
Author: Ian Bodford, MD (EM Resident Physician, UTSW / Parkland Memorial Hospital) // Editors: Alex Koyfman, MD (@EMHighAK, EM Attending Physician, UTSW / Parkland Memorial Hospital) and Stephen Alerhand, MD (@SAlerhand)

You are deep into one of your busy night shifts, and one of your frequent flyers shows up via EMS. Your nurse approaches you and exasperates, “Mr. X is back again, and of course he is drunk. His vital signs are normal, and he is snoozing in room 7 whenever you can get to him.” Admittedly, this patient goes to the bottom of your triage list. An hour or so later, you get around to walking into room 7 and discover Mr. X still asleep on the stretcher. You sternal rub him and he does not arouse very easily. While sternal rubbing, you feel a bottle in his jacket pocket. You pull it out to discover an almost empty bottle of windshield wiper fluid and suddenly begin to panic as this is not your typical intoxicated patient.
Background
When discussing toxic alcohols, it is important to define what constitutes a “toxic” alcohol. Any alcohol when consumed in enough of a quantity can be toxic; however, we will not discuss ethanol as it is not one of the classic “toxic alcohols.” These typically include methanol, ethylene glycol, propylene glycol, and isopropanol (isopropyl alcohol). Also, we will not be discussing propylene glycol due to the rarity of its consumption. Propylene glycol toxicity is seen mainly in an inpatient setting with IV infusions that contain propylene glycol as an excipient. Since this is a focused review for the emergency department setting, this leaves three “toxic alcohols” to discuss.
Why would someone ever consume these alcohols? Typically, these substances are used for two reasons: suicide/homicide or inebriation. Toxic alcohols are more readily available than ethanol and are usually cheaper. This is especially true in patients who are under the legal drinking age. Toxic alcohol assays are commercially available, but are rarely used in hospital laboratories. It remains a challenge to diagnose these patients in the emergency room, as many of them mimic simple ethanol intoxication.
Pathophysiology

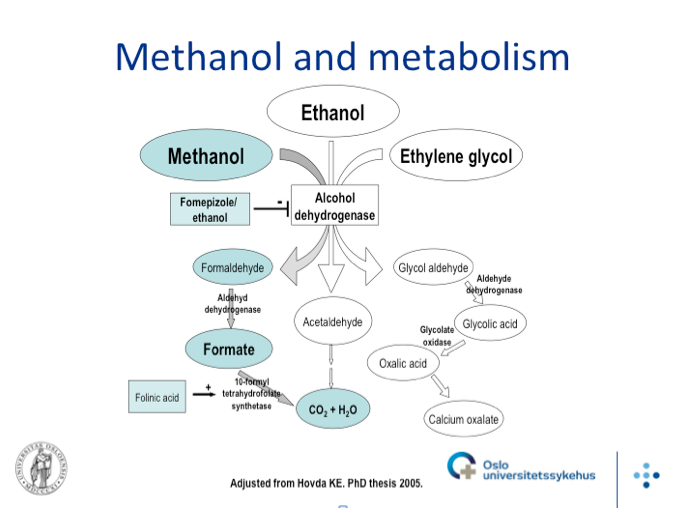
Methanol also called methyl alcohol is found in windshield wiper fluid, de-icing products, paint removers, photocopying fluid, shellacs, and embalming fluid. A rarer place that a patient would consume methanol is in contaminated moonshine. Very rarely, inhalational and dermal exposures have been reported. Methanol is metabolized in the liver to formaldehyde by alcohol dehydrogenase. The formaldehyde is then metabolized by aldehyde dehydrogenase to formic acid. The formic acid inhibits cytochrome c in the mitochondria, shifting the cell to anaerobic glycolysis, leading to lactic acid accumulation. Methanol ingestion is the M in the MUDPILES mnemonic; thus, it is an elevated anion gap metabolic acidosis. The formic acid buildup and lactic acid buildup are to thank for this. The acidosis leads to the byproducts crossing the blood-brain barrier leading to neurologic effects, including Parkinsonism, transverse myelitis, and basal ganglia hemorrhages. Methanol leads to the classic “snowstorm” vision and also photophobia. Methanol ingestion usually provides a decreased level of inebriation compared to ethylene glycol and isopropyl alcohol; however, if coingested with ethanol, this is not a reliable symptom. With the acidosis, the patient may be hyperventilating to compensate.

