
Authors: Demetrios Neofitidis, DO (Lincoln Medical Center Bronx New York), Jeffrey Uribe, MD (Lincoln Medical Center Bronx New York), and Muhammad Waseem, MD, MS (Lincoln Medical Center & St. Georges University Grenada West Indies)// Edited by: Alex Koyfman, MD (@EMHighAK) and Brit Long, MD (@long_brit)
Falls come in all shapes and sizes, especially with trauma. This post will cover falls in special populations, including the elderly, intoxicated patients, and falls from extreme height.
Geriatric
Case
A 67-year-old male is brought to the emergency department after a fall from standing. He reports that he tripped over a crack in the road causing him to fall forward and strike his head on the edge of a step. He denies loss of consciousness, vision changes, nausea, or vomiting. He is complaining of a headache and pain around the site of impact.
His past medical history is significant for hypertension, hyperlipidemia, and atrial fibrillation. He is taking rivaroxaban.
Background/Incidence
Geriatric patients commonly visit the ED for various reasons. Burns et al states that adults aged >85 years are the fastest growing age group among U.S. citizens and are expected to reach nearly 9 million in 2030 (2). Among their presentations, falls account as being the most common cause of both fatal and nonfatal injuries, especially in those > 65 years of age (5). The total visits of fall-related emergencies in the patient population are estimated to be 3 million per year (2). One should expect to deal with older population as we move through our careers as well as the social, medical, and legal dilemmas that come with them.

While a simple trip-and-fall may not prompt an initial inquiry, multiple falls or first time falls without a clear mechanism should raise a red flag. Outlined below are some of the common causes of falls in the elderly population, both dangerous and benign.
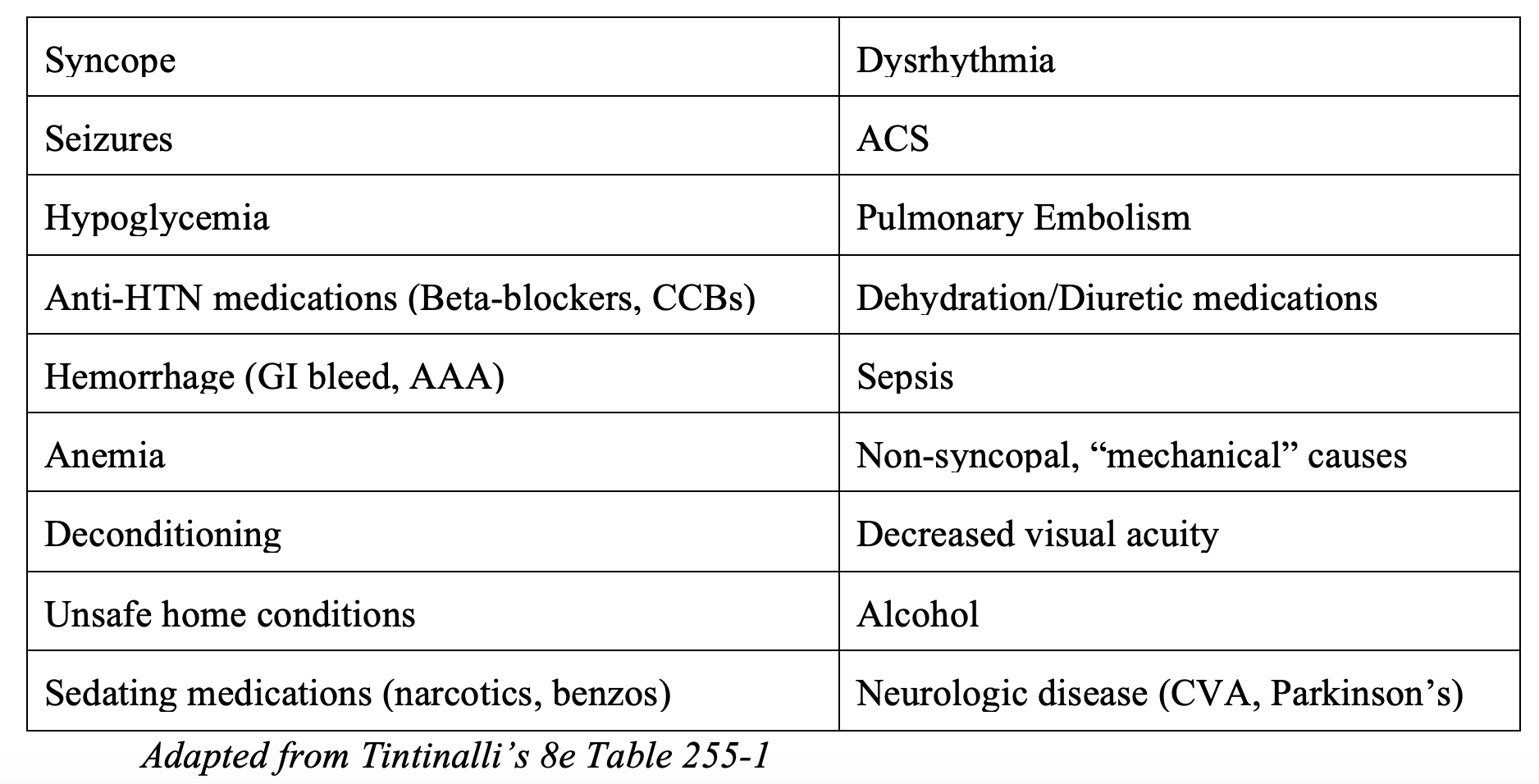
Looking at this list closely shows that not all causes are readily apparent on a primary or secondary survey. History taking and collateral information from family, nursing home staff, home health attendants, visiting nurse services, and EMS can uncover more occult diagnoses (e.g. syncope vs trip and fall) for falls in this population.
Assessment
Step 1: Think of mechanism/cause first!
- Take a careful fall history and use your collateral from EMS and family to help differentiate between mechanical fall and syncope.
- Make note of common risk factors as seen above including medication changes.
- Bathroom falls (hard surface), stairs (higher energy fall vs ground falls).
- Keep differential broad for medical causes that can contribute to falls including cardiac disease, sepsis and GI bleeds.
Step 2: Assess for injuries from the fall
- After your ABCDs have been completed make sure to go through a thorough exposure and take time during your secondary survey to avoid missing any minor injuries.
- Don’t be fooled by normal vital signs – tachycardia masked by beta-blockers, normotensive in a regularly hypertensive patient. One study reported that 39% of patients with a systolic blood pressure >90 mm Hg and heart rate <120 beats/min still had occult hypoperfusion (9).
