Author: Brit Long, MD (@long_brit, EM Chief Resident at SAUSHEC, USAF) // Edited by: Jennifer Robertson, MD and Alex Koyfman, MD (@EMHighAK, EM Attending Physician, UTSW / Parkland Memorial Hospital)
The diagnosis of pyelonephritis is not always straightforward and there are many mimics of this condition. This article will evaluate why diagnosing simple vs. complicated pyelonephritis matters. In addition, the diagnosis and management of complicated pyelonephritis and the mimics of pyelonephritis will also be discussed.
CASE:
A 45 year-old female presents with a two day history of dysuria, fevers, suprapubic discomfort, and right flank pain. She tells you that her symptoms are similar to a prior urinary tract infection (UTI) with the exception of the fever. Your assessment reveals a febrile female with positive right-sided costovertebral angle (CVA) tenderness, but the rest of the exam is normal. The patient’s urinalysis is positive for leukocyte esterase (LE), nitrites, white blood cells (WBC) and bacteria. Her serum WBC is elevated at 22,000, but her renal function, electrolytes, and lactic acid levels are normal.
Background
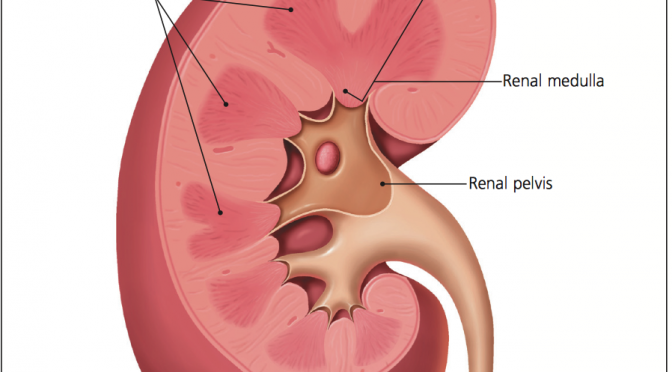
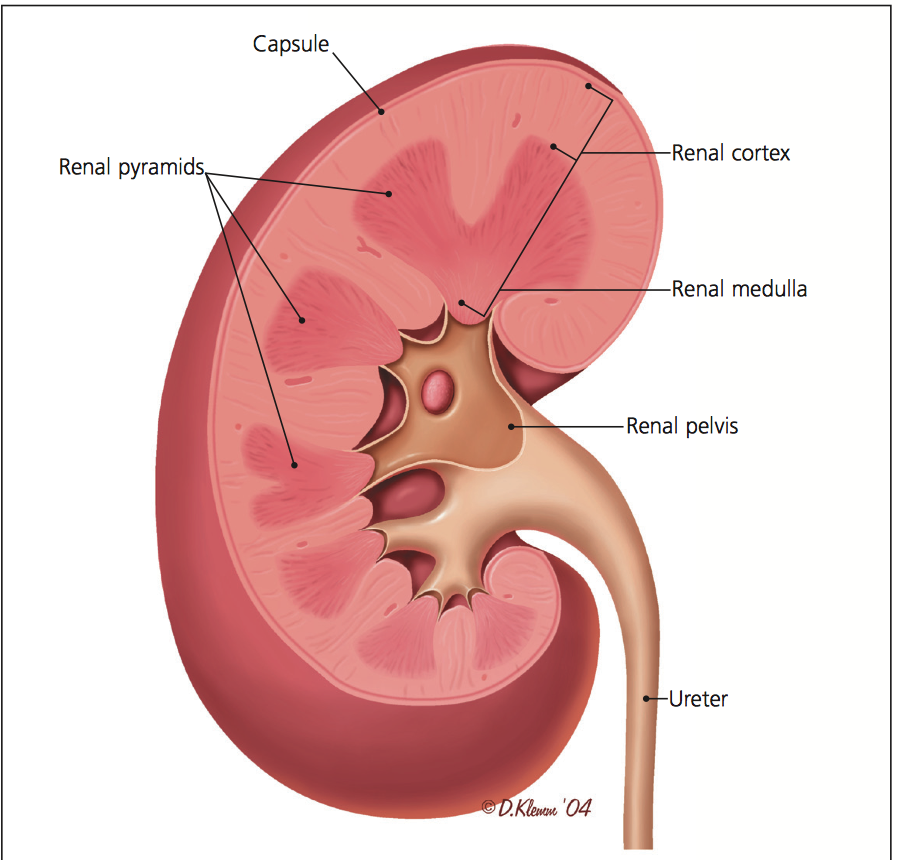
Pyelonephritis is an infection of the renal parenchyma, calyces, and/or pelvis. Acute infection is most commonly caused by enteric organisms that ascend from a lower urinary tract infection or hematogenous spread. In an ascending infection, microbes colonize the lower urogenital tract and reach the kidneys via the bladder and ureters. Over 250,000 cases of pyelonephritis are diagnosed per year. Overall, females (15/10,000) are affected more than males (3/10,000), but elderly female and male patients are more equally affected. Females experience three peaks of life where they may be more affected by pyelonephritis. These peaks include ages 0-4 years, 15-35 years, and greater than 80 years. Males experience two main peaks where they may be more affected and this includes ages 0-4 years and greater than 80 years of age.1-3
The vast majority of genitourinary (GU) tract infections can be thought of as a spectrum ranging from simple, uncomplicated UTI to sepsis with shock from abscess/complicated infection.2
Renal Anatomy
Pathogens
The most common pathogens that cause urinary tract infections are enteric microbes but mainly E. coli (which accounts for 70-95% of simple cases). Other common organisms include Staph saprophyticus, Klebsiella pneuomoniae, Proteus mirabilis, Enterococci, Staph aureus (S. aureus), and Enterobacter. The E. coli bacterium is particularly dominant because it possesses several elements that increase host infection, such as flagella (increased motility), hemolysin proteins to break down red blood cells (RBC), fimbriae and adhesins that increase attachment to epithelial surfaces, and molecules that scavenge free iron (called siderophores).3 It should be noted that the elderly are more commonly infected with agents other than E. coli. This is due to the physiologic differences between the elderly and the young, as the elderly tend to get UTIs secondary to urinary retention and instruments such as catheters.2-5