Ethylene glycol is found in radiator antifreeze, degreasing agents, and metal cleaners. It has no smell or color and tastes sweet. Ethylene glycol is metabolized in the liver to glycoaldehyde by alcohol dehydrogenase. Glycoaldehyde is then converted to glycolic acid by aldehyde dehydrogenase, which is then converted to glyoxylic acid, then to oxalic acid. It is this acid that combines with serum calcium to form the classic calcium oxalate crystals found in the urine of patients who have consumed ethylene glycol. Ethylene glycol is the E in the MUDPILES mnemonic, meaning that it causes an elevated anion gap metabolic acidosis. NAD+ is a cofactor needed for alcohol dehydrogenase in the first step of ethylene glycol’s breakdown. Once these stores are depleted, the pathway is shunted to the citric acid cycle where lactate is a byproduct. The neurologic effects of ethylene glycol are coma, seizures, meningismus, muscle spasms, and paralysis of the extraocular muscles. It can also affect the heart and lungs, causing tachycardia, hyperventilation, ARDS, and heart failure. Hypocalcemia and resulting QT prolongation are due to serum calcium combining with oxalic acid. Lastly, kidney failure is due to these calcium crystals depositing into renal tubules. This also causes flank pain and oliguria.

Isopropanol is the most commonly ingested toxic alcohol in the United States. Isopropyl alcohol is found in solvents and disinfectants. It is also found in mouthwashes, lotions, as well as rubbing alcohol and hand sanitizers. It is also hepatically metabolized by alcohol dehydrogenase to acetone. The acetone does not undergo further metabolism, and no acid byproducts are formed. This means that isopropanol is the only toxic alcohol that does not cause an elevated anion gap acidosis. It can cause hemorrhagic gastritis and profound inebriation with cerebellar signs and coma. Due to the acetone byproduct, the patient will sometimes have a fruity odor on their breath.
Epidemiology
According to the 2012 data from the United States Poison Control Center, 16,458 cases of isopropyl alcohol ingestions were reported. 8,773 of these cases were classified as a “toxicity” with 65 patients experiencing “major morbidity,” but only one patient dying. Also in 2012, there were 1,612 cases of ingestion of methanol, with 26 patients having “major morbidity” and 6 deaths. There were 5,869 cases of ethylene glycol ingestion, with 205 having a “major morbidity” and 23 deaths.
Diagnosis
Certain patients will make for an easy diagnosis, like the patient in the opening scenario; however, the conundrum for the emergency physician lies in the patient that appears intoxicated, but has not obviously ingested a toxic alcohol. How do we as emergency physicians know when to suspect a toxic alcohol ingestion? It is a difficult question to answer. It is extremely important to listen to what the patient (if coherent), family/friends, and EMS have to say regarding the patient’s condition. Clinical suspicion should always remain high when a “drunk” patient is brought in to the department. Of course, any patient with symptoms listed above should raise suspicion.
If toxic alcohol ingestion is suspected, the patient’s blood should be sent for serum levels of the toxic alcohols; however, these usually take several hours to days to return depending on your hospital’s laboratory. While you wait for these results, a BMP, ethanol level, lactate, serum osmolarity, and an ABG/VBG should be ordered. The BMP provides useful information about the patient’s creatinine. It also provides the patient’s anion gap, which will be elevated in toxic alcohol consumption other than isopropanol. The ethanol level helps prove that the intoxication is from something else other than ethanol. Lactate will usually be elevated with methanol or ethylene glycol consumption. The ABG/VBG reveals how acidotic a patient is. If a patient’s osmolar gap is >10-25 mOsm in the setting of an elevated anion gap, this is highly suggestive of toxic alcohol ingestion. Keep in mind that the osmolar gap will be elevated early on as the parent compound of the toxic alcohol is still present; however, it will gradually decrease, and the anion gap will increase as more toxic metabolites are formed. The patient’s urine can be analyzed under a Wood’s lamp. Sodium fluorescein, which is found in antifreeze will fluoresce under a black light. The urine can also be analyzed under microscopy for presence of urinary calcium oxalate crystals. It is important to note that these two urine tests are highly unreliable. If imaging of the brain is performed, a CT or MRI might show putamen necrosis or basal ganglia hemorrhages in methanol ingestion.
Management
The first initial step in treating any patient with a poisoning should be to call the poison control center at 1-800-222-1222. A toxicologist should be involved early in these cases. Although used in the past, GI decontamination is no longer recommended. The main goal of treatment is blocking the conversion of the mother compounds to their toxic metabolites. This is done by blocking alcohol dehydrogenase. Both fomepizole and ethanol have a higher affinity for alcohol dehydrogenase than the toxic alcohols and can be used as antidotes for methanol/ethylene glycol poisoning; however, fomepizole is preferred due to its better side effect profile and ease of use. The loading dose for fomepizole is 20 mg/kg and then 10 mg/kg every 12 hours for 4 doses. The question is when is a poisoning bad enough to use the antidote. If the serum levels of methanol or ethylene glycol are greater than 20 mg/dL, antidote therapy should be started. Also, if there is a high suspicion of toxic alcohol poisoning and two of the following, fomepizole should be given: osmolar gap > 10 mOsm, arterial pH < 7.3, bicarbonate < 20 mmol/L, or the presence of urinary oxalate crystals.
