Authors: Tanya Belle, MD (EM Resident Physician, University of Connecticut) and Adam Wise, MD (EM Attending Physician, Hartford Hospital) // Editors: Alex Koyfman, MD (@EMHighAK) and Brit Long, MD (@long_brit)
Case
A 60 y.o male presents to your ED after being in the waiting room for 6 hours, with complaints of feeling unwell for the last 4 weeks. He notes he is originally from India but has been living in the U.S. for several years. He complains of a dry cough and endorses occasional shortness of breath and subjective fevers, as well as 10lb unintentional weight loss. This is his 3rd ED visit for similar complaints. He has no significant past medical history. His vitals reveal a temperature of 100.4°F, heart rate of 100, blood pressure 110/60, respiratory rate of 26, and pulse oxygenation 93% on room air. His examination reveals a thin, unwell appearing male, in mild distress. His cardiac and pulmonary examinations are normal. What in his history is particularly concerning for possible TB? When do you consider starting treatment? At what point should he be placed in isolation?
Epidemiology and Background: Why do we care?
The number of Tuberculosis related deaths has fallen by an estimated 22% between 2000 and 2015. (1) Despite its decline in mortality overall, Tuberculosis (TB) remains one of the leading causes of communicable infectious disease-related deaths worldwide; second only to HIV. (2) According to the WHO, as of 2015, the number the number of TB related deaths was averaged at just over 1 million .Incident cases worldwide were quoted at 10.4 million; with HIV co-infected individuals accounting for 1.2 million (11%) of all new cases. Males accounted for the majority, with 5.9 million (56%) cases, females 3.5 million (34%), and children 1 million cases (10%). Amongst the new cases, there were 48000 cases of multidrug-resistant TB (MDR-TB). (1)
While the disease is less prevalent in the United States, the numbers of persons infected overall remains significant at an estimated 15 million. In 2015 there were >9,000 new cases reported alone, representing a rate of 3.0 cases per 100,000 persons. (3)
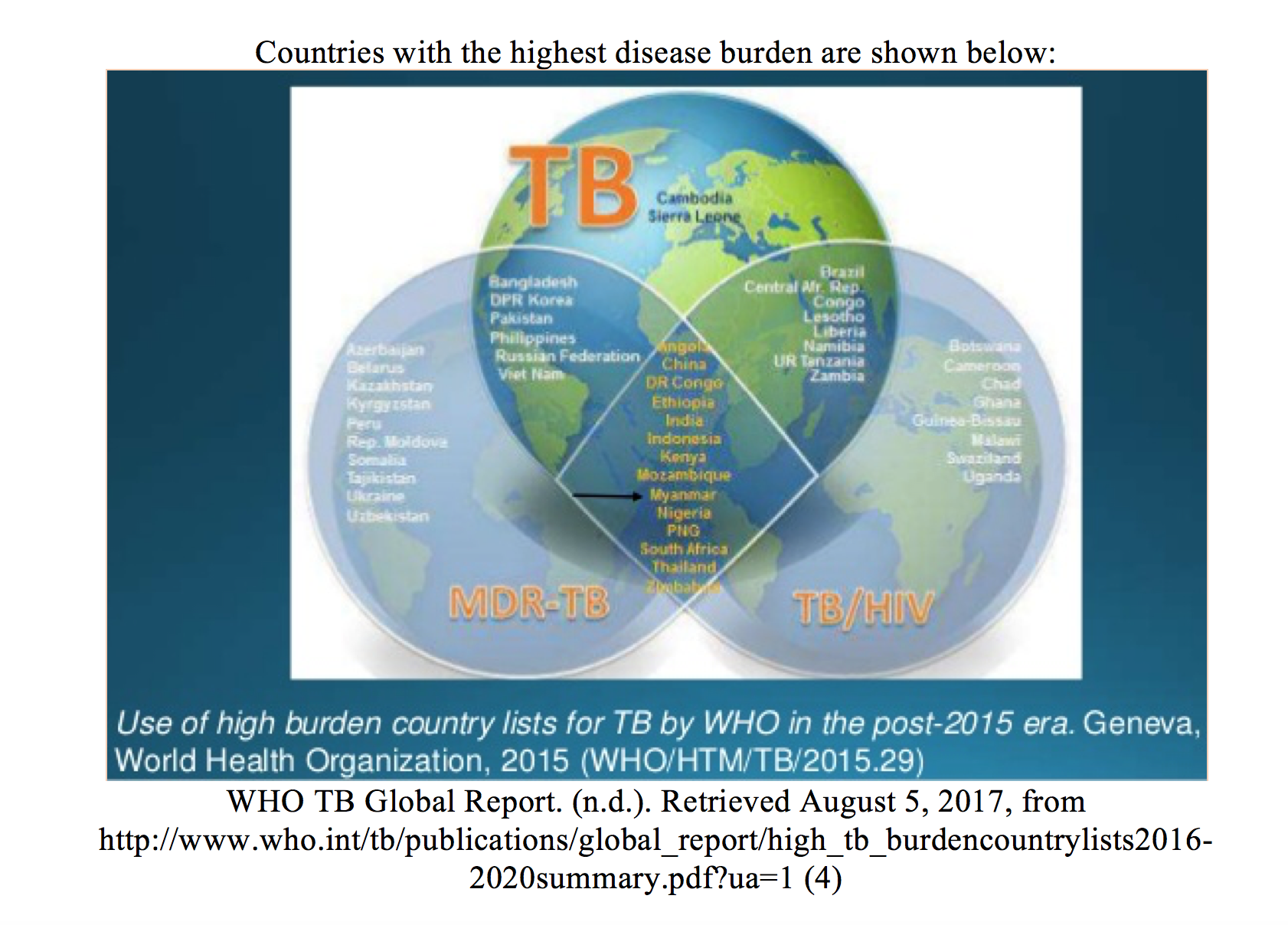
Countries with the lowest rates of TB (<25 per 100,000 persons) include the United States, Canada, Australia, Western Europe, and Japan. (5)
Pathogenesis and Disease manifestation
TB is causes by the slow-growing acid-fast bacillus Mycobacterium Tuberculosis. It is spread via aerosolized respiratory secretions. After exposure, the particles migrate to the lung alveoli, activating the host’s defense mechanisms. The infectious sequence of events is dependent on the pathogen burden and the host’s immune system.
- In an immunocompetent host, the bacteria are destroyed by the immune system, prior to infection developing. (6)