Hematogenous spread to the kidneys resulting in pyelonephritis is most commonly due to S. aureus. If suspicious of a hematogenous origin, consider endocarditis, epidural abscess, IV drug abuse, or another source that is causing the infection. Hematogenous spread of gram negative organisms is much less likely unless an obstruction such as a kidney stone is present in the urinary tract. Skin infections due to S. aureus or fungi can also lead to pyelonephritis.2,3
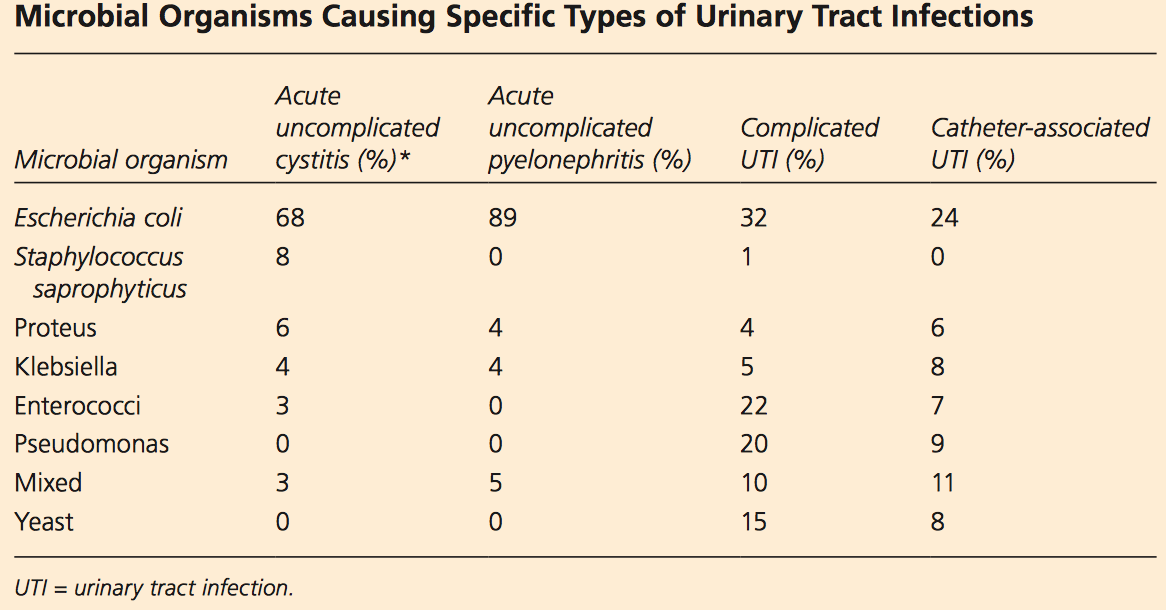
Table 1 – Most common causes of UTI by species
Simple vs. Complicated Infection
Why does this matter? Simple versus complicated pyelonephritis infections have different treatment plans and even different prognoses. Simple infections require shorter antibiotic courses and are associated with improved outcomes, while complicated infections require longer treatment courses and have higher morbidity and mortality.2,3
Complicated pyelonephritis is an infection of the upper urinary tract in the following populations: infants, patients older than 60 years, patients with anatomical abnormalities (single kidney, polycystic kidney disease, vesicoureteral reflux, renal stone, urinary/ureteral/nephrostomy catheter presence), those with impaired renal function, the immunocompromised (diabetes, sickle cell, transplantation, cancer, chemotherapy, HIV, chronic steroid use), males, pregnant patients, or those with a known obstruction (BPH, renal stone, foreign body, neurogenic bladder). As you can see, the list is quite extensive, but this can be broken down into a simple manner:2,3
Think of a simple pyelonephritis infection as any non-pregnant, non-immunosuppressed female of reproductive age with normal renal function pre-infection. Anyone else should be considered complicated. 2,3
Keys to diagnosis using history and exam
Acute pyelonephritis and UTI have a wide spectrum of presentations, from mild symptoms to septic shock. What physical exam and history findings help diagnose UTI/pyelonephritis?
For pyelonephritis, a UTI in the prior year has an odds ratio (OR) of 4.4. If a UTI was present in the last 30 days, the OR increases to 12.5. For women, sexual intercourse greater than 3 times per week in the last 30 days has an OR of 5.6. Diabetes and stress incontinence are also a risk factors.5 In 2010, a study by Giesen et al evaluated 3,711 patients with urinary tract infections. The authors found dysuria to have a + likelihood ratio (LR) of 1.3, frequency to have a +LR of 