Author: Linda L. Herman, MD, FACEP (Kaweah Health Care District Emergency Medicine Program Director, Visalia, CA) // Edited by: Alex Koyfman, MD (@EMHighAK, EM Attending Physician, UTSW / Parkland Memorial Hospital) and Jennifer Robertson, MD, MSEd
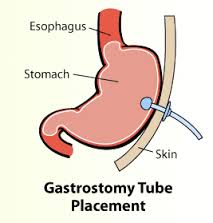
While working in the emergency department (ED), you note that the next patient to be seen has a chief complaint of “My G-tube fell out”. The patient’s vital signs are normal and he is triaged as a green. It is a very busy day in the ED and you consider skipping this patient for a few hours so that other, more ill patients can be seen. However, you remember that the G-tube should not be out for more than a two hours as even an established stoma can begin to close after this amount of time. If the replacement of the tube has to be delayed due to a preponderance of critically ill patients in the ED, then ask the nurse to place a same size Foley catheter in the stoma. The nurse does not even have to blow up the balloon. This will keep the stoma open until you have time to replace the tube.
This article will discuss how replace a G-tube or J-tube. It will also review how to remove and/or declog these tubes.
Methods
Replacing a G-tube should only take a few minutes, but taking an accurate history and performing a focused physical examination is important. The most important historical points are: (1) how long has the patient had a G-tube, (2) any problems with administering feedings or medications through the tube, (3) and how long has the G-tube been out. A new G-tube needs about 2 -3 weeks to form a tract. If the G-tube is new, notify the physician who placed it. Replacing a G-tube in a new site that has not formed a tract may cause separation of the stomach from the abdominal wall.
Next, inspect the site to make sure that there are no signs of infection around the tube. An abdominal exam should also be performed.
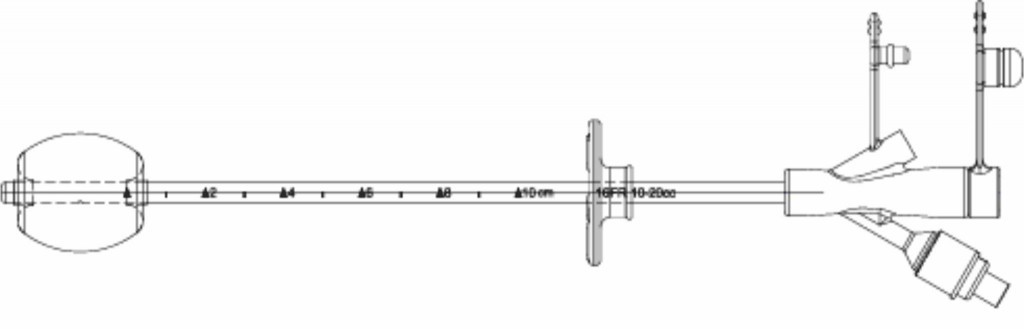
Replacing the tube requires the following equipment: clean gloves, G-tube (one same size and one or two that are smaller), lubricant, syringe to inflate the balloon, saline for the balloon, suture kit and suture (if you decide to suture in place), and tape.
Try to pick a G-tube that is most similar to the patient’s previous tube. There are several types on the market. Some hospitals only carry one or two brands and if the G-tube is similar in size it will work.
- Read the package instructions to determine the quantity of water or saline used to inflate the balloon.
- Open the package and check the balloon.
- Prepare the skin by washing with cleanser. (This is not a sterile procedure.)
- Lubricate the end of the G-tube and insert into the stoma using gentle pressure. Lidocaine jelly can be used to decrease the pain of insertion but there is no literature about the safety or efficacy of its use for this purpose.
- Insert until the outside buttress is against the skin and inflate the balloon and pull back to make sure that the G-tube is secure.
- Order an X-ray of the abdomen with 20-30 milliliters (ml) of gastrografin injected into the G-tube to check placement.
- Lower the buttress to the skin and either tape or suture in place.
