
Authors: Brit Long, MD (@long_brit, EM physician at SAUSHEC, USAF) and Barry Sheridan, DO (EM Staff Physician and Professor at SAUSHEC) // Edited by: Alex Koyfman, MD (@EMHighAK, EM Attending Physician, UTSW / Parkland Memorial Hospital) & Justin Bright, MD (@JBright2021)
Case:
A 42–year-old male presents with dull chest pain for 4 hours, which worsens with exertion. He has a history of hypertension, and he does not smoke. His VS are normal, as is the physical exam and ECG. He has no risk factors for PE or dissection, and the chest xray is normal as well. Your first troponin comes back negative. What is this patient’s disposition? Is there any way to avoid admitting or placing this patient into the observation unit for stress testing?
Background:
Clinical decision rules (CDR) can improve decision-making in specific situations in the ED, potentially decreasing further testing and improving disposition times. This part of the CDR series will look in detail at a current clinically significant CDR and pathway – The HEART pathway.
Part one of this series listed the essentials a CDR should possess: answers a relevant question, addresses a common clinical problem, appropriately derived, externally validated, improves clinical practice, applicable to practice and patients, and ease of use. http://www.emdocs.net/clinical-decision-rules-part-1/
Part two examined applying a CDR to actual clinical practice, which involved several steps: determining the rule that would most affect patient care in your setting, identify obstacles to implementation (provider and institution), achieving buy-in (from all members of the team including nurses and other specialties/consultants), publicizing pathway use, and monitoring and refinement of the rule once in place. http://www.emdocs.net/clinical-decision-rules-part-2/
Part 3 will evaluate actual risk of missed MI in chest pain patients, followed by a look at several clinical rules and pathways.
Risk:
Chest pain accounts for 10% of ED visits. Up to 10 million visits per year and $10 to $12 billion per year in healthcare expenditures are due to chest pain.1-6 The etiology of these presentations can range from benign to life-threatening, and ACS is a major concern. Many of these patients do not possess a cardiac etiology, and patients lacking evidence of ischemia demonstrate low risk of adverse outcomes.1,5,6 However, the ED evaluation of chest pain can present significant medicolegal risk. Approximately 20% of lawsuits are due to diagnosis and management of ACS, and missed myocardial infarction (MI) is one of the highest costs to insurers.2,7-10
The true rate of misdiagnosis approximates 0.2%, rather than the commonly quoted 2% from a study by Pope et al. in 2000.2 In 1996, Goldman et al. suggested that patients without hypotension, heart failure, known prior myocardial infarction, or worsening chest pain had less than 1% risk of death, need for revascularization, or acute coronary syndrome.11 A recent 2015 article by Weinstock et al. found that with two negative troponin tests and nonischemic ECG, the primary outcome of adverse cardiac event occurred in 0.18% of admissions.12
Clinical decision rule/pathways:
Several clinical decision aids have been developed with the intent of risk stratification for chest pain. The objective of these aids is to place patients into risk categories based on a combination of separate factors, allowing proper selection for discharge, further testing, or intervention. A sensible, safe, and consistent pathway can assist with appropriate disposition, while minimizing patient harm. The first decision aid was published in 1982 by Goldman et al. using a computer-based algorithm.13 This pathway addressed diagnosis of MI and need for cardiac care unit (CCU) admission.13 Later investigators have sought an aid to appropriately risk stratify patients appropriate for discharge. This review will examine several of the most commonly utilized decision aids.