- Living situation – i.e. live alone = prolonged down-time (rhabdomyolysis can cause dehydration, elevated creatinine and electrolyte disturbances).
Step 3: Disposition challenges (as discussed below).
Step 4: Plan for prevention (as discussed below).
Anticoagulants
A study conducted by the National Electronic Injury Surveillance System–Cooperative Adverse Drug Event Surveillance system showed that oral anticoagulant or antiplatelet agents (warfarin, aspirin, and clopidogrel)were one of3 medication classes that contributed to 48% of all ED visits for adverse drug effects in patients older than 65 years (7). These medications pose a challenge to emergency physicians especially in the absence of clear documented injury such as subdural or epidural hematomas.
- Important questions on triage (i.e. what medication, what dose, last dose).
- Considerations for reversal and observation.
- Nishijima et al. studied a total of 1,064 patients (768 warfarin patients [72.2%] and 296 clopidogrel patients [27.8%])with an average age 75.4 to determine the incidence of immediate and delayed intracranial hemorrhage (6).
- Results: prevalence of immediate traumatic intracranial hemorrhage in patients with clopidogrel was significantly higher compared with those receiving warfarin despite the cohorts’ having similar characteristics (6).
- Conclusions: development of a delayed traumatic intracranial hemorrhage after a negative initial cranial CT scan result is rare and does not warrant routine hospitalization for observation or immediate anticoagulation reversal with blood products (6).
- ED Observation vs imaging vs repeat imaging vs admission for observation and possible imaging.
- McCammack et al showed that patients presenting with mild traumatic brain injury (defined as presenting GCS between 13-15) on anticoagulant, antiplatelet or combination therapy with an initial negative non-contrast CT Brain did not require observation or repeat imaging (5). They also postulated that “normal presentation GCS and neurological examinations, no associated LOC, on single anticoagulant therapy and no antiplatelet agent, may be able to forego initial imaging altogether.”
- Anticoagulation can affect length of stay and contribute to complications for those admitted and thus should prompt admitting teams to monitor certain patients more closely.
- Coleman et al assessed effect of anticoagulation (aspirin, warfarin, clopidogrel, enoxaparin, and dipyridamole) status on hospital course, complications, and outcomes among geriatric fall trauma patients (3). They concluded Warfarin led to longer lengths of stays and days in the ICU while Clopidogrel had a higher mortality and complication rate.
- See REBELEM for a great video on reversal and the details on who should be considered by Dr. Scott Wieters (@EMedCoach).
Disposition and follow up
- Timed Up and Go (TUG) test in ED first described by Podsialdo and Richardson:
- Performed by having patient raise from a seated position, walk approximately 10 feet at their usual pace, turn, and return to the seat.
- Times >13.5 seconds identified those at risk for future falls.
- Some controversy as to the utility of this test. Some studies have shown no correlation to future fall risk while the same studies have shown correlation to functional decline at 3 and 6 months (1).
- Ultimately, the risk stratification of elderly fall patients should not rely on a single tool but should be multidisciplinary and involve community services.
- Evaluate future fall risk – multi-faceted and includes gait, balance, vision, and addressing polypharmacy.
- Multidisciplinary – include family, nursing, social work.
- Ensure a safe and well-established discharge plan that includes follow up and monitoring by family or caretakers.
- Have a low threshold to admit geriatric patients with polytrauma or who may need opioid pain medication as this can precipitate delirium, decrease balance and impair ambulation (9).
- If the barriers to a safe home environment exist at discharge then admission may allow for appropriate and safe pain control, physical therapy assessment and social work consultation to limit secondary injury (9).
Pearls
- Treat elderly patient falls as both medical and trauma.
- Use patient, family and EMS to uncover mechanism and details of scene.
- Fully assess medication list, paying special attention to anticoagulants.
- Involve a multidisciplinary team for disposition challenges.
Intoxicated
Case
A 35-year-old alcohol dependent patient is brought by emergency medical services (EMS) to your Emergency Department (ED) after being found unconscious on the sidewalk. On examination, you clearly see the patient is intoxicated and has an abrasion to the right eyebrow. The patient is severely intoxicated and unable to provide history. You decide to monitor the patient in the ED. After about 2 hours, the patient becomes agitated and attempts to walk out of the ED stating, “I want to sign out AMA!” You manage to convince the patient to stay for observation for a few more hours. You wonder to yourself, “should my management of this patient be any different?”
Background/Incidence
According to a study conducted by the National Institute on Alcohol Abuse and Alcoholism (NIAAA), the number of ED visits related to acute alcohol consumption increased by 51.5% (1.8 million to 2.7 million) and the rate increased by 40% (720 to 1000 per 100,000 population) between 2006 and 2014, accounting for a total of 8.7 billion in costs of ED services (1). A retrospective review by Mullins et al., showed that utilization of resources such as laboratory tests, medications and radiography all increased, with the use of advances imaging (CT or MRI) increasing 232.2% from 2001-2002 to 2010-2011 (2).
Between 2006 and 2010, approximately 88,129 deaths occurred each year where roughly 49,544 deaths annually resulted from (1):
a) 7,541 falls
b) 12,460 car crashes
c) 1,647 alcohol overdoses
d) 8,404 overdoses
The increase in rates do not appear to be related to general increase in alcohol consumption, since the increase in per capita alcohol consumption was less than 2% (1). As emergency physicians, we must be prepared to appropriately manage intoxicated patients in order to prevent any morbidity and mortality in this population.
Assessment
The assessment should begin with attention to ABCs. An intoxicated patient in a comatose state is at risk for aspiration and if the airway is unprotected (no gag reflex) or the patient has poor respiratory effort, the patient must be intubated. Although the clinical decision rules for cervical spine and brain imaging are available (3, 4). However, often the cervical spine may not be cleared clinically, and patients are commonly placed in a c-collar, if not already placed by EMS. A focused history and physical exam are warranted including any collateral information from EMS, friends and families, and at times, careful search of the patients belonging for any helpful clues (overdose, drugs…etc.). These patients should be undressed to assess whether any injuries exist.
One must not assume the etiology of the patient’s presentation especially if cognition is altered, is due to alcohol intoxication. It is important to keep a broad differential as there are mimics of alcohol intoxication (5). It is also important to keep in mind that alcoholics may present with trauma due to underlying medical illnesses/emergencies (6).

A simple first step is to obtain a bedside glucose level as alcoholics are at higher risk for hypoglycemia, and a core temperature as these patients are commonly found outside in the cold or directly in the sun and at risk for hypothermia or heat stroke, respectively. If pinpoint pupils, bradypnea or track marks are present with the patient unresponsive, Naloxone should be administered in case of concomitant opiate overdose.
