Author: Michael Ullo, MD (EM PGY-2 Resident, Rutgers NJMS Dept. of Emergency Medicine), Cynthia Santos, MD (Assistant Professor Emergency Medicine, Medical Toxicology, Rutgers NJMS Dept. of Emergency Medicine) // Edited by: Alex Koyfman, MD (@EMHighAK, EM Attending Physician, UTSW / Parkland Memorial Hospital), and Brit Long, MD (@long_brit, EM Attending Physician, San Antonio, TX)

Case:
A 46-year-old male with a history of recurrent dyspepsia and recent weight loss presents to the Emergency Department (ED) for evaluation of cyanosis. Earlier that day, the patient underwent endoscopy for evaluation of his symptoms. Notes from the procedure indicate that the patient was premedicated with intraoral benzocaine spray and intravenous midazolam. During the procedure, the patient was noted to “turn blue” with a oxygen saturation of 86% on room air. Supplemental oxygen was provided via nasal cannula without any improvement in skin color or saturation. The procedure was aborted, and the patient was transported directly to the ED.
On examination, the patient’s vitals are remarkable for an oxygen saturation of 86% on 6 liters nasal cannula. The patient is awake, speaking full sentences, and in no acute distress. Physical examination is only remarkable for perioral cyanosis. Arterial blood gas with co-oximetry shows a pH of 7.41, PaO2 265 mmHg, and methemoglobin level of 13%.
Questions:
- What is methemoglobinemia?
- What common agents induce methemoglobin formation?
- Is there an antidote for methemoglobinemia?
Background:
- Methemoglobin (MetHb) normally accounts for < 1% of the total hemoglobin in the human body. MetHb is formed when the heme iron of deoxyhemoglobin is oxidized from the ferrous (Fe2+) to ferric (Fe3+) state.
- This oxidation shifts the hemoglobin dissociation curve to the left, resulting in impaired oxygen delivery. This leftward shift results in a “functional anemia” where the amount of functional hemoglobin is less than the amount of total hemoglobin.
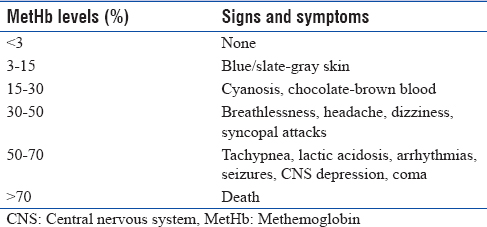
- Consequently, symptoms of methemoglobinemia mimic an acute impairment of oxygen delivery to tissues. Patients can present with cyanosis, fatigue, dyspnea, tachycardia, and lethargy.

When should the ED physician suspect methemoglobin?
- Methemoglobin should be suspected in any patient with sudden onset findings of inadequate oxygen delivery that does not respond to supplemental oxygen.
- The degree of hypoxia does not necessarily correspond to the amount of methemoglobin in the blood.
- Additionally, methemoglobin causes blood to turn a characteristic “chocolate” color.
What are the common causes of methemoglobin formation?
- Methemoglobin can have acquired or congenital causes, with the former being more common.
- Acquired causes include exposure to drugs or toxins that oxidize ferrous iron. Local anesthetics (including benzocaine), nitrates and nitrites are frequently associated with MetHb formation.
- Other implicated agents include sulfonamide antibiotics, dapsone, chloroquine, and primaquine.
- Congenital causes, although rare, include enzymatic deficiencies (NADH methemoglobin reductase) and Hemoglobin M (a hemoglobin variant that is stabilized in the oxidized form).
How is the diagnosis confirmed?
- Definitive diagnosis is made on co-oximetry of either venous or arterial blood gas samples. This testing can give the percentage of hemoglobin in the methemoglobin state.
- Another clue to the diagnosis will be a normal partial pressure of oxygen on an obtained arterial sample (or high if on supplemental O2).
- Typically cyanosis will be evident when levels of methemoglobin reach 10-15% of total hemoglobin in nonanemic persons, but this % can be higher in anemic persons. Cyanosis usually occurs when methemoglobin concentration exceeds 1.5 g/dL of methemoglobin.
- For example, a patient with a hemoglobin concentration of 15 g/dL will typically develop cyanosis when methemoglobin percentages exceed 10%. On the other hand, a person with a hemoglobin concentration of 6 g/dL may not develop cyanosis until the methemoglobin percentage exceeds 25%.
What is the management and disposition?
- When a diagnosis of methemoglobinemia is made, symptomatic patients should receive the appropriate antidote, methylene blue.
- This compound is a thiazine dye that increases the conversion of methemoglobin to hemoglobin via enzymatic reduction.
- A 1% solution of methylene blue should be administered as a 1-2 mg/kg (0.1 to 0.2 mL/kg) dose intravenously over five minutes.
- Consultation with a medical toxicologist can help guide management as additional doses may be necessary.
- Final disposition will vary depending on response to the antidote and persistence of symptoms.
References:
- Garza F, Kearney TE. Chapter 205. Methylene Blue. In: Olson KR. eds.Poisoning & Drug Overdose, 6e New York, NY: McGraw-Hill; 2012
- Hoffman, R. S. 1., Howland, M. A., Lewin, N. A., Nelson, L., Goldfrank, L. R., & Flomenbaum, N. (2015). Goldfrank’s toxicologic emergencies (Tenth edition.). New York: McGraw-Hill Education.
- Madke, Bhushan & Kumar, Piyush & Kabra, Poonam & Lata Singh, Adarsh. (2016). How to manage a side effect: Dapsone-induced methemoglobinemia. Indian Journal of Drugs in Dermatology. 2. 117-120. 10.4103/2455-3972.196225.
- Marx, J. A., & Rosen, P. (2014). Rosen’s emergency medicine: Concepts and clinical practice (8th ed.). Philadelphia, PA: Elsevier/Saunders.
- Williams SR, Sztajnkrycer MD, Thurman R. TOXICOLOGICAL CONDITIONS. In: Knoop KJ, Stack LB, Storrow AB, Thurman R. eds. The Atlas of Emergency Medicine, 4e New York, NY: McGraw-Hill





6 thoughts on “Tox Card: Methemoglobinemia”
Awesome work, will bookmark, will share, would recommend to those in training.
Great article!
Thanks great article! When I was practicing in the Philippines, I have encountered families from a rural community turning blue after eating “longganiza” or local chorizo/ sausage. Found out that such food was loaded with too much potassium nitrate. Thank goodness, no mortality.
As a point of clarification, cyanosis may be present with metHb when the total concentration exceeds 1.5 g/dL of metHb. Meaning if a patient has a baseline hemoglobin of 15 g/dL, 10% metHb will cause cyanosis. However, if the patient has anemia with baseline hemoglobin of 8 g/dL, the patient may not be cyanotic until 19% methb. So it is very important to interpret the metHb concentration relative to the total hemoglobin. Thanks for the article!
Excellent point. We will update the article with your feedback. Thank you for the comment!
Pingback: Länkar v43-44 | Internmedicin