Thrombolysis In Myocardial Infarction (TIMI) score
The TIMI score was first published in 2000, followed by validation in 2006.14 Initial studies evaluated patients at high-risk for unstable angina and non-ST-elevation MI. This score incorporates several elements based on a 7-point scale, shown below.15-17 Scores of 0-1 points result in a 4.7% risk of ACS, while scores of 6-7 are associated with 40.9% risk.15-18 Validation in separate cohorts demonstrated similar rates of increasing risk for cardiac outcomes with increasing TIMI score. Sanchis et al. proposed a risk score based on the original TIMI score with troponin, with a primary outcome of death or AMI within one year.19 A small subset of the evaluated population, 17%, were deemed very low risk based on a score of 0. However, patients categorized as low risk demonstrated a 1 year adverse event rate of 3.1%.19
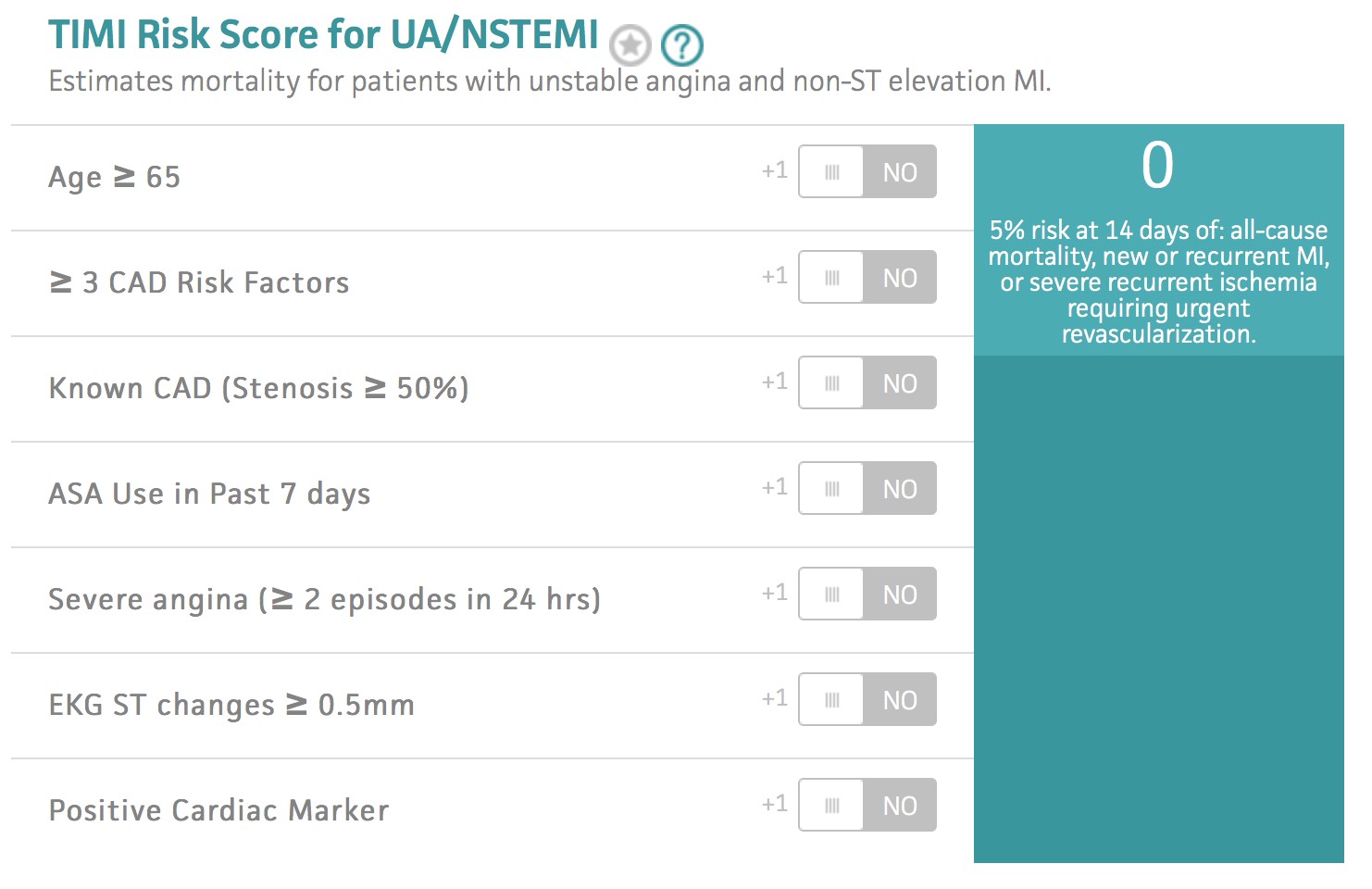
Several flaws affect this decision aid. A score of 0 does not risk stratify below 1%, and a score of 0 is not common. 10% to 20% of patients were stratified as low risk based on scores 0-1.15-18 Aspirin use alone provides a score of 1. This decision aid was not derived for the undifferentiated chest pain population in the ED, but rather to determine which patients would benefit from early invasive therapy. Chase in 2005 evaluated TIMI in an ED population of undifferentiated chest pain patients.15 The cohort consisted of 1,458 patients, with 136 adverse events. Eight adverse events occurred over 30 days, or 1.2%, with mortality 0.2%. 15 Pollack et al. found a 2% MACE rate at 30 days with TIMI 0.16 Hess et al. found insufficient sensitivity with TIMI use in 17,265 patients.18 Unlike other decision aids and scores, the TIMI score does not stratify patients into discrete groups, and parts of the score are subjective, most importantly the presence of severe angina. The use of this score for risk stratification does not have appropriate characteristics to discharge patients from the ED.18,20,21