1.10, hematuria a +LR of 1.72, nocturia a +LR of 1.30, and urgency a +LR of 1.22. The occurrence of an infection increased to greater than 93% with the presence of over 100 colony forming units (CFU)/ml and positive nitrites on urine testing.6 A Journal of the American Medical Association (JAMA) article in 2002 found dysuria to have a +LR of 1.5, hematuria a +LR of 2.0, back pain a +LR of 1.6, and CVA tenderness a +LR of 1.7. The combination of dysuria and frequency with no vaginal irritation or discharge had a +LR of 24.6.7 A study from Family Practice found similar likelihood ratios as the prior studies.8 One study in Academic Emergency Medicine found that history and physical findings were not sufficient to alter the pretest probability of UTI. A urinalysis negative for LE and blood were useful for ruling out infection, while pyuria > 50 CFU/ml and moderate bacteriuria had a +LR of 6.4 and 15.0, respectively.9
Structural abnormalities provide a shelter for bacteria and allow biofilm formation. These structural abnormalities may include renal stones, catheters, polycystic kidney disease, and enlarged prostates. Immunosuppression and chronic steroid use decreases the cytokine and inflammatory response to bacteria in the urogenital system, which also increases risk. Pregnancy is also a key risk factor, as an enlarged uterus can compress the ureters and bladder.2,3,10
Evaluate patients closely for the above risk factors and examine for fever, chills, flank/abdominal pain, and urinary symptoms including urgency, frequency, and dysuria. If the triad of fever, flank pain, and nausea/vomiting is present, strongly consider pyelonephritis. Fever is found in up to 77% of patients with pyelonephritis, but patients with over the age of 65 and those with immunosuppression and/or renal failure may present afebrile. Though nausea and vomiting is common, it is non-specific. In 86% of patients, flank pain or CVA tenderness is found.2,3,10
As in many other conditions, the diagnosis of pyelonephritis is not straightforward in the young and elderly. Infants may only demonstrate decreased feeding or fever with fussiness, while the elderly may only demonstrate altered mental status and/or fever. Up to 33% of elderly patients will have no fever, and 20% will have GI or pulmonary symptoms.2,3,10
Urine Testing
Any suspicion of pyelonephritis warrants a urinalysis and a urine culture. The culture will confirm the diagnosis. Along with the appropriate symptoms, the presence of 10,000 colony forming units (CFU) per mm3 in the urinalysis is required to make the diagnosis. Do not rely on appearance or odor of the urine specimen, as these are unreliable.