If a G-tube has been out for several hours, its stoma may have already started to close. If this occurs, a smaller G-tube can be placed and/or dilation of the stoma can also be attempted using sequential red rubber catheters. Some healthcare providers use the curved forceps in a suture kit or the cap of an irrigation syringe to widen the stoma. The cap is tapered and blunt and will, therefore, not cause trauma. It should be noted, however, that none of these methods have been studied for safety or efficacy.

Too vigorous or aggressive work on the stoma should be avoided because the stomach may separate from the abdominal wall. To avoid this, insert a smaller tube to keep the stoma open and refer the patient to the specialist to have the appropriate gauge feeding tube placed.
Complications
Leaking G-tube:
There is no method to repair a leaking G-tube. Gather your equipment and then, using a syringe, deflate the balloon of the existing tube and remove with gentle traction. If the balloon does not deflate with aspiration using a syringe, then the balloon port can be cut to deflate the balloon. Replace the tube according to the directions above.
If a particular tube does not have a balloon, then it is likely that this tube is relatively new and was inserted percutaneously. These tubes each contain a silicone piece that helps keep the tube in the stomach while the stoma tract is maturing. There are products on the market with collapsible bumpers that allow you to remove these tubes with traction, but not all of these tubes can be removed this way. It is best to be familiar with the type of tube and if you have any questions about replacement, it should be discussed with the physician who placed the tube.
If a specialist is not available, the percutaneous endoscopic gastrostomy (PEG) tube can be severed with scissors at the abdominal wall and a new G-tube with a balloon can be placed. The silicone retention piece will then be eliminated through the GI tract. This usually occurs without difficulty, but on rare occasions in patients who have had previous abdominal surgeries, the retention piece causes a small bowel obstruction. Therefore, instructions to check the stool daily should be given to the patient and his or her caregivers. Also, patients should return if they develop abdominal pain, fever and/or vomiting.
Clogged G-tube:
The patient presents to the ED because feedings and/ or medication (s) cannot be given because the tube is clogged. It is important to determine what efforts were made at home to declog the tube. Although many myths abound about the use of meat tenderizer or carbonated beverages to declog a tube, these are not recommended. First, instill a small amount of warm water and use a back and forth motion to see if the clog can be dislodged. If not, put in a small amount of warm water and wait 20 minutes to see if will declog. Use a 30 to 60 ml syringe as to avoid excessive pressure when pushing fluid through the G-tube.
There is an enzyme solution on the market that can help in declogging a tube. This solution is called “Clog Zapper”TM , which is made by Copak Medsystems. The Clog Zapper comes in a kit that consists of a small tube that is placed into the G-tube to the level of the clog. The syringe in the kit is then filled with the enzyme material and reconstituted using 10 ml of water. The reconstituted enzyme solution is then injected into the small tube, the small tube is removed, and the solution is given 30 minutes to work. At the end of the 30 minutes, the G-tube is flushed with warm water.
Pancreatic enzyme supplementation has also been used to declog G-tubes. The only enzyme supplementation that can be used for this is Viokace® because the tablet needs to be crushed and mixed with water. It is recommended to mix a crushed Viokace® tablet with 1/8 teaspoon of baking soda or a 324 milligram (mg) non-enteric-coated sodium bicarbonate tablet with 5 ml of water. Inject the solution into the G-tube and wait for 30 minutes before attempt to withdraw or flush.
There are three mechanical decloggers that are available on the market: Bionix Enteral Feeding Tube DeClogger®, the Bard® PEG Cleaning Brush, and TubeClear® System. The Bionix DeClogger® is a plastic device with a treaded end that is made to clear multiple feeding tubes in sizes 14 to 24 French (Fr) . The device is inserted in the G-tube and twisted to break up the clog.
*Bionix Enteral Feeding Tube DeClogger®


*Pictures reproduced with permission from Bionix ®Medical Technologies
The Bard® PEG feeding tube cleaning brush is a brush that is inserted into the G-tube and used to clean the G-tube and break up the clog. The brush should not be used during the first 14 days after insertion and cannot be used in anything smaller than an 18 Fr catheter. Forceful cleaning can result in entrapment or breakage and should absolutely be avoided.