- Infection may become established and the organism is transported to regional lymph nodes where it may become contained by the immune system in granulomas (tubercles), thereby limiting replication and spread of the disease. This results in latent TB which generally lasts for life. These patients are at risk of re-activation TB if their immune systems become compromised and they are no longer able to contain the infection. The overall lifetime risk of reactivation of TB is estimated to be 10% in immunocompetent individuals; it is higher in those with HIV at approximately 7% per year. (6)
- In those immunosuppressed individuals, initial infection can lead to primary active TB.
Primary TB
- Host cell-mediated response leads to granuloma formation / tubercles, in lymph nodes, which represent primary infection.
- A similar reaction occurs within the lung resulting in the Ghon complex (calcified hilar lymph nodes).

- In the case of containment failure, the organisms spread via direct, haematogenous, and lymphatic routes, generally towards areas with higher oxygen content/ blood flow (apical and posterior segments of the upper lobe, superior segment of the lower lobe of the lung, the renal cortex, the meninges, epiphyses of long bones, vertebrae). The organism may remain dormant within these regions for several years, where it may only be detected by a positive tuberculin skin test. (8)
Reactivation TB
Otherwise referred to as chronic TB or post primary disease, this form represents the majority of adult cases. It is the result of reactivation of a previously contained focus of mycobacteria which was seeded at the time of primary infection (9). Symptoms are similar to those of active TB.
Who is at risk?
Over 50% of the active TB cases reported in the U.S. currently occur in foreign-born individuals, with the majority being the result of re-activation of latent TB. (5)
Risk factors for developing TB include the following: recent residence in an endemic region, low socioeconomic status, ethnic minorities, homelessness, close contact to known case of TB, institutional living or employment at high-risk facilities (e.g., correctional facilities, homeless shelters, skilled nursing facilities), health care employment (5), elderly or very young patients, and immune suppression.
Clinical Presentation
ED diagnosis of TB can be challenging on account of the highly variable nature of presentation. This is further compounded by the fact that primary TB is for the most part asymptomatic, and the culturing process of the organism takes several days to weeks.
The signs and symptoms of active disease are similar to reactivation TB. Patients may present with either pulmonary manifestations (most commonly) or systemic. The key to early diagnosis is considering the disease.
Common presenting symptoms include fever, productive cough, dyspnea, night sweats, malaise, fatigue and weight loss, hemoptysis, and pleuritic chest pain.
The absence of cough does not rule out the possibility of TB. In an ED based study by Sokolove et al., cough was only present in 64% of cases and the chief complaint in less than 20% of patients. (10) Physical exam findings tend to be nonspecific and may include rales or evidence of pleural effusions. (5) Patients who have bronchial extension of TB may present with productive cough with wheezing, which may be misdiagnosed as asthma.