The dipstick leukocyte esterase (LE) is usually positive and greater than +1. The LE test requires 60 seconds of urine exposure to register as positive. Dipstick LE has a sensitivity ranging from 72% to 97% and specificity of 41% to 86%. The presence of nitrites suggests urine infection, as greater than 10,000 bacteria per ml of urine are required for conversion of the normal urine nitrates to the abnormal presence of nitrites. The sensitivity of the nitrite test ranges from 19% to 48% and specificity 92% to 100%. Hematuria may be present in pyelonephritis (dipstick of >+1 blood has a sensitivity of 68% to 92%, but low specificity of 46%). Proteinuria of > +3 has a sensitivity of up to 83%, with a specificity up to 53%. Urine cultures should be obtained and will be positive in 90%. With associated symptoms, the presence of WBC casts on urinalysis is specific for pyelonephritis. These WBC casts point to direct renal involvement. 2,5,10,11
What about completely ruling out UTI or pyelonephritis with a negative dipstick in a patient with urinary symptoms? Two studies (one a prospective observational study12 and the other a meta-analysis7) evaluated this question. The meta-analysis found that patients with UTI symptoms had confirmed UTI 50% of the time. When combined with a clear, convincing history, this increased the true positive rate of 90%, which was confirmed by urine culture. However, urine dipstick showed sensitivities as low as 75%, which is not acceptable if the patient has symptoms.7,11,12
Management
Sepsis due to infection of the urinary tract accounts for 25% of all sepsis cases. Mortality can reach 40% if not adequately treated. Complicated UTI and pyelonephritis are the most common causes of urosepsis. The classic UTI and pyelonephritis signs and symptoms may not be present, as only one-third of these patients present with fever, chills, and hypotension. Management should focus on early diagnosis, early resuscitation, early antibiotic administration and identifying and controlling any complicating factors. If the patient is in septic shock, immunosuppressed, or pregnant, obtain blood cultures (positive in 20%-40% of cases).13-15 Avoid blood cultures in simple or complicated pyelonephritis and in patients not in severe sepsis or septic shock, as it is controversial whether blood cultures change clinical course in these populations.16,17 Patients with sepsis from pyelonephritis should have complete blood count (CBC), lactate, and renal function panel obtained, followed with resuscitation and antibiotics. If the patient is hemodynamically stable and tolerating oral fluids, encourage oral fluids and antibiotics.
Pyelonephritis may have serum WBC greater than 20,000 per mL. Other diseases such as severe pneumonia, mesenteric ischemia, bowel perforation, pancreatitis, necrotizing fasciitis, lymphoma/leukemia, and meningitis can also drastically elevate serum WBC levels, so always consider these conditions if a severely elevated WBC count is discovered.