Modified TIMI
The modified TIMI score was designed for ED use based on four variables: elevated cardiac biomarker, age > 65 years, ischemic ECG changes, and history of CAD. In one study of 947 patients with chest pain, the modified TIMI had similar predictive capability as the original TIMI. The same flaws exist with use of the modified score, as the MACE rate is 2.4% in the lowest risk category.22
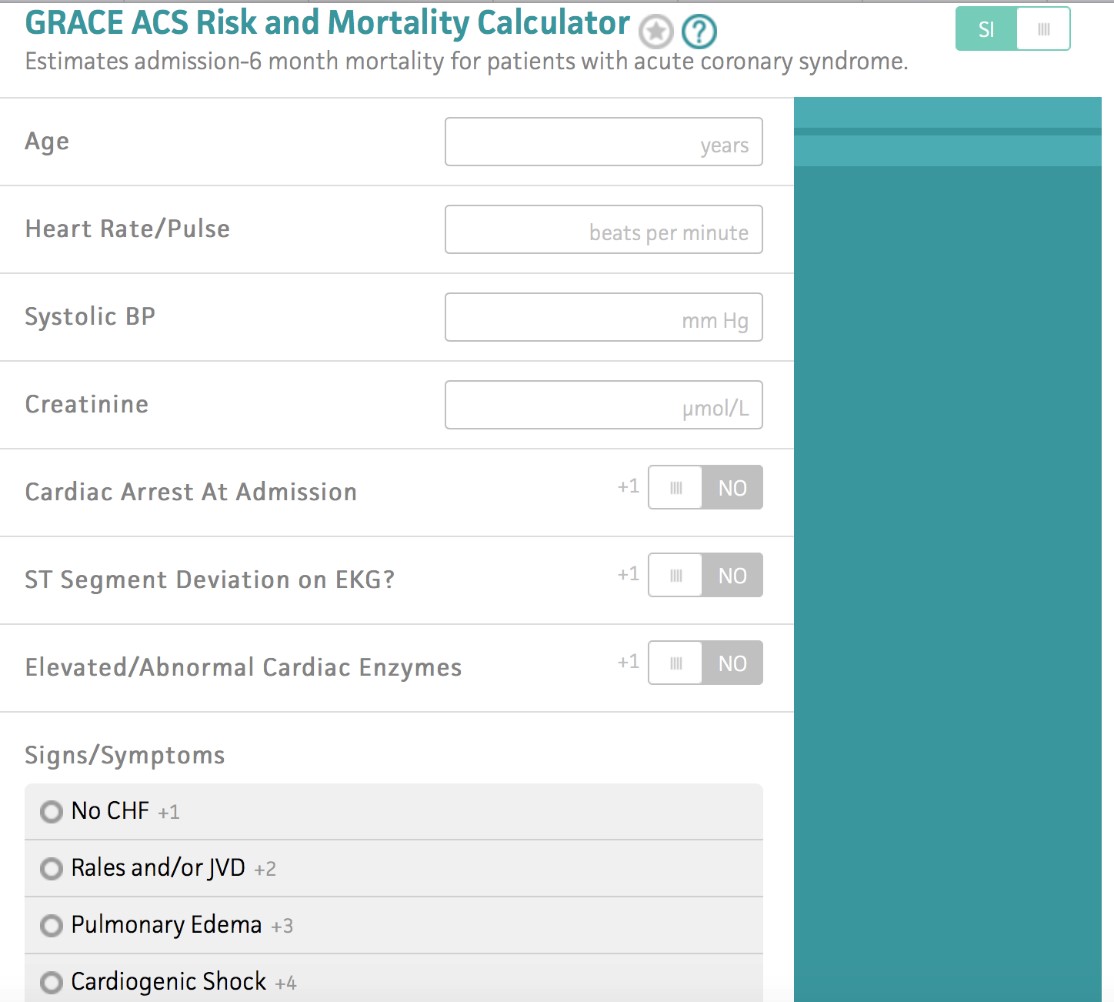
Global Registry of Acute Coronary Events (GRACE) score
The Global Registry of Acute Coronary Events (GRACE) score, developed in 2003, is accurate in predicting in-hospital, 3 month, and 6 month mortality in ACS.20,21,23,24 The score relies on 8 variables from history, examination, ECG, and laboratory tests, each given a specific weighted score based on predictive value, shown below. It has been externally validated.22 Rates of adverse cardiac events significantly increase as the score rises, ranging from 0.2% for scores less than 60 to above 52% for scores greater than 250. Subsequent evaluations of the score have demonstrated that patients with scores ranging from 0-60 still have a 2.9% risk of adverse coronary event within 30 days.21,23,24 The score is difficult to use in the ED, it does not stratify patients into separate risk categories, and it was not designed to assess undifferentiated chest pain.20,21
The Heart Score
The HEART score has gained popularity in recent years due to its ease of use, applicability, and multiple validations. Not only has the score demonstrated ability to stratify patients into low risk appropriate for discharge, but also those patients at high risk and need for possible intervention.21,25-28 It consists of several components, demonstrated below. The original score used Troponin > 2X normal limit, rather than 3X. Patients with scores 0-3 are low risk (appropriate for discharge), 4–6 moderate risk (appropriate for admission/observation), and > 7 high risk (consideration of intervention). 