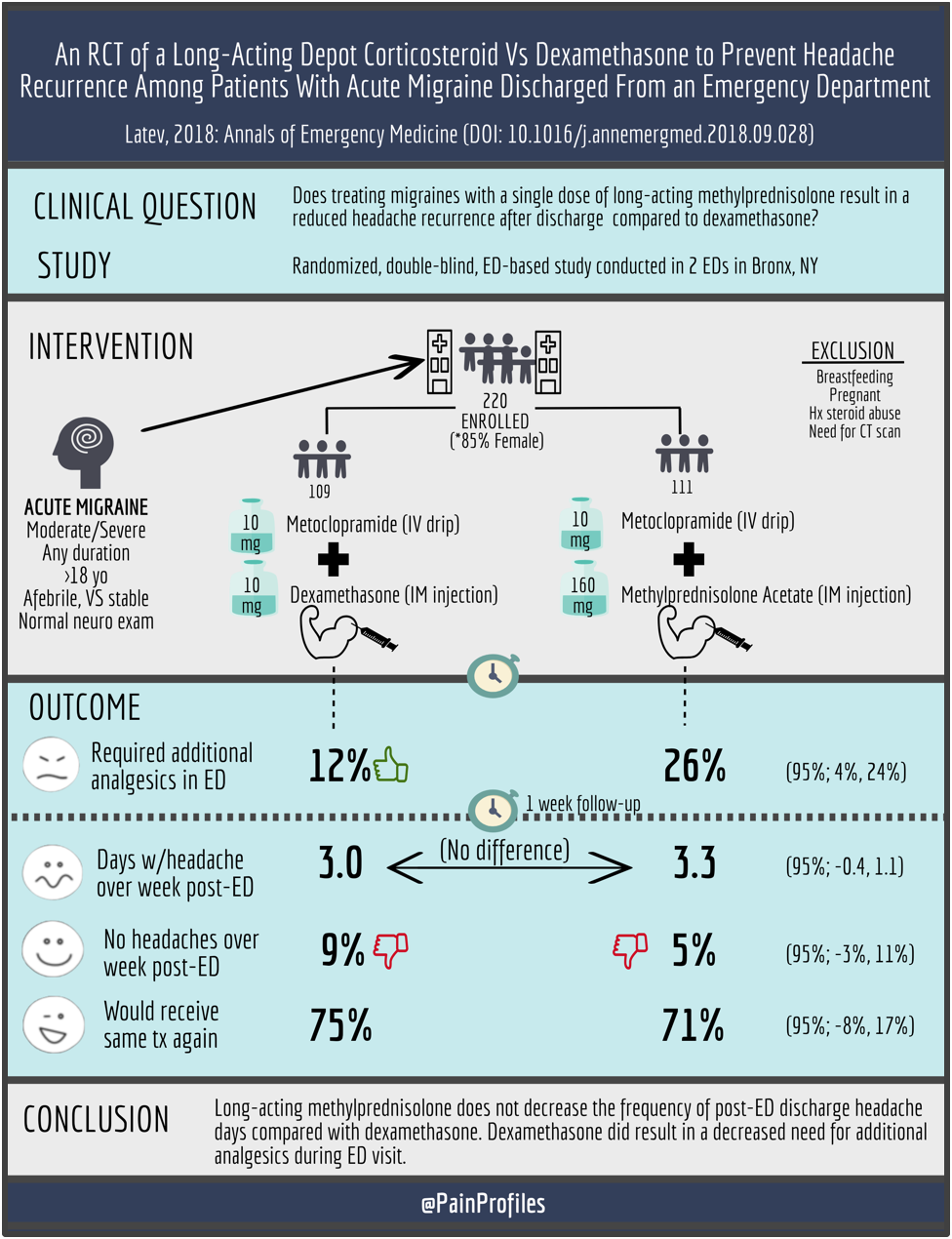
This brings us to the point of this article… Latev, et al recently published research investigating the effectiveness of methylprednisolone acetate in comparison to dexamethasone to see whether a long-acting steroid could decrease the number of days of headache recurrence following ED discharge (9). The hypothesis being that if short-acting dexamethasone decreases headache recurrence, perhaps a longer-acting corticosteroid will provide more headache-free days.

Interestingly, this research was conducted by many of the same members of the research team who previously found no decreased headache recurrence over placebo and concluded IV dexamethasone should not be administered routinely for the emergency department-based treatment of acute migraine (although it might be useful for patients with migraine lasting longer than 72 hours) (10).
What were the specifics of this study?
This was a randomized, blinded clinical control trial based out of Bronx, NY using two high-volume ED’s (Jacobi Hospital, Montefiore Hospital). Population: patients older than 18 years old presenting with a migraine headache of moderate to severe intensity (not limited by duration) without signs or secondary headaches, not currently on steroids, and not pregnant or breastfeeding were included in the study. Of 1,292 patients screened, 220 were included in the study. Intervention/Comparison: patients were randomized to receive 10 mg IV metoclopramide and either 10 mg IM dexamethasone or 160 mg methylprednisolone. Primary outcome was number of days with headache over the 7 days following ED discharge. Secondary outcomes included complete headache freedom, number adverse events, and percentage of patients who would receive the same medication again.
How were the corticosteroid doses chosen?
As mentioned, 10 mg IM dexamethasone is the most commonly used dose based on a prior meta-analyses (3-5). As no prior research has been conducted using methylprednisolone acetate, 160 mg IM was chosen as an above-average dose (average range 40-120 mg) that could ensure researchers were able to capture therapeutic benefit if one existed.
What did the results of this study show?