Blood Alcohol Levels
Electrolyte abnormalities in alcoholics, especially chronic users is common and a basic metabolic panel with magnesium and phosphate should be obtained. The question is whether a blood alcohol concentration (BAC) should always be ordered? Intoxication is used to describe a level that produces clinical identifiable impairment that may alter sensation, coordination, judgement, and insight (7). That level as we know, varies from person to person. The root of the question actually lies in whether the diagnosis of ethanol intoxication is in question? The alcohol level may be useful in patients with trauma presenting with cognitive and psychomotor impairment, delirium/agitation due to possible intracranial pathology, altered mental status, seizures, antifreeze ingestions, and patients whose conditions does not improve over time to name a few. The medicolegal aspects of an ethanol level often come into play at the point of discharge. Having a documented BAC, not allowing adequate time for ethanol to be metabolized and the patient being discharged despite being clinically sober may carry a degree of medicolegal risk.
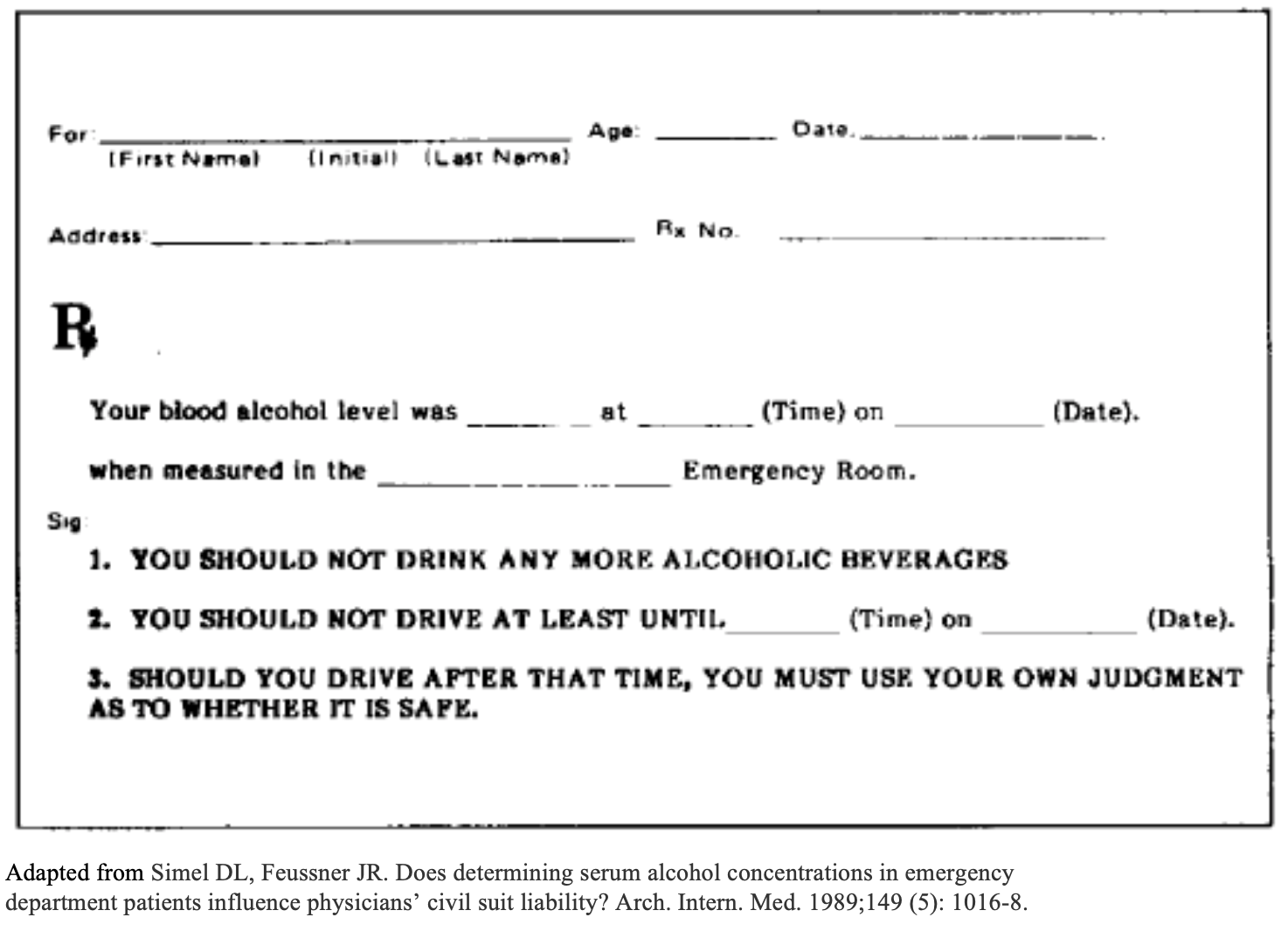
In a survey of plaintiff’s attorney’s attitudes of a hypothetical case of a patient seen for alcohol intoxication and had an accident shortly after discharge: 43% of attorneys would advise patient to sue for negligent care if elevated BAC was documented and no advice was given regarding drunk driving compared to only 17.3% of attorneys would give similar advice if impairment was not documented and no advice was given regarding drunk driving. However, if BAC is documented and specifically advised not to drive, only approximately 4% of attorneys would suggest to provider was negligent (8).
To provide evidence against future litigations, a written prescriptions or discharge instructions should be noted that the patient cannot drive because of a higher-than-legal BAC (figure 1) (8). If the patient is accompanied by someone (family member or friend), this person can also sign the discharge papers, and their name and relationship should be mentioned in the medical record. The role of the accompanying person is not to just drop the patient off, but to stay until the effects of the acute intoxication have fully resolved (9).