21,25-28 The original derivation study utilized 122 patients in 2008, evaluating for the primary outcome of acute myocardial infarction (AMI), percutaneous coronary intervention (PCI), coronary artery bypass graft (CABG) and death plus a combined endpoint of AMI, PCI, CABG and death.26 Of low risk patients, 2.5% experienced an adverse coronary outcome.26 Of high risk patients, 72.7% experienced an adverse event. Following derivation, the score was externally validated.96 A study in 2010 found a rate of 0.99% in 303 low risk patients, with adverse events occurring in 65.2% of high risk patients.27 One study in 2013 found a 1.7% event rate in patients stratified to low risk, with 50.1% high risk patients experiencing adverse event. Use of this score dropped admissions by at least 20%, while maintaining negative predictive values of > 99% at 30 days.27,28 A recent JAMA publication found low risk HEART scores possess a 0.20 LR for ACS (95% CI, 0.13-0.30), while the patients categorized as high risk had a 13 LR (95% CI, 7.0-24) for ACS.29
HEART Score
| Component | Grading | Score |
| History | Highly suspicious
Moderately suspicious Slightly or non-suspicious |
2
1 0 |
| ECG | Significant ST-depressions
Nonspecific repolarization disturbance Normal |
2
1 0 |
| Age | > 65 years
45-64 years < 45 years |
2
1 0 |
| Risk factors | > 3 risk factors, or history of CAD
1-2 risk factors No known risk factors |
2
1 0 |
| Troponin | > 3X normal limit
> 1 – < 3X normal limit < Normal limit |
2
1 0 |
Several aspects of this score must be considered. The first involves troponin, as one elevated troponin with no other points provides a score of 2. Dynamic ECG changes with no other points provide a score of 2 as well. The third factor deals with risk factors, as the patient who has no past medical history on record may have undiagnosed hypertension, hyperlipidemia, or diabetes.