Imaging is often not required in the initial stage of management in simple pyelonephritis. However, with the availability of ultrasound (US), an argument can be made for a quick bedside US exam of the kidneys, bladder, and aorta. If the patient is not responding to treatment within 72 hours or in the setting of complicated pyelonephritis, strongly consider imaging (US or CT) to evaluate for hydronephrosis, abscess, or cyst presence. This can drastically change management and requires urology consultation. 2,3,14,15 One study found that abnormal US or computed tomography (CT) results diverted patients to surgical intervention in 34.3% of cases. Emergency department (ED) use of US found significant abnormalities in 61% of patients with complicated pyelonephritis.18 Factors contributing to abnormal results included male gender, the elderly, prior renal disease, catheter use, prior renal stones, diabetes.
Disposition
The disposition of each patient will center on clinical course and patient comorbidities. If a patient with complicated pyelonephritis also has associated hypotension, peroral (PO) intolerance, dehydration, multiple comorbidities, a single kidney, immunosuppression, an obstructing stone, is pregnant, or has severe sepsis/septic shock, then he or she should be admitted and a urology consultation should be obtained.2,3 If the patient is hemodynamically stable, is PO tolerant, and is otherwise healthy with few comorbidities, then he or she can be safely discharged home with follow up and oral antibiotics.
Antibiotics
Antibiotics are not only the cornerstones of treatment, but they also prevent disease progression. For all antibiotic treatment regimens, consult the local antibiogram and local resistance patterns. In mild simple pyelonephritis, oral fluoroquinolones are first line for 7 to 14 days per the Infectious Diseases Society of America (IDSA). Patients with simple, uncomplicated pyelonephritis should be treated for 7 days. Treatment courses for less than 5 days are associated with relapses in 50% of cases. In the setting of high resistance to fluoroquinolones, provide a one-time dose of ceftriaxone 1g IV, followed by oral antibiotics. Approximately 90% of cases of acute simple pyelonephritis will respond to oral antibiotics, and adequate treatment will be seen with fever resolution within 72 hours. In severe, complicated pyelonephritis or pregnancy, admission is needed with IV fluids and IV antibiotics. Fluoroquinolones, aminoglycosides, carbapenems, and extended spectrum beta-lactams can provide adequate coverage. However, if greater than 10% resistance to fluoroquinolones is present, carbapenems or aminoglycosides are first line. Two weeks of treatment with transition to PO antibiotics when hemodynamically stable and PO tolerant is warranted.2,3,13,19 Complicated pyelonephritis with severe sepsis/shock require IV antibiotics with removal/control of the instigating factor. These patients require 14-21 days of treatment with transition to PO antibiotics when able.13,19
Prognosis and Complications
Resolution depends on initial disease severity. Simple pyelonephritis usually resolves quickly with no residual renal damage. Complicated pyelonephritis has several important complications that cannot be missed. Mortality increases with older age (> 65 years), prior renal disease, and acute renal injury.
Urology consultation is usually required for emphysematous pyelonephritis, renal cortical/perinephric abscess, renal stone in the setting of pyelonephritis, and renal papillary necrosis with pyelonephritis. Emphysematous pyelonephritis has a mortality rate that reaches 80% if left untreated. Usually seen in diabetics, this is a rare necrotizing infection of the renal parenchyma with gas formation. It requires urological consult for percutaneous drainage and may need nephrectomy. Renal and perinephric abscesses are again more common in diabetics and respond to antibiotics and percutaneous drainage. Renal papillary necrosis occurs due to ischemia of the renal papilla in the medulla. Acute kidney injury is rare, but is associated with complicated pyelonephritis. Renal scarring is more common (up to 46% of patients with one episode of pyelonephritis); however, its clinical significance is controversial. 2,3,14,15
Ultimately, patients who are age greater than 65 years or have septic shock, low baseline functional status, and/or immunosuppression have longer hospital stays, higher rates of bacteremia, and greater risk of morbidity and mortality.2,3,20
Mimics
Several conditions mimic pyelonephritis and can confuse physicians.