Extrapulmonary Manifestations
Approximately 15% of immunocompetent patients with TB will present with extra-pulmonary manifestations, which are even more common in patient with HIV co-infection. (11) Every organ system can be affected by TB; however, the most common extra-pulmonary sites include lymph nodes, CNS, bones, and joints.
Tuberculous Lymphadenitis
- This form represents approximately 40% of extra-pulmonary cases; cervical, mediastinal, and axillary nodes are most commonly affected. Generally, adenopathy tends to be unilateral and nontender, with matted nodes on exam. (11)
- Patients can develop scrofula, which is cervical lymphadenitis where the nodes become matted and enlarge within the neck, sometimes to the extent of rupturing through the skin and forming fistulas.

Pleural TB
- This represents 4% of TB cases; presenting with pleuritic chest pain, cough and unilateral pleural effusion on CXR. (12)
- Pleural fluid analysis is diagnostic in approximately 30% of cases only. (13)
Central Nervous System
- CNS involvement occurs in 1% of cases but represents one of the more severe manifestations of the disease. (14) Focal neurologic deficits or cranial nerve palsies may occur, and long-term neurologic dysfunction is common. Patients may go through 3 phases of illness: a prodromal phase characterized by a more indolent onset of headache, fever, and altered mental status; a meningitic phase similar to bacterial meningitis; and finally a paralytic phase (coma, seizures, paralysis, and death). (15)
- CSF analysis is similar to that of bacterial meningitis with a mononuclear pleocytosis. (5)
Tuberculous Peritonitis
- Most common presentation of gastrointestinal tract involvement, presenting with ascites, abdominal pain, weight loss, and fever. Consider this in patients presenting with unexplained lymphocytic ascites. (5)
Tuberculous Pericarditis
- This presents with pericardial effusion and is a common cause of constrictive pericarditis. (16)
Skeletal TB
- Occurring in 1% to 5% of patients with TB, the thoracolumbar spine is most commonly affected. (17) Patients may complain of pain over the affected area.
Miliary TB
- This term is classically used to describe the appearance of the lung in cases of disseminated TB. Currently the term is applied to wide hematogenous spread during primary or reactivation disease, which carries a higher mortality. (8) When occurring during active disease, patients may present more severely with evidence of multi-organ failure and shock.
Investigations
Patients with high clinical suspicion of having TB based on history or positive screening tests should have a chest x-ray (CXR) done. If there are findings concerning for tuberculous changes, these patients should go on to have sputum culturing done. It should be noted that while culture is the gold standard for diagnosis, definitive diagnosis in the ED is generally not possible as culture takes several weeks.
Imaging
- CXR should be obtained on anyone suspected of having TB.
- Classic findings include upper lobe infiltrates, cavitation, hilar and para-tracheal adenopathy.
- Approximately 5% of patients with active pulmonary disease have a normal chest radiograph.
- Immunosuppressed patients are more likely to have atypical radiographic findings (e.g. less predisposition to upper lobes). (18)
- Apical computed tomography may show a “tree in bud” pattern with centrilobar lesions and nodules and branching linear densities. (19)
Screening options: The Mantoux and Interpreting the PPD
The Mantoux test is the most commonly employed screening method for TB exposure. 0.1 ml of purified protein derivative (PPD) is injected subcutaneously in the forearm, and the degree of induration at the test site is measured 48-72 hours later. Although the PPD test is unable to discriminate between active TB and latent TB, any patient with a newly positive skin test or recent conversion should be considered for further investigation and treatment (8). Some situations may give false negative and false positive results.
False Positive Results: persons who have received Bacillus Calmette-Guérin (BCG) immunization may have a positive test without infection, as well as patients exposed to nontuberculosis mycobacteria.
False Negative Results: inaccurate administration of test or reading of results, patients who are very early in the course of their disease, and patients with profound immunosuppressed states (8).
For patients in whom skin testing may be unreliable, a serum quantiferon (Interferon-gamma release assay) test can be done. This is an indirect test for TB which measures the levels of interferon-gamma which is released by infected hosts in response to M. tuberculosis proteins. It has a higher specificity than skin testing and is more useful in such cases as mentioned above.

NB: Detection of newly infected persons in a screening program:
- ≥10-mm induration increase within any 2-year period is positive if <35 years old; ≥15-mm induration increase within any 2-year period is positive if >35 years old (8)
Other tests: Nucleic acid amplification test (NAAT) utilizes PCR of bodily fluids (e.g. sputum, CSF, pleural fluid), with results available within 1 day. It is highly specific, but a negative NAAT is unable to rule out disease especially if clinical suspicion is high. Gold standard testing includes culture, but definitive diagnosis in the ED is generally not possible, as culture takes several weeks.