These scores have been compared in several studies. One investigation compared GRACE, TIMI, and HEART scores. In this study, 34% of the study with a TIMI 0-1 had a 2.8% rate of MACE at 6 weeks, 14% had a GRACE 0-60 with an adverse rate of 2.9%, and 36.4% had HEART 0-3 with adverse rate of 1.7%.30 Sun in 2015 compared TIMI and HEART scores; a HEART score 0-3 had a NPV 98.2% (95% CI: 0.978-0.986) and c-statistic of 0.753, while TIMI 0 had NPV of NPV 97.8%, 95% CI: 0.971-0.983) c-statistic 0.678.31 Sun recommended the HEART score, which has better discrimination and outperforms TIMI within low-risk categories.31 A review in 2011 comparing TIMI, GRACE, HEART, and PURSUIT scores recommended HEART due to its ease of use, greater ability to categorize patients, and greater accuracy in stratifying patients to low risk.21
Chest Pain Pathways
Accelerated diagnostic protocol (ADP) use has the potential to identify low risk chest pain patients appropriate for discharge. Several trials have utilized repeat troponin testing with TIMI. The ASPECT trial conducted in 2011 identified low risk patients defined by TIMI 0, ECG without new ischemic changes, and negative point of care biomarker at 0 hr and 2 hr.32 The primary outcome was major adverse cardiac event (MACE) within 30 days. Approximately 10% of patients were low risk, and of these 352 patients, 3 experienced MACE. This provided a sensitivity of 99.3% and NPV of 99.1%.32 The new improved ADP evaluated patients utilizing the ASPECT trial definition for low risk.33 Investigators compared this definition with a new edition based on modifications: troponin I at 0 hr and 2 hr, high sensitivity troponin T at 0 hr and 2 hr, and patients with a TIMI 1 and negative biomarkers. Of the 1,000 patients, 123 were low risk (12.3%). Two of 123 patients experienced ACS at 30 days. All pathways demonstrated similar sensitivities except for the group with TIMI 1, where sensitivity was 97%. However, the amount of patients categorized as low risk reached 19.7%.33 The ADAPT trial in 2012 used normal ECG, TIMI score of 0, and two negative troponin I at 0 hr and 2 hr.34 This study consisted of 1,975 patients, of which 302 patients experienced MACE. Of 392 patients meeting criteria for low risk, 1 patient experienced MACE, for a sensitivity of 99.7% (95% CI 98.1% to 99.9%) and NPV of 99.7% (95% CI 98.6% to 100.0%).34
Mahler et al. in 2015 attempted to validate the ADAPT trial in the U.S. using secondary analysis of 1,140 patients with TIMI 0-2, negative ECG for ischemia, and negative biomarkers.35 MACE occurred in 2.7% of the population, which is lower than prior studies. However, this use of the ADP in this trial identified 48.3% of the population for early discharge, with 0.9% of the patients experienced MACE within 30 days. Sensitivity for MACE was 83.9% in this study.35
Utilizing the HEART pathway can drop MACE to approximately 1% using the HEART score with 0 hr and 3 hr troponin testing.25,28 This pathway categorizes patients into separate categories based on HEART score. Those patients who are low risk undergo repeat troponin testing at 3 hr. If negative repeat troponin, the patient is appropriate for early discharge and encouraged to follow up with their primary physician. If the patient is moderate to high risk or has an elevated troponin above the 99th percentile threshold, the HEART Pathway recommends further evaluation (objective cardiac testing) in the hospital or observation unit (OU). The first study evaluating this pathway included 1,070 patients in an ED-based observation unit.25,28 The pathway demonstrated 100% sensitivity (95% CI 72% to 100%), with NPV 100% (95% CI 94.6% to 100%) for MACE, while identifying 82% of patients for discharge. Patients in this first cohort study did receive further testing.25,28 One validation study retrospectively investigated a multicenter cohort of 1,107 patients from 18 different U.S. EDs.25 Investigators found a sensitivity of 99% with NPV of 99%, while also identifying 20% of patients as low risk. Most importantly, no patients discharged home experienced MACE within 30 days.25A prospective validation was conducted of 282 patients, and investigators found decreased objective cardiac testing at 30 days by 12.1% (68.8% versus 56.7%; P=0.048) and length of stay by 12 hours (9.9 versus 21.9 hours; P=0.013), while increasing early discharges by 21.3% (39.7% versus 18.4%; P<0.001).36 In this prospective validation, no patients experienced MACE.36