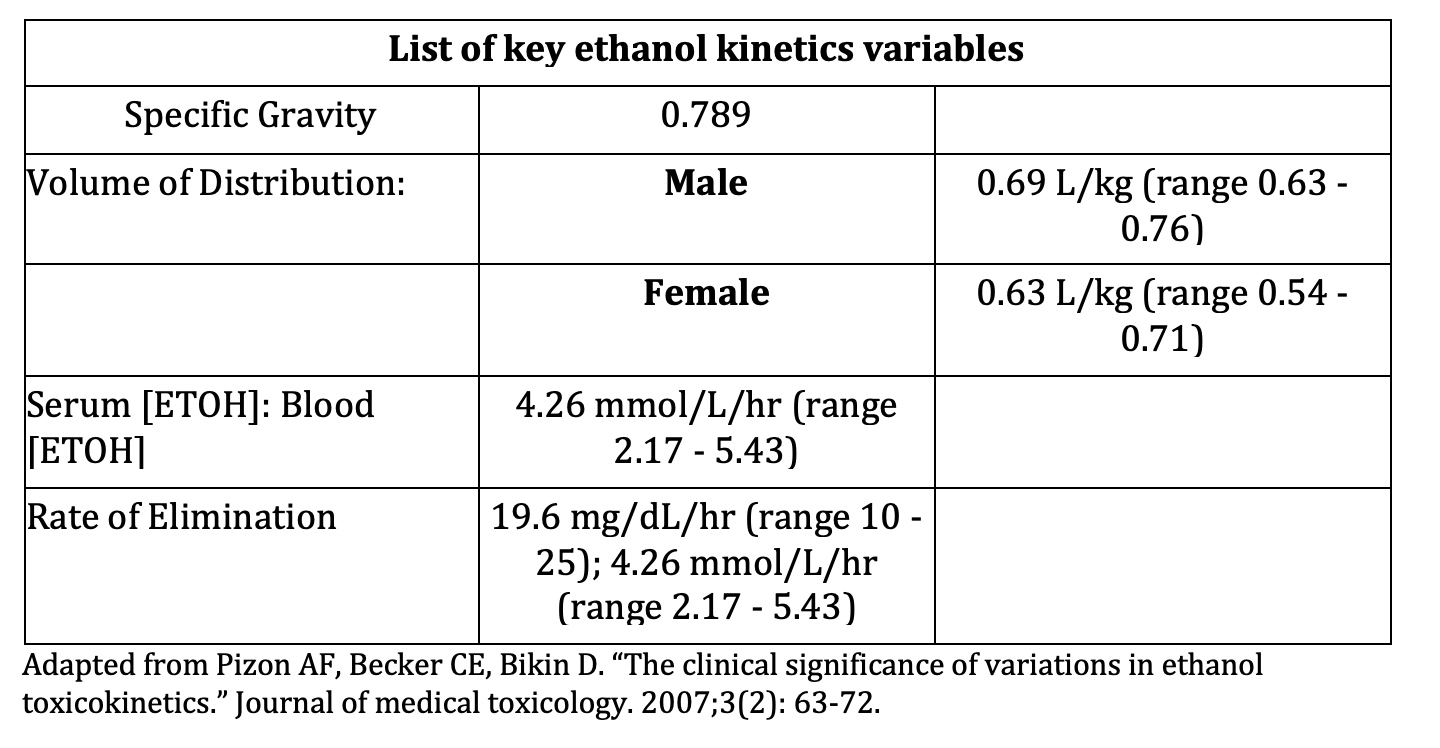
If you decide to not order alcohol level and you believe the patient is honest about the number, type and time of alcohol drinks, you may be able to calculate a rough estimate of the patients’ blood alcohol concentration (BAC) using the below alcohol content and formulas (10):


With an estimated calculated BAC and the average rate of elimination, you may determine an alcohol level where the patient may be safe for discharge.

Imaging
There are a certain clinical decision rules that guide physicians to determine whether CT acquisition is necessary for patients with minor head injury (4, 11, 12). These studies did not focus exclusively on intoxicated patients and their cohort only consisted between 6% to 35% of intoxicated patients. The American College of Emergency Physicians clinical policy include alcohol intoxication as an indication for CT acquisition after minor head injury with loss of consciousness or amnesia (13). A prospective cohort study by Easter et. al compared sensitivities between the Canadian CT Head rule, National Emergency X-Radiography Utilization Study (NEXUS), and New Orleans Criteria and found that the Canadian CT Head Rule and the NEXUS criteria do not have adequate sensitivity to be applied in intoxicated patients with minor head injury, even though none of the patients required neurosurgery intervention. In their study, they found loss of consciousness and headache to be significantly associated with traumatic intracranial injury in intoxicated patients (14). Can we delay imaging for intoxicated patients presenting with altered mental status (AMS) and possible ICH? No prospective study as shown we can, but a retrospective chart review by Granata et al suggests that deferring CT imaging while monitoring clinical status is a safe emergency department practice (15). In their study, neurosurgical intervention was required in only one patient in the group with CT scans deferred for more than 180 minutes and even then, the procedure was not performed emergently, but instead the following day. However, their study lacked follow up of patients discharged home without CT imaging and the use of CT order time rather than CT acquisition time. The decision to obtain CT in intoxicated patients with minor head trauma can often be difficult and the physician should use clinical gestalt along with frequent monitoring for improvement of mental status if CT is deferred.
Given the presentation of AMS in alcohol-intoxicated patients and the lack of history including the mechanism of their trauma, cervical spinal immobilization must be performed until cleared. Not to mention, AMS or intoxication disqualifies trauma patients from clinical spine clearance and therefore, radiographic imaging with computed tomography (CT) of the cervical spine is performed (16, 17). Injuries to the spine and/or spinal cord are relatively uncommon, with the incidence of cervical spinal injuries in trauma ranging from 2.0% to 5.0% (18, 19, 20). A prospective cohort study of 250,000 patients, found 3.5% (8,871) patients suffered from cervical spine trauma. Of this, 23.3% (2,069) suffered a cervical cord injury with or without a fracture/dislocation, of which 1.4% (30) suffered multiple level cord injury, involving the cervical cord (21). Despite a normal CT scan, the concern for a missed unstable ligamentous injury has led to protocols within many institutes recommending clinically reassessment of the c-spine after sobriety or progressing to MRI. However, does further radiologic examination with MRI add anything or alter treatment? Many published articles have demonstrated MRI does not disclose any additional information beyond multidetector CT scanning in identifying unstable cervical spine injuries (22, 23, 24). Some would argue that high-quality CT imaging should pick up injuries that are mechanically unstable and could potentially be exacerbated by premature c-collar removal and that the presence of gross motor function of all extremities combined with a negative CT scan successfully rules out an unstable injury without the need for additional imaging (25, 26). Prolonging immobilization and cervical collar wear which can often be a few days before MRI imaging has potential adverse effects and consequences. Pressure ulcerations, increased intracranial pressure, and decrease pulmonary volumes have been shown to be affected by cervical collar wear (27, 28, 29). Recently, the Western Trauma Association in their prospective multicenter study between 2013-2015 involving over 10,000 patients throughout 17 centers, evaluated the incidence and type of cervical spine injuries, the accuracy of CT scan and the impact of intoxication on the time of cervical spine clearance in blunt trauma patients. They report that a high-quality negative CT scan is highly accurate and reliable for ruling out a clinically significant injury and has a 100% negative predictive value for identifying unstable injury that could result in harm with discontinuation of spinal precautions (30). This will allow us to avoid associated morbidity, cost and inconvenience of prolonged immobilization.