A sodium bicarbonate infusion should be started if the patient’s arterial pH is less than 7.3 with a goal pH between 7.35 and 7.45. Hemodialysis can also be used in these patients. Indications for dialysis are pH < 7.25, changes in vision, kidney failure, electrolyte abnormalities not treated by conventional means, unstable hemodynamics, or a serum concentration > 50 mg/dL. If antidote therapy is begun early enough, dialysis can usually be avoided in ethylene glycol poisoning. Methanol is usually eliminated too slowly for fomepizole to be effective alone. Cofactors can also be administered to help with the conversion of toxic metabolites to non-toxic metabolites. For ethylene glycol, both thiamine and pyridoxine should be given. For methanol, folic acid or folinic acid should be given.
Isopropyl alcohol poisonings are usually treated supportively. The patient’s CNS depression can be profound enough to require intubation. Also, proton pump inhibitors should be used if hemorrhagic gastritis is suspected. Hemodialysis can also be effective for these patients, but is usually reserved for patients with declining GCS or unstable vital signs.
Disposition
Now that you have successfully diagnosed and began treating your poisoned patient, what is their likely disposition? If their serum concentration is < 20 mg/dL and there are no signs of end organ damage with stable vital signs, the patient can be either admitted to a floor bed or watched in the emergency department for several hours. A repeat level should be drawn prior to discharge to make sure it is trending down. If the patient is acidotic or has end organ damage, ICU admission is appropriate. If toxic alcohol levels are not available at your hospital, a patient can be cleared after a few hours of observation if you have a low suspicion for toxic alcohol ingestion, they have a normal anion and osmolar gap, they have a normal pH, and they have improvement in their clinical picture. If hemodialysis or fomepizole are unavailable at your hospital, transfer to another hospital is appropriate.
Major Points
– Always have toxic alcohol ingestion in the differential when seeing an inebriated patient. Although rare, having a high clinical suspicion can help save lives. Obtain a thorough history from any and all persons involved.
– Methanol: byproducts cause an elevated anion gap metabolic acidosis. Effects of ingestion are inebriation (less so than ethanol, ethylene glycol, or isopropanol), Parkinsonism, transverse myelitis, and basal ganglia hemorrhages. Patients also might complain of “snowstorm” vision.
– Ethylene glycol: byproducts cause an elevated anion gap metabolic acidosis. Effects of ingestion are inebriation, coma, seizures, meningismus, muscle spasms, and paralysis of the extraocular muscles. Also causes tachycardia, hyperventilation, ARDS, and heart failure. One of the byproducts of breakdown combines with calcium to form crystals. These deposit in the kidney leading to kidney injury and can cause hypocalcemia with resulting QT prolongation.
– Isopropanol: most commonly ingested toxic alcohol but does not lead to metabolic acidosis. Effects of ingestion are severe inebriation, fruity smelling breath, and hemorrhagic gastritis.
– Obtain a BMP, ethanol level, lactate, serum osmolarity, and an ABG/VBG. A serum osmolar gap of >10-25 mOsm in the setting of an anion gap is highly suggestive of toxic alcohol exposure. Examine the urine for crystals.
– Call the poison control center at 1-800-222-1222 when toxic alcohol consumption is suspected. If suspicion is high enough, begin fomepizole administration prior to labs resulting as time equals tissue. Hemodialysis may ultimately be needed. Immediate transfer to another facility is warranted if fomepizole or hemodialysis are not available.
References/Further Reading
– Burns, Edward. Life in the Fast Lane. “Toxic Alcohol Ingestion.” Life in the Fast Lane. <http://lifeinthefastlane.com/toxic-alcohol-ingestion/>
– Krautz and Kurtz. “Toxic Alcohol Ingestions: Clinical Features, Diagnosis, and Management.” Clinical Journal for the American Society of Nephrology. Nov 2007. <http://cjasn.asnjournals.org/content/3/1/208.full>
– Levine MD, Michael, et. al. “Alcohol Toxicity.” Medscape. 25 Mar 2015. <http://emedicine.medscape.com/article/812411-overview#a6>
– Patil N, Becker MWL, Ganetsky M (2010). Toxic Alcohols: Not Always A Clear-Cut Diagnosis. Emergency Medicine Practice, 12 (11).
– http://www.ncbi.nlm.nih.gov/pubmed/25493973
– http://www.ncbi.nlm.nih.gov/pubmed/23431453





7 thoughts on “The Unhappy Drunk: Toxic Alcohols”
Pingback: Weekly Review | theNursePath
Pingback: LITFL Review 199 | LITFL: Life in the Fast Lane Medical Blog
Pingback: Toxic Alcohols | FOAM links
Pingback: Отравление метиловым спиртом — Девятый вызов | The 9th Call |
Pingback: Toxic Alcohols - Minding the Gaps | Emergency Medicine Cases
Pingback: emDOCs.net – Emergency Medicine EducationEM@3AM: Ethylene Glycol Toxicity - emDOCs.net - Emergency Medicine Education
Pingback: emDOCs.net – Emergency Medicine EducationEM Cases: Toxic Alcohols - Minding the Gap - emDOCs.net - Emergency Medicine Education