HEART Pathway from Mahler 2015
A large component of the HEART pathway is utilizing a shared decision making model, which allows the patient to become an active participant in management decisions. This has been investigated in patients evaluated for pulmonary embolism and chest pain.37 Hess et al. in 2008 evaluated the use of a decision aid in chest pain, finding patients had significantly greater knowledge, greater engagement, and decided to be admitted less frequently to an observation unit for further testing.38 No major cardiac events occurred in the discharge group.38 By combining this with the HEART pathway’s MACE rate of < 1%, optimal NPV and sensitivity, and ability to categorize a significant proportion of undifferentiated chest pain as low risk, this pathway with shared decision making can decrease length of stay and decrease risk to the patient and provider. If an institution decides to implement a CDR like the HEART score, a mechanism needs to be in place to insure outpatient follow up/studies as needed.
Case Resolution: This patient’s HEART score is less than 3. His second troponin at 3 hr is negative. The patient agrees with the plan for discharge home and primary care follow up, as he feels comfortable with a risk of 1%.
Summary
– Risk stratification in patients with low risk chest pain has significantly evolved over the past decade. Multiple tools have been derived and evaluated for patient disposition decisions.
– TIMI and GRACE are not sensitive enough to use in the undifferentiated patient in the ED with chest pain.
– Decision pathways using these scores should be used with caution, though patients with two negative biomarkers and negative ECG for ischemia are at low risk for MACE.
– The HEART score and pathway provide the best sensitivity and NPV capability, while classifying a large percentage of patients as low risk.
– By combining the use of this rule with shared decision making, this pathway provides safe, efficient care, protecting the patient and physician.
References/Further reading
- Owens PL, Barrett ML, Gibson TB, Andrews RM, Weinick RM, Mutter RL. Emergency department care in the United States: a profile of national data sources. Ann Emerg Med 2010; 56:150–65.
- Pope JH, Aufderheide TP, Ruthazer R, Woolard RH, Feldman JA, Beshansky JR, et al. Missed diagnoses of acute cardiac ischemia in the emergency department. N Engl J Med 2000; 342:1163–70.
- Pines JM, Isserman JA, Szyld D, Dean AJ, McCusker CM, Hollander JE. The effect of physician risk tolerance and the presence of an observation unit on decision making for ED patients with chest pain. Am J Emerg Med 2010; 28:771–9.
- Fleischmann KE, Goldman L, Johnson PA, et al. Critical pathways for patients with acute chest pain at low risk. J Thromb Thrombolysis 2002; 13:89–96.
- Roger VL, Go AS, Lloyd-Jones DM, et al. Heart disease and stroke statistics–2011 update: a report from the American Heart Association. Circulation 2011; 123:e18–e209.
- Amsterdam EA, Kirk JD, Bluemke DA, et al; American Heart Association Exercise, Cardiac Rehabilitation, and Prevention Committee of the Council on Clinical Cardiology, Council on Cardiovascular Nursing, and Interdisciplinary Council on Quality of Care and Outcomes Research. Testing of low-risk patients presenting to the emergency department with chest pain: a scientific statement from the American Heart Association. Circulation 2010;122(17):1756-1776.