Informed Consent, Refusal of Care, and AMA
Self-discharge of intoxicated patients signing against medical advice is always a difficult and not a straightforward decision. The decision depends on whether the patient lacks capacity and on how the patient arrived to the hospital. If the physician believes the intoxicated patient lacks capacity, you are in the right to act in the patient’s best interests, in situations of necessity (emergent situations), and in the duty of care in caring for all patients, to do what is immediately necessary even without the patient’s consent (31). Now if the patient voluntarily came to the hospital, was clearly intoxicated, but wants to sign AMA or leave, this person can leave even if capacity is limited by his intoxication. An example of a similar case is found in Kowalski vs St. Francis Hospital and Health centers (32, 33). In this scenario, even the Mental Hygiene Law Section 22.09 would only apply “If the person comes voluntarily or is brought with his or her objection…If the person is incapacitated by alcohol and/or substances to the degree that there is likelihood to result in harm to the person or others, he or she may be retained to receive emergency services and shall be regularly reevaluated to confirm continued incapacity by alcohol and/or substances to the degree that there is a likelihood to result in harm to the person or other. (34). “To restrain plaintiff on these facts would have exposed defendants to liability for false imprisonment (33).” Now if the patient is unfit to drive and is leaving the ED to drive home and despite voicing your concerns and attempting to reach family or friends, you may need to notify the police without giving any confidential medical information (such as diagnosis or laboratory tests results) (35). Ultimately, it is important for every hospital to have clear policies on discharging intoxicated patients based on local laws (36).
Discharge Recommendations
Several issues must be considered before discharging your intoxicated patient:
1) Current clinical condition and conduct.
2) Possible signs of alcohol withdrawal and delirium tremens.
3) Disposition of where and how the patient will be going.
4) Support network.
5) Follow up care.
Pearls
1) Begin with ABCs, bedside glucose level and possibly Naloxone if overdose suspected, expose patient for complete evaluation.
2) Remember there are both medical and trauma chameleons to alcohol intoxication.
3) Obtain alcohol level if diagnosis of alcohol intoxication is in question or if mental status is not improving after a few hours of observation.
4) If head trauma is minor, deferring CT brain may be reasonable with frequent monitoring, but use your clinical gestalt.
5) If CT C-spine is negative and no gross motor deficit on exam, cervical collar can be cleared.
6) Look to the hospital policy regarding disposition of intoxicated patients.
Falls from Height
Case
40-year-old female is brought in by EMS as a known jumper from a bridge. GCS 14, opens eyes to speech. Vital signs: 115 bpm, 100/75, RR 23, T98.3. Airway intact, breath sounds bilaterally. Patient has a clear deformity to the left lower extremity but no notable trauma to head, face and chest. Patient is exposed and rolled with manual traction to the left leg and there is no midline spinal tenderness or trauma appreciated to the back. Patient is screaming out in pain upon rolling her and is stating “my hips are killing me.” FAST negative. Does this patient also have a pelvic injury? Could she being have a life threatening pelvic or intra-abdominal bleed?
Background/Incidence
Falls account for the second most common cause of injury associated mortality after motor vehicle accidents. (13) Many of these injuries occur in work related accidents such as falls from ladders or scaffolding but is important to determine the intent (e.g. suicide) or circumstances surrounding the fall. OSHA data shows that of the construction industries causes of death, falls from height tops the “Fatal Four” (others being struck by objects, electrocutions and stuck-in-between injuries) and makes up 38.7% of work-related deaths.
Among these cases, the pattern of injury is most frequently blunt injury and the particular body system that absorbs this blunt injury heavily influence the morbidity and mortality as well as the individual injuries within that system. Turgut et. al. showed that age, fall height, fall place, linear skull fracture, subarachnoid hemorrhage, cervical fracture, thoracic vertebra fracture and trauma scores had statistically significant effect on mortality.

The height fallen, chest/head injuries and the old/young were amongst the highest group with mortality due to falls from height and thus should be variables considered when triaging and resuscitating these patients (6, 16).

Assessment
While collecting the information that surrounds the circumstance of the fall is important, our overall management follows ATLS algorithms for these patients and thus is fairly straightforward and familiar to all EM physicians. It is particularly important to understand the kinetics of this injury and how it relates to the point of impact. Vertical free fall injuries account for a majority of falls from height, especially in urban environments. Of these, urban falls tend to produce severe lower-extremity, spinal, and pelvic fractures (4).
Of note, falls from height may also be jumps from height and thus after stabilization these patients will require psychiatric evaluation. This population specifically has the highest rate of mortality, Roccos and Chesser showed that, “jumping requires no equipment and is easily carried out with little planning, and is likely to be fatal with 55% of patients dying either at the scene within an emergency department”. Furthermore, jumpers vs falls from height are more likely to have a more severe pattern of injury and thus there should be a higher index of suspicion for polytrauma as well as height jumped from (1).
Much like our patient in the case above, patients with falls from height that have a point of impact on their lower extremities will suffer severe orthopedic, vascular and neurologic injury. It is important to understand the transfer of kinetic energy from the jump to impact and how it is transmitted in a linear fashion along the musculoskeletal system thus contributing to a majority of long bone and spinal injuries. Below we will look at this pattern of injury in an organized system based manner.
Spine
The spine acts as a conduit of energy for falls when landing on the feet as well as direct impacts to the back. Prehospital care continues to manage patients in the field with long boards and cervical collars, more information on the data against such practices can be found on this great post by Dr. Joseph on emDocs from 2016. Special consideration should be paid towards the junctional zones of the spine including C7-T1 and T12-L1 as this is where the greatest amount of stress is sustained during motion (8). Furthermore, the thoracic region is the narrowest point of the vertebral column and thus at the highest risk for spinal cord injury. Much can be said about “stable” vs “unstable” vertebral fractures and while there is the classic teaching of unstable cervical fractures, in a fall from height patient it is best to consider all possible fractures unstable until further advanced imaging can be obtained.
Special considerations for spinal injuries:
- Airway control in high cervical injuries (i.e. C3-C5)
- C-spine stabilization during intubation.
- Video-assisted intubation over DL – Video assisted models have shown less cervical spine mobility (4).