- Pneumonia: Lower lobe pneumonia can present with flank pain. Look for respiratory symptoms such as cough and pleuritic chest pain. Listen carefully to the lungs to detect abnormal breath sounds, and use US or Chest Xray to investigate.
- Pulmonary embolism (PE): This can also present with upper back/flank pain if the infarction occurs in the lower lobes of the lung next to the pleural line. Evaluate for PE risk factors, and if positive, consider this diagnosis.
- Abdominal aortic aneurysm (AAA): The classic triad of pain, hypotension, and pulsatile mass is rare. Patients with AAA are usually older (greater than 50 years) with a history of atherosclerosis. Any abdominal or flank pain in an older patient warrants an US exam of the aorta, especially if urinary symptoms (hematuria) or femoral neuropathy symptoms are present. Any hemodynamic instability with AAA on US warrants an immediate vascular surgery consultation and type & cross for 8-10 units of packed RBCs, as rapid exsanguination may occur.
- Pelvic inflammatory disease (PID): Carefully evaluate the patient for risk factors such as new or multiple sexual partners, pain with intercourse, pelvic pain, or vaginal discharge. A pelvic exam with cervicitis, adnexal tenderness, and/or uterine tenderness provides definitive diagnosis. PID can be tricky to diagnose, and given the possible complications of the infection, one should have a low threshold to treat.
- Prostatitis: The diagnosis of prostatitis can be difficult. Patients often present with dysuria, increased frequency, and hematuria. A tender enlarged, boggy prostate is found on exam. This disease requires longer-term antibiotic therapy, often for 4 weeks or longer.
- Diverticulitis: Due to bowel innervation, this condition can present with flank pain or suprapubic pain, although it most commonly presents with left lower quadrant pain. By age 60 years, over 30% of the population has diverticulosis, and the vast majority (70%) remain asymptomatic. Erosion of the diverticular wall with microperforation leads to a localized infection. Constipation will be present in 50%, with diarrhea in 30%. CT of the abdomen/pelvis is most useful for the diagnosis.
- Appendicitis: Patients may present with vague abdominal pain that then localizes. They may or may not have fever, anorexia, elevated WBC count, vomiting, urinary symptoms, and flank pain. Over 1/3 of patients will present atypically. A careful abdominal exam, history, and imaging can make the diagnosis.
- Torsion: Ovarian and testicular torsion can present with flank pain. If the pain was sudden in onset, appears in waves, or if any suspicion of these conditions is present, complete a full GU exam and image with US while obtaining specialist consultation. These are time dependent diagnoses that can have significant morbidity if not discovered.
- Epidural abscess: Be careful of patients with back pain and red flags such as IV drug use, recent instrumentation, immunosuppression, etc., with any flank pain or back pain and fever. Diagnosis and treatment require MRI of the entire spine, antibiotics, and surgical consultation.
- Herpes zoster (HZV): Flank pain may preempt rash in HZV. If urine is negative, search the area carefully for a rash consistent with zoster. These patients should be afebrile, and urinary symptoms and nausea/vomiting are also uncommon for HZV.
- Ectopic pregnancy: Any pregnant patient with pyelonephritis warrants admission. However, one must be aware of the patient in early pregnancy with flank pain. Obtain an US to evaluate the uterus and ovaries to evaluate for ectopic pregnancy.
- Other renal pathology: Be careful of renal artery embolism, renal vein thrombosis, and nephrolithiasis. Look for risk factors (coagulopathic state, family history, transplant history) and image appropriately.
Summary
– Pyelonephritis is infection of the kidney. Acute infection is most commonly caused by enteric organisms that ascend from a lower tract infection. Hematogenous infection may occur.
– Simple pyelonephritis occurs in non-pregnant, non-immunosuppressed females of reproductive age with normal renal function pre-infection. Anyone else should be considered complicated.
– Key historical and exam factors include dysuria, frequency, CVA tenderness, fever, and absence of vaginal discharge.