- McCarthy BD, Beshansky JR, D’Agostino RB, et al. Missed diagnoses of acute myocardial infarction in the emergency department: results from a multicenter study. Ann Emerg Med 1993;22(3):579–82.
- Freas GC. Medicolegal aspects of acute myocardial infarction. Emerg Med Clin North Am 2001;19(2):511–21.
- Rusnak RA, Stair TO, Hansen K, Fastow JS. Litigation against the emergency physician: common features in cases of missed myocardial infarction. Ann Emerg Med 1989;18(10):1029–34.
- Mitchell AM, Garvey JL, Chandra A, et al. Prospective multicenter study of quantitative pretest probability assessment to exclude acute coronary syndrome for patients evaluated in emergency department chest pain units. Ann Emerg Med 2006;47:447.
- Goldman L, Cook EF, Johnson PA, Brand DA, Rouan GW, Lee TH. Prediction of the need for intensive care in patients who come to the emergency departments with acute chest pain. N Engl J Med 1996 Jun 6;334(23):1498-504.
- Weinstock MB, Weingart S, Orth F, VanFossen D, Kaide C, Anderson J, Newman DH. Risk for Clinically Relevant Adverse Cardiac Events in Patients With Chest Pain at Hospital Admission. JAMA Intern Med 2015 Jul;175(7):1207-12.
- Goldman L, Weinberg M, Weisberg M, Olshen R, Cook EF, Sargent RK, et al. A computer-derived protocol to aid in the diagnosis of emergency room patients with acute chest pain. N Engl J Med 1982 Sep 2;307(10):588-96.
- Antman EM, Cohen M, Bernink PJ, McCabe CH, Horacek T, Papuchis G, et. al. The TIMI risk score for unstable angina/non-ST elevation MI: A method for prognostication and therapeutic decision making. JAMA 2000 Aug 16;284(7):835-42.
- Chase M, Robey JL, Zogby KE, et al. Prospective validation of the thrombolysis in myocardial infarction risk score in the emergency department chest pain population. Ann Emerg Med 2006;48(3):252–9.
- Pollack CV Jr, Sites FD, Shofer FS, et al. Application of the TIMI risk score for unstable angina and non-ST elevation acute coronary syndrome to an unselected emergency department chest pain population. Acad Emerg Med 2006;13(1):13–8.
- Campbell CF, Chang AM, Sease KL, et al. Combining thrombolysis in myocardial infarction risk score and clear-cut alternative diagnosis for chest pain risk stratification. Am J Emerg Med 2009;27(1):37–42.
- Hess EP, Thiruganasambandamoorthy V, Wells GA, et al. Diagnostic accuracy of clinical prediction rules to exclude acute coronary syndrome in the emergency department setting: a systematic review. CJEM 2008;10(4):373–82.
- Sanchis J, Bodi V, Nunez J, et al. New risk score for patients with acute chest pain, non-ST-segment deviation, and normal troponin concentrations: a comparison with the TIMI risk score. J Am Coll Cardiol 2005;46(3):443–9.
- Hess EP, Agarwal D, Chandra S, et al. Diagnostic accuracy of the TIMI risk score in patients with chest pain in the emergency department: a meta-analysis. CMAJ 2010;182(10):1039-1044.
- Backus B, Six A, Kelder J, Gibler W, Moll F, Doevendans P. Risk Scores for Patients with Chest Pain: Evaluation in the Emergency Department. Current Cardiology Reviews 2011;7(1):2-8.
- Jaffery Z, Hudson MP, Jacobsen G, et al. Modified thrombolysis in myocardial infarction (TIMI) risk score to risk stratify patients in the emergency department with possible acute coronary syndrome. J Thromb Thrombolysis 2007;24(2):137–144.