- Hypotension
- Can be due to neurogenic shock, hemorrhage or tension pneumothorax so keep a broad differential.
- Treat with IV fluids or blood depending on suspicion of hemorrhage.
Head
For head injury, GCS is key but not king. Its power lies not in evaluating the acuity of an injury, but rather its progression over time. Obtain any changes in mental status from EMS. The patient with a GCS of 10 in front of you may have started as a GCS of 15 with EMS and thus could be trending in a dangerous direction. This type of presentation may conflict with the classic teaching of intubating for a GCS of 8. For specifics of neurocritical care intubation see EMCrit.
Assess pupillary response as a single, dilated, fixed pupil in an unconscious patient could indicate an intracranial bleed with impending herniation. These patients require rapid, surgical depression and may even benefit from an ED burr hole if indicated.
Finally, assess for decorticate vs decerebrate positioning as these are indicators for severe injury above the midbrain or more caudal injuries; respectively.
Pelvis
Pelvic injuries are a cause of significant morbidity and mortality in falls from height and especially so in jumps from height. Teh et. al showed that jumpers tend to fall feet first and to their dominant side thus sustaining greater lower extremity and pelvic fractures vs their fall from height counter parts (15). Thus, patients presenting with a known jump or more information on their mechanism of landing should lead clinicians to have a higher suspicion of pelvic fractures and their sequelae.
Testing for laxity or instability should be performed with GENTLE downward and medial pressure at the iliac wings (2). In trauma, patients care should be made to perform this test a single time and possibly waiting until the trauma team is available to avoid unnecessary repeat manipulation of an unstable pelvic fracture (2). The theory is that manipulation can dislodge any clot formation resulting in worsening incompressible hemorrhage. More current literature shows that manual rocking is dangerous, and its sensitivity is as low as 8% (9). Any positive findings should prompt early pelvic binder application prior to radiologic confirmation. For those with EMRAP access there is a great video from their EM:RAP HD series showing the appropriate positioning and placement of a pelvic binder. As shown in the video, care should be taken to place a sheet or commercial binder at the level of the greater trochanter in order to maximize stabilization. This leads to decrease pelvic volume size, venous hemorrhage tamponade and prevention of secondary hemorrhage from the shearing forces of fractures. Ultimately there are two main dispositions for these patients assuming there aren’t other more pressing injuries; OR for preperitoneal packing or IR suite for angioembolization. The latter is dependent on how quickly IR is available, the IR capabilities of your center and the stability of your patient.
It is important to consider the surrounding structures that may be injured as the pelvis acts as a vessel for vasculature, GI, and GU structures (8). It is not uncommon to have concomitant urogynecological, rectal, neurologic injury (2). Injury patterns such as blood per rectum, blood at the urethral meatus or perineal bruising can increase your suspicion for pelvic fractures (3). Most of these injuries will be addressed in the secondary or tertiary survey of hypotensive trauma patients or may be delayed presentations.
Thorax/Abdomen
Chest and abdominal trauma follow TBI as the second leading cause of immediate death in fall from height victims (10). Chest trauma especially, including hemo/pneumothorax, contributed to worsening outcomes in those with TBI due to limited chest excursions and lung tissue compression causing decompensated hypoxia (10). Abdominal trauma tended to be the leading cause of hemodynamic disturbances due to visceral organ hemorrhage, with hollow viscous organs being the more typical pattern in blunt injury (7).
FAST exam as a bedside screening tool for injury in these regions offers time sensitive confirmation and is an accepted indication for emergent laparotomy in hemodynamically unstable fall patients.
Indications for Emergent Laparotomy
- Absolute
- Anterior abdominal injury with hypotension
- Abdominal wall disruption
- Peritonitis
- Free air under diaphragm on CXR
- Positive FAST or DPL in hemodynamically unstable patients
- CT-diagnosed injury requiring surgery
- Relative
- Positive FAST or DPL in hemodynamically stable patients
- Solid visceral injury in stable patients
- Hemoperitoneum on CT without an obvious source
REBOA
A new intervention gaining worldwide attention over approximately the past decade is REBOA (resuscitative endovascular balloon occlusion of the aorta). This intervention includes accessing the aorta via the femoral artery and passing a balloon using the Seldinger technique into one of three zones of the aorta. Inflation of a balloon at the end of the catheter tip provides hemorrhage control for intra-abdominal/pelvic injuries. EMCrit’s Scott Weingart has a podcast from 2014 with an accompanying written walkthrough on this technique. The presumed benefit for REBOA is largely when compared to the morbidity associated with survived resuscitative thoracotomies (RT) for similar indications. A meta-analysis of REBOA vs cross-clamping the aorta in resuscitative thoracotomy performed by Manzano et. al showed that the odds of mortality were no different between the two groups but sensitivity analysis showed that the mortality risk was significantly lower in those undergoing REBOA. Undoubtedly, this area of damage control resuscitation requires further inquiry and by no means is a silver bullet for the hemodynamically unstable trauma patients. One major bias is that RT is utilized as a “last-ditch” effort while REBOA is commonly utilized earlier in the disease course due to being less-invasive. As more data comes to light and more hospitals begin utilizing this intervention the topic will be worth circling back to in the future.
Pearls
- Heights of falls/jumps are important information for your primary survey.
- Follow ATLS and you won’t miss major injuries.
- Know the specific patterns of injury you expect by system and know how to troubleshoot them (i.e. FAST, pelvic binder, REBOA).
- SLOW IS SMOOTH AND SMOOTH IS FAST. Your job is to resuscitate and stabilize. These patients will need you in their resuscitation and then likely will go on to receive advanced endovascular or surgical intervention.
References/Further Reading:
“Geriatric” Resources
- Barry E, Galvin R, Keogh C, Horgan F, Fahey T. Is the Timed Up and Go test a useful predictor of risk of falls in community dwelling older adults: a systematic review and meta- analysis. BMC Geriatrics. 2014;14:14.
- Burns E, Kakara R. Deaths from Falls Among Persons Aged ≥65 Years — United States, 2007–2016. MMWR Morb Mortal Wkly Rep 2018;67:509–514.
- Coleman J, Baldawi M, Heidt D. The effect anticoagulation status on geriatric fall trauma patients. Am J Surg.2016 Dec;212(6):1237-1242.
- Martin JT, Alkhoury F, O’Connor JA, et. al. Normal’ vital signs belie occult hypoperfusion in geriatric trauma patients. Am Surg 76: 65, 2010.