There was no significant difference in headache recurrence between dexamethasone and methylprednisolone (3.0 days vs 3.3 days with headache during week following ED visit; 95% CI -0.4 to 1.1). Complete headache freedom was only achieved in 9% of patients receiving dexamethasone and 5% of patients receiving methylprednisolone (95% CI -3% to 11%). Approximately three-fourths of patients said they would receive the same medication again (75% for dexamethasone, 71% methylprednisolone; 95% CI -8%, 17%). Both groups experienced a similar incidence of side effects (17% for dexamethasone, 25% methylprednisolone; 95% CI -2% to 19%) while the methylprednisolone resulted in a higher incidence of pain with injection (presumably because of higher volume).
Worth noting, only 12% of patients in this dexamethasone-metoclopramide group required rescue analgesics which is much lower than the 30 to 38% requirement previously reported from this institution receiving metoclopramide alone, suggesting dexamethasone may serve as an adjunct analgesic for short-term relief (11).
The Upshot
Though rapid relief of migraines may be the primary object of the emergency doc, headache recurrence continues to be a very important outcome for migraneurs (2). Unfortunately, long-acting corticosteroids weren’t the answer we were hoping for. Is dexamethasone effective? Yes. Is it really effective? No. Should we be using it? Judgement call. A big takeaway from these results were that only 5-10% of patients experienced complete headache freedom at discharge. This leaves a lot of room for improvement and the hope that future research will continue the search for an improved therapeutic modality. Until then, continued headaches following discharge are highly likely and patients should be counseled on this unfortunate reality. Use of dexamethasone following a shared decision with the patient including the possible benefit (1 in 9) weighed against the side effect is advised. Based on the results of this most recent study, I will now be giving dexamethasone and metoclopramide together at migraine treatment initiation with the thought that I have about a 10% chance of decreasing headache recurrence, but may also be reducing the need for repeat analgesia during the current ED visit.
Summary Points:
- 10mg IV/IM dexamethasone can be used to reduce migraine recurrence (NNT = 9-10).
- The optimal dose of dexamethasone is unknown; may be a trend toward higher doses.
- Oral and long-term IM corticosteroids (methylprednisolone) do not appear as efficacious as IV/IM dexamethasone at preventing migraine headache recurrence.
- If you decide to give dexamethasone, give at arrival, not discharge: IV/IM dexamethasone may offer short-term benefit by reducing need for repeat (rescue) analgesics.
Further Reading:
- emDocs – Pain Profiles: ED Migraine Management – The New Kid on the “Block”
- emDocs Cases – Headache Management in the ED
- Ben Friedman, Annals of Emergency Medicine –Managing Migraine
- Orr, 2016 – Management of Adults With Acute Migraine in the Emergency Department: The American Headache Society Evidence Assessment of Parenteral Pharmacotherapies
- Ben Friedman, MD on headache management from painandpsa.orgEmergency Department Management of Acute Headache
For EMA fans out there (and Hoffman Disciples like myself) I also recommend the following two discussions on these meta-analysis reviews where Hoffman does a deep-dive into power and statistical/clinical significance and how we should use that to interpret this data. It’s fascinating to hear the thoughts of physicians who have seen this topic evolve over the last 20 years.

References:
[1] Friedman BW, Hochberg ML, Esses D, et al. Recurrence of primary headache disorders after emergency department discharge: frequency and predictors of poor pain and functional outcomes. Ann Emerg Med. 2008;52:696-704.
[2] Lipton RB, Hamelsky SW, Dayno JM. What do patients with migraine want from acute migraine treatment? Headache. 2002;42 Suppl 1:3-9.
[3] Colman I, Friedman BW, Brown MD, et al. Parenteral dexamethasone for acute severe migraine headache: meta-analysis of randomised controlled trials for preventing recurrence. BMJ. 2008;336:1359-61.
[4] Singh A, Alter HJ, Zaia B. Does the addition of dexamethasone to standard therapy for acute migraine headache decrease the incidence of recurrent headache for patients treated in the emergency department? A meta-analysis and systematic review of the literature. Acad Emerg Med. 2008;15:1223-33.
[5] Huang Y, Cai X, Song X, et al. Steroids for preventing recurrence of acute severe migraine headaches: a meta-analysis. Eur J Neurol. 2013;20:1184-90.
[6] Innes GD, Macphail I, Dillon EC, Metcalfe C, Gao M. Dexamethasone prevents relapse after emergency department treatment of acute migraine: a randomized clinical trial. CJEM. 1999;1:26-33.
[7] Donaldson D, Sundermann R, Jackson R, Bastani A. Intravenous dexamethasone vs placebo as adjunctive therapy to reduce the recurrence rate of acute migraine headaches: a multicenter, double-blinded, placebo-controlled randomized clinical trial. Am J Emerg Med. 2008;26:124-30.
[8] Kelly AM, Kerr D, Clooney M. Impact of oral dexamethasone versus placebo after ED treatment of migraine with phenothiazines on the rate of recurrent headache: a randomised controlled trial. Emerg Med J. 2008;25:26-9.
[9] Latev A, Friedman BW, Irizarry E, et al. A Randomized Trial of a Long-Acting Depot Corticosteroid Versus Dexamethasone to Prevent Headache Recurrence Among Patients With Acute Migraine Who Are Discharged From an Emergency Department. Ann Emerg Med. 2018.
[10] Friedman BW, Greenwald P, Bania TC, et al. Randomized trial of IV dexamethasone for acute migraine in the emergency department. Neurology. 2007;69:2038-44.
[11] Friedman BW, Cabral L, Adewunmi V, et al. Diphenhydramine as Adjuvant Therapy for Acute Migraine: An Emergency Department-Based Randomized Clinical Trial. Ann Emerg Med. 2016;67:32-9 e3.