- Fox KA, Dabbous OH, Goldberg RJ, Pieper KS, Eagle KA, et al. Prediction of risk of death and myocardial infarction in the six months after presentation with acute coronary syndrome: prospective multinational observational study (GRACE). BMJ 2006 Nov 25;333(7578):1091.
- Elbarouni B, Goodman SG, Yan RT, Welsh RC, Kornder JM, Deyoung JP, et al. Validation of the Global Registry of Acute Coronary Event (GRACE) risk score for in-hospital mortality in patients with acute coronary syndrome in Canada. Am Heart J 2009 Sep;158(3):392-9.
- Mahler SA, Miller CD, Hollander JE, Nagurney JT, Birkhahn R, Singer AJ, et al. Identifying patients for early discharge: performance of decision rules among patients with acute chest pain. Int J Cardiol 2013;168:795–802.
- Six AJ, Backus BE, Kelder JC. Chest pain in the emergency room: value of the HEART score. Neth Heart J 2008;16:191–6.
- Backus BE, Six AJ, Kelder JC, et al. Chest pain in the emergency room. A multicenter validation of the HEART score. Crit Pathw Cardiol 2010;9:164–9.
- Mahler SA, Hiestand BC, Goff DC Jr, Hoekstra JW, Miller CD. Can the HEART score safely reduce stress testing and cardiac imaging in patients at low risk for major adverse cardiac events? Crit Pathw Cardiol 2011;10:128–133.
- Fanaroff AC, Rymer JA, Goldstein SA, Simel DL, Newby L. Does This Patient With Chest Pain Have Acute Coronary Syndrome? The Rational Clinical Examination Systematic Review. JAMA 2015;314(18):1955-1965.
- Backus BE, Six AJ, Kelder JC, Bosschaert MA, Mast EG, Mosterd A, et al. A prospective validation of the HEART score for chest pain patients at the emergency department. Int J Cardiol 2013 Oct 3;168(3):2153-8.
- Sun BC, Laurie A, Fu R, Ferencik M, Shapiro M, Lindsell CJ, Diercks D, et al. Comparison of the HEART and TIMI Risk Scores for Suspected Acute Coronary Syndrome in the Emergency Department. Crit Pathw Cardiol 2016 Mar;15(1):1-5.
- Than M, Cullen L, Reid CM, et al. A 2-h diagnostic protocol to assess patients with chest pain symptoms in the Asia-Pacific region (ASPECT): a prospective observational validation study. Lancet 2011;377: 1077–1084.
- Aldous SJ, Richards MA, Cullen L, Troughton R, Than M. A new improved accelerated diagnostic protocol safely identifies low-risk patients with chest pain in the emergency department. Acad Emerg Med 2012 May;19(5):510-6.
- Than M, Cullen L, Aldous S, Parsonage WA, Reid CM, Greenslade J, Flaws D, et al. 2-Hour accelerated diagnostic protocol to assess patients with chest pain symptoms using contemporary troponins as the only biomarker: the ADAPT trial Journal of the American College of Cardiology 2012. 59(23):2091-2098.
- Mahler SA, Miller CD, Litt HI, et al. Performance of the 2-hour accelerated diagnostic protocol within the American College of Radiology Imaging Network PA 4005 cohort. Acad Emerg Med 2015;22:452–460.
- Mahler SA, Riley RF, Hiestand BC, Russell GB, Hoekstra JW, Lefebvre CW. The HEART Pathway randomized trial: identifying emergency department patients with acute chest pain for early discharge. Circ Cardiovasc Qual Outcomes 2015 Mar;8(2):195-203.
- Geyer BC, Xu M, Kabrhel C. Patient preferences for testing for pulmonary embolism in the ED using a shared decision-making model. Am J Emerg Med 2014 Mar;32(3):233-6.
- Hess EP, Knoedler MA, Shah ND, Kline JA, Breslin M, Branda ME, et al. The chest pain choice decision aid: a randomized trial. Circ Cardiovasc Qual Outcomes 2012 May;5(3):251-9.