- McCammack K.C. Sadler, C., Guo Y. Routine repeat head CT may not be indicated in patients on anticoagulant/antiplatelet therapy following mild traumatic brain injury. West J Emerg Med.2015 Jan;16(1):43-9.
- Nishijima DK, Offerman SR, Ballard DW, et al. Immediate and Delayed Traumatic Intracranial Hemorrhage in Patients With Head Trauma and Preinjury Warfarin or Clopidogrel Use. Annals of Emergency Medicine, Volume 59, Issue 6, 460 – 468.e7.
- Samaras N, Chevalley T, Samaras D, et al. Older Patients in the Emergency Department: A Review. Annals of Emergency Medicine, Volume 56, Issue 3, 261 – 269.
- Stevens JA, Mack KA, Paulozzi LJ, et. al. Self-reported falls and fall-related injuries among persons aged >65 years—United States, 2006. MorbidMortal Wkly Rev 57: 225, 2008.
- Fleischman RJ, Ma O. Trauma in the Elderly. In: Tintinalli JE, Stapczynski J, Ma O, Yealy DM, Meckler GD, Cline DM. eds. Tintinalli’s Emergency Medicine: A Comprehensive Study Guide, 8e New York, NY: McGraw-Hill; 2016.
- WISQARS leading causes of death reports, 1999-2009, National Center for Injury Prevention and Control, US Centers for Disease Control. Accessed July 21, 2012. http://webappa.cdc.gov/sasweb/ncipc/leadcaus10_us.html
“Intoxicated” References
- White AM, Stater ME, Ng G, Hingson R, Breslow R. Trends in Alcohol-Related Emergency Department Visits in the United States: Results from the Nationwide Emergency Department Sample, 2006-2014. Alcoholism: Clinical and Experimental Research. 2018 pp1-8
- Mullins PM, Mazer-Amirshahi M, Pines JM. Alcohol-related visits to US Emergency Departments, 2001-2011. Alcohol and Alcoholism. 2017; 52(1): 1-7
- Hoffman JR, Wolfson AB, Todd K, Mower WR. Selective cervical spine radiography in blunt trauma: methodology of the National Emergency X-Radiography Utilization Study (NEXUS). Ann Emerg Med.1998;32(4): 461-9
- Haydel MJ, Preston CA, Mills TJ, et al. Indications for computed tomography in patients with minor head injury. N Engl J Med. 2000;343(2): 100-5
- Bennett, Joe, and Hillary Fairbrother. Alcohol Intoxication Mimics: ED DDx Approach to Management. EmDOCs, 30 Aug. 2017. www.emdocs.net/alcohol-intoxication-mimics-ed-ddx-approach-management/.
- Uribe, Jeffrey, and Muhammad Waseem. Medical Emergencies Disguised as Trauma, or Trauma Chameleons. emDocs, 11 June 2018. www.emdocs.net/medical-emergencies-disguised-as-trauma-or-trauma-chameleons/.
- Hubler, James R, et al. Management of the Intoxicated Patient in the Emergency Department. Relias Media, 1 Jan. 1998. www.reliasmedia.com/articles/35285-management-of-the-intoxicated-patient-in-the-emergency-department.
- Simel DL, Feussner JR. Does determining serum alcohol concentrations in emergency department patients influence physicians’ civil suit liability? Arch. Intern. Med. 1989;149 (5): 1016-8.
- Hubler, James. Are Blood Alcohol Levels Needed for Intoxicated Patients? Relias Media, 1 Nov. 2007. www.reliasmedia.com/articles/107392-are-blood-alcohol-levels-needed-for-intoxicated-patients?utm_source=TrendMD&utm_medium=cpc&utm_campaign=AHC_Media_TrendMD_0?utm_source=TrendMD&utm_medium=cpc&utm_campaign=AHC_Media_TrendMD_0.
- Pizon AF, Becker CE, Bikin D. The clinical significance of variations in ethanol toxicokinetics.” Journal of medical toxicology. 2007; 3(2): 63-72.
- Stiell IG, Wells GA, Vandemheen K, et al. The Canadian CT Head Rule for patients with minor head injury. Lancet. 2001; 357:1391–6.
- Mower WR, Hoffman JR, Herbert M, et al.; NEXUS II Investigators. Developing a decision instrument to guide computed tomographic imaging of blunt head injury patients. J Trauma. 2005; 59:954–9.
- Jagoda AS, Bazarian JJ, Bruns JJ, et al. Clinical policy: neuroimaging and decision making in adult mild traumatic brain injury in the acute setting. Ann Emerg Med. 2008; 52:714–8.
- Easter JS, Haukoos JS, Claud J, et al. Traumatic intracranial injury in intoxicated patients with minor head trauma. Acad Emerg Med. 2013; 20(8):753-60.
- Granata Robert T., Castillo Edward M., Vilke Gary M., Safety of Deferred CT Imaging of Intoxicated Patients Presenting with Possible Traumatic Brain Injury, American Journal of Emergency Medicine 2017 Jan; 35(1):51-54.
- Stiell IG, Wells GA, Vandemheen KL, et al. The Canadian C–spine rule for radiography in alert and stable trauma patients. JAMA 2001; 286:1841–8
- Hoffman JR, Wolfson AB, Todd K, Mower WR. Selective cervical spine radiography in blunt trauma: methodology of the National Emergency X-Radiography Utilization Study (NEXUS). Ann Emerg Med 1998; 32:461–9.
- Grossman MD, Reilly PM, Gillett T, Gillett D. National survey of the incidence of cervical spine injury and approach to cervical spine clearance in U.S. trauma centers. J Trauma. 1999; 47(4):684-90.
- Milby AH, Halpern CH, Guo W, Stein SC. Prevalence of cervical spinal injury in trauma. Neurosurg Focus. 2008; 25(5):E10.
- Goldberg W, Mueller C, Panacek E, Tigges S, Hoffman JR, Mower WR, Group N. Distribution and patterns of blunt traumatic cervical spine injury. Ann Emerg Med. 2001; 38(1):17-21.
- Hasler RM, Exadaktylos AK, Bouamra O, et. al., Epidemiology and predictors of cervical spine injury in adult major trauma patients: a multicenter cohort study. J Trauma Acute Care Surg. 2012; 72(4):975-81
- Chew BG, Swartz C, Quigley MR, et. al., Cervical spine clearance in the traumatically injured patient: is multidetector CT scanning sufficient alone? Clinical article. J Neurosurg Spine. 2013; 19(5):576-8
- Muchow RD, Resnick DK, Abdel MP, Munoz A, Anderson PA. Magnetic resonance imaging (MRI) in the clearance of the cervical spine in blunt trauma: a meta-analysis. J Trauma. 2008; 64(1):179-89.