– Use urine dipstick wisely. LE and nitrites are usually positive. WBC casts may be present.
– Simple pyelonephritis can be discharged with PO antibiotics and follow up.
– Sepsis due to pyelonephritis can be deadly and must be diagnosed and treated promptly with antibiotics and source control. A urology consultation should also be considered.
– Beware of pyelonephritis mimics including: pneumonia, PE, AAA, chronic pyelonephritis, PID, pelvic pain syndrome, prostatitis, diverticulitis, appendicitis, ovarian/testicular torsion, HZV, epidural abscess, and ectopic pregnancy.
References/Further Reading
- Hooton TM, Stamm WE. Diagnosis and treatment of uncomplicated urinary tract infection. Infect Dis Clin North Am. 1997;11:551-81.
- Ramakrishnan K and Scheid DC. Diagnosis and management of acute pyelonephritis in adults. Am Fam Physician. 2005;71:933-42.
- Fulop T. Acute Pyelonephritis. Emedicine/Medscape. http://emedicine.medscape.com/article/245559. Accessed 02 October 2015.
- Stamm WE, Hooton TM. Management of urinary tract infections in adults. N Engl J Med. 1993;329:1328-34.
- Bass PF, Jarvis JA, Mitchell CK. Urinary tract infections. Prim Care. 2003;30:41-61.
- Giesen LG, Cousins G, Dimitrov BD, van de Laar FA, Fahey T. Predicting acute uncomplicated urinary tract infection in women: a systematic review of the diagnostic accuracy of symptoms and signs. BMC Fam Pract. 2010 Oct 24;11:78.
- Bent S, Nallamothu BK, Simel DL, Fihn SD, Saint S. Does this woman have an acute uncomplicated urinary tract infection? JAMA. 2002 May 22-29;287(20):2701-10.
- Medina-Bombardó D, Seguí-Díaz M, Roca-Fusalba C, Llobera J; dysuria team. What is the predictive value of urinary symptoms for diagnosing urinary tract infection in women? Fam Pract. 2003 Apr;20(2):103-7.
- Meister L, Morley EJ, Scheer D, Sinert R. History and physical examination plus laboratory testing for the diagnosis of adult female urinary tract infection. Acad Emerg Med. 2013 Jul;20(7):631-45.
- Simerville JA, Maxted WC, and Pahira JJ. Urinalysis: a comprehensive review. Am Fam Physician. 2005;71:1153-62.
- Rubin RH, Shapiro ED, Andriole VT, Davis RJ, Stamm WE. Evaluation of new anti-infective drugs for the treatment of urinary tract infection. Infectious Diseases Society of America and the Food and Drug Administration. Clin Infect Dis. 1992;15(suppl 1):S216-27.
- McMurray BR, Wrenn KD, Wright SW. Usefulness of blood cultures in pyelonephritis. Am J Emerg Med. 1997;15:137-40.
- Gupta K, Hooton TM, Naber KG, Wullt B, Colgan R, Miller LG, et al. International clinical practice guidelines for the treatment of acute uncomplicated cystitis and pyelonephritis in women: A 2010 update by the Infectious Diseases Society of America and the European Society for Microbiology and Infectious Diseases. Clin Infect Dis. 2011 Mar 1. 52(5):e103-20.
- Kofteridis DP, Papadimitraki E, Mantadakis E, et al. Effect of diabetes mellitus on the clinical and microbiological features of hospitalized elderly patients with acute pyelonephritis. J Am Geriatr Soc. 2009 Nov. 57(11):2125-8.





4 thoughts on “Pyelonephritis: It’s not always so straightforward…”
Pingback: strength in numbers: Pyelonephritis | DAILYEM
Pingback: Asynchronous Learning: Renal and Urogenital Emergencies - Bold City Emergency Medicine
Pingback: emDOCs.net – Emergency Medicine EducationRenal colic mimics: Differential diagnosis and approach to management - emDOCs.net - Emergency Medicine Education
Pingback: UVI och Pyelonefrit – Mind palace of an ER doc