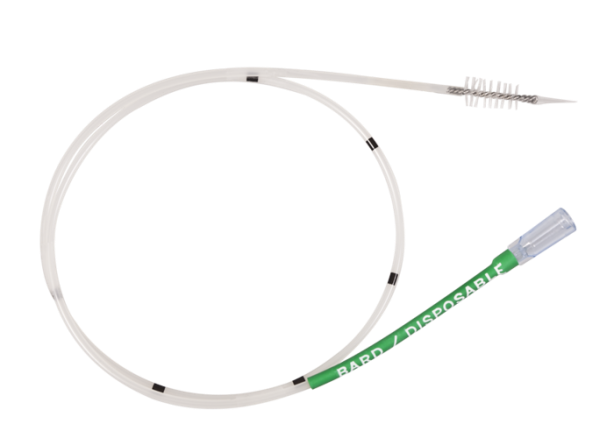
© 2016 C. R. Bard, Inc. Used with permission
The TubeClear® System can be used on G-tubes size 10 to 18 Fr in adult patients. The System is comprised of a re-usable Control Box and a single use Clearing Stem. One end of the Clearing Stem is attached to the Control Box and the other end is inserted into the G-tube. The mechanical motion of the Control Box actuates the Clearing Stem Wire Tip as it is advanced through the tube to actively work on and remove the clog.

Copy with permission from TubeClear®
Displacement of tube into the peritoneal cavity:
The most serious complication with any G-tube or Jejunostomy (J) tube complication is peritonitis from inadvertently inserting the tube into the abdominal cavity. This is rare but has a high rate of morbidity and mortality. That is why it is so important to check the placement of the tube before discharging the patient from the ED. Unfortunately, many patients who have G-tubes are non-verbal and are unable to alert the healthcare provider by complaining of abdominal pain. Also, elderly patients may not have a rigid abdomen when peritonitis is present. The possibility of peritonitis from enteral feedings entering the abdominal cavity should be considered in the differential of a febrile patient with a G-tube or J-tube. The method for evaluating this possibility is an abdominal radiograph after the instillation of gastrografin through the G- or J-tube. This should be one of the first considerations when a febrile patient with a G or J-tube comes to the ED and should be done in conjunction with other tests that evaluate for fever, such as urinalysis and a chest x-ray.
J-tubes
These are similar to gastrostomy tubes but they are of a smaller diameter and are placed into the small bowel. Feedings given through these tubes are continuous instead of bolus. They also form a tract over time but can close easily when the tube is removed. The replacement procedure is the same as the G-tube. Most G-tubes will be too big to use to replace a J-tube unless they are of pediatric size. If no J-tube is available, a pediatric feeding tube or urinary catheter of a similar gauge can be used as a replacement to keep the stoma open until one can be obtained. Also, the placement should be checked with gastrografin before instilling any fluids into the J-tube.
Pearls
–The sooner the G- or J-tube is replaced, the easier the placement will be.
–Gather all equipment necessary for the placement (expect that it will not go in) so that you will be prepared if the insertion is difficult.
–Familiarize yourself with the tubes that you are both replacing and inserting
–Always check placement with an abdominal x-ray with gastrografin before using the replaced G-tube.
–Several methods are available to declog a G- or J-tube. Ask if any are available at your institution.
-Consider peritonitis as an etiology for fever in any patient with a G- or J-tube.
References/Further Reading
–http://www.bcchildrens.ca/health-info/coping-support/tube-feeding
–http://www.tubeclear.com/tubeclear-support/
–http://www.bionixmed.com/MED_Pages/DeClogger_Features.html
–http://www.bardpv.com/portfolio/percutaneous-endoscopic-gastrostomy-peg-accessories/
-Fisher C, Blalock B. “Clogged Feeding tubes: A Clinician’s Thorn.” Practical Gastroenterology 2014 March;37(3):16.