- Hogan GJ, Mirvis SE, Shanmuganathan K, Scalea TM. Exclusion of unstable cervical spine injury in obtunded patients with blunt trauma: is MR imaging needed when multi-detector row CT findings are normal? Radiology. 2005; 237:106 –113.
- Como JJ, Diaz JJ, Dunham CM, et al. Practice management guidelines for identification of cervical spine injuries following trauma: update from the eastern association for the surgery of trauma practice management guidelines committee. J Trauma. 2009; 67(3):651-9.
- Schuster R, Waxman K, Sanchez B, et. al., Magnetic resonance imaging is not needed to clear cervical spines in blunt trauma patients with normal computed tomographic results and no motor deficits. Arch Surg. 2005; 140(8):762-6.
- Ackland HM, Cooper JD, Malham GM, Kossmann T. Factors predicting cervical collar-related decubitus ulceration in major trauma patients. Spine. 2007; 32:423– 428.
- Mobbs RJ, Stoodley MA, Fuller J. Effect of cervical hard collar on intracranial pressure after head injury. ANZ J Surg. 2002; 72(6):389-91.
- Ala A, Shams-Vahdati S, Taghizadieh A, et. al., Cervical collar effect on pulmonary volumes in patients with trauma. Eur J Trauma Emerg Surg: official publication of the European Trauma Society. 2016; 42(5):657-60.
- Martin MJ, Bush LD, Inaba K, et al., and the WTA C-Spine Study Group, Portland, Oregon. Cervical spine evaluation and clearance in the intoxicated patient: A prospective Western Trauma Association Multi-Institutional Trial and Survey. J Trauma Acute Care Surg; 83,6:1032-1040.
- Malone D, Friedman T., Drunken patients in the general hospital: their care and management. Postgraduate Medical Journal 2005; 81:161-166.
- Catherine GA, Crowley AR., Intoxicated patient in the emergency room, New York Physician. 2014; 4(5):20-21
- Kowalski vs St. Francis Hospital and Health Centers. NYC Courts, 26 June 2013.
- United States, Congress, Mental Hygiene. Emergency Services for Persons Intoxicated, Impaired, or Incapacitated by Alcohol and/or Substances. Emergency Services for Persons Intoxicated, Impaired, or Incapacitated by Alcohol and/or Substances, ser. 22.09. 22.09.
- Managing Intoxicated Patients in the Emergency Department. Why Good Documentation Matters, CMPA, Dec. 2009. www.cmpa-acpm.ca/en/advice-publications/browse-articles/2009/managing-intoxicated-patients-in-the-emergency-department.
- Simon, Jeremy. “Discharging Intoxicated Patients Requires a Clear Hospital Policy.” Ethics on Call, SAEM. saem.org/docs/default-source/saem-documents/education/ethicsoncalljuly-august.pdf?sfvrsn=e93224fd_2.
“Fall from Height” Resources
- Abel SM, Ramsey S. Patterns of skeletal trauma in suicidal bridge jumpers: a retrospective study from the southeastern United States.Forensic Sci Int. 2013 Sep 10; 231(1-3):399.e1-5.
- Barton MA, Derstine H, Barclay-Buchanan CJ. Pelvis Injuries. In: Tintinalli JE, Stapczynski J, Ma O, Yealy DM, Meckler GD, Cline DM. eds. Tintinalli’s Emergency Medicine: A Comprehensive Study Guide, 8e New York, NY: McGraw-Hill; 2016.
- Mahoney, Heather. Management of Major Pelvic Trauma. ALIEM, 19 July 2017, www.aliem.com/2017/07/management-major-pelvic-trauma/.
- Azia M. Use of video-assisted intubation devices in the management of patients with trauma. Anesthesiology Clinics. 31:157, 2013.
- Bruckman R, Buckman P. Vertical Deceleration Trauma: Principles of Management. Surgical Clinics of North America. 1991; 71(2): 331-344.
- Dickinson A, Roberts M, Kumar A, et al. Falls From Height: Injury and Mortality. Journal of the Royal Army Medical Corps 2012; 158:123-127.
- French L, Gordy S, Ma O. Abdominal Trauma. In: Tintinalli JE, Stapczynski J, Ma O, Yealy DM, Meckler GD, Cline DM. eds. Tintinalli’s Emergency Medicine: A Comprehensive Study Guide, 8e New York, NY: McGraw-Hill; 2016.
- Go S. Spine Trauma. In: Tintinalli JE, Stapczynski J, Ma O, Yealy DM, Meckler GD, Cline DM. eds. Tintinalli’s Emergency Medicine: A Comprehensive Study Guide, 8e New York, NY: McGraw-Hill; 2016.
- Hsu S-D, Chen C-J, Chou Y-C, Wang S-H, Chan D-C. Effect of Early Pelvic Binder Use in the Emergency Management of Suspected Pelvic Trauma: A Retrospective Cohort Study. International Journal of Environmental Research and Public Health. 2017; 14(10):1217.
- Khadjibaev AM, Sultanov PK, Kim H. Features of Patients Associated with Falls from Heights Admitted to Republican Research Center of Emergency Medicine. Journal of Trauma and Injury 2015; 28:248-255.
- Manzano Nunez R, Naranjo MP, Foianini E, et al. A meta-analysis of resuscitative endovascular balloon occlusion of the aorta (REBOA) or open aortic cross-clamping by resuscitative thoracotomy in non-compressible torso hemorrhage patients. World Journal of Emergency Surgery: WJES. 2017; 12:30. doi:10.1186/s13017-017-0142-5.
- Oguztürk H, Turgut K, Turtay MG, Sarihan ME, Gur A, Beydilli I, et al. Apricot tree falls: a study from Malatya, Turkey. Biomedical Research. 2016; 27(1):210–3.
- United States Department of Labor, OSHA. Fatal Occupational Injuries by Selected Characteristics. BLS Reports20014.
- Rocos B, Chesser TJ. Injuries in jumpers – are there any patterns? World Journal of Orthopedics. 2016; 7(3):182-187.
- Teh, J et al. Jumpers and Fallers: A Comparison of the Distribution of Skeletal Injury.Clinical Radiology, Volume 58, Issue 6, 482 – 486.
- Turgut K, Sarihan ME, Colak C, Güven T, Gür A, Gürbüz S. Falls from height: A retrospective analysis. World Journal of Emergency Medicine. 2018; 9(1):46-50.