Treatment/ Disposition
- Isolation within a negative pressure room should be done as early as possible for those suspected of having TB. Treatment should not be initiated before consulting with hospital infectious disease specialists. As this is a reportable disease, public health services should be notified of all suspected and confirmed cases. Given the frequency of co-infection with HIV, patients identified as having active TB should receive counselling and HIV testing.
- Contact primary care physicians or public health services and arrange for long-term care before patient discharge. Discharge instructions include home isolation procedures and follow-up at the appropriate clinic to receive medication and ongoing care. Antituberculosis medications should not be instituted in the ED unless there is joint agreement with the consultant and follow-up providers.
- Prior to commencing therapy, baseline labs are recommended as follows: CBC (platelet count), LFTs, serum urea, and creatinine.
Some cases where compliance and home isolation can be guaranteed are suitable for outpatient management. Admission should be considered for those patients with uncertain diagnosis; potentially noncompliant patients; concern for multidrug resistant TB (MDRTB); or severe illness with respiratory compromise, shock, or multi-organ failure.
Treatment Regimens
- Requires combination therapy to overcome organism resistance.
- Regimens are divided into an intensive phase of 2 months, followed by a continuation phase of either 4 or 7 months (total of 6 to 9 months for treatment).
- Continuation phase of treatment is given for either 4 or 7 months.
- Direct observation therapy (DOT) is recommended for certain treatment regimens and generally done on a case by case situation. It is required in most cases of multidrug resistant treatments, as adherence is paramount.
Active TB
- Initial therapy includes:
- First-line treatment includes 4 drug regimen, plus pyridoxine for 8 weeks
- Isoniazid (INH): 300 mg (child 10 mg/kg up to 300 mg) orally daily
- Rifampicin (RIF): 600 mg (adult less than 50 kg: 450 mg; child 10 mg/kg up to 600 mg) orally daily PLUS
- Ethambutol (E): 15 mg/kg orally daily (up to 1200 mg; in adults and children 6 years or older) PLUS
- Pyrazinamide (PZA): 25 mg/kg (up to 2 g) orally daily
- Pyridoxine: 25 mg orally daily. (20)
- Continuation therapy:
- 2 drug regimen for 18-31 weeks based on culture results.
- First-line treatment includes 4 drug regimen, plus pyridoxine for 8 weeks
Latent TB
- INH alone is appropriate for recent asymptomatic skin test conversion in any person in close contact with an actively infected patient and anergic patients with known tuberculosis contact. (8)
- Therapy continues for 9 months unless contraindicated.
- See the table below for CDC recommended treatment regimens.

Table showing CDC recommended treatment regimens for latent TB infection; reproduced from CDC website. Note: Due to the reports of severe liver injury and deaths, CDC recommends that the combination of rifampin (RIF) and pyrazinamide (PZA) should not be offered for the treatment of latent TB infection. (21)
Steroid Use: Steroids act as an adjunct in certain forms of TB infection to decrease complications associated with infection such as hydrocephalus, constrictive pericarditis, neurological deficits, intestinal strictures, and pleural adhesions. They have recently been demonstrated to improve the morbidity in HIV patients with paradoxical TB immune reconstitution inflammatory syndrome (IRIS). Indications include tuberculous meningitis, pericarditis, and adrenal insufficiency due to TB. (22)
Special circumstances
Pregnancy: For active TB the regimen should consist of 9 months of INH, RIF, and EMB. Current literature does not recommend discontinuation of breast feeding during this period. Also pyridoxine supplementation is recommended for all pregnant and lactating women. (5)
Multidrug Resistant TB: With the emergence of organisms resistant to first line therapy, treatment regimens have become more expensive and challenging. These patients are at increased risk of treatment failure. Infectious disease consultation is recommended, and the addition of a second line agent is needed which may include fluoroquinolones, amikacin, prothionamide, and para-aminosalicylic acid (PAS). Treatment duration is usually approximately 18-24 months duration. (23)
Common Complications of TB drugs
Isoniazid commonly causes hepatitis, giddiness, convulsions, peripheral neuropathy (preventable with pyridoxine – vitamin B6); potential interaction with anticonvulsants.
Rifampicin has several side effects which include hepatitis, gastrointestinal upset, rashes, thrombocytopenia, renal failure, and hemolytic anemias. Orange discolouration of secretions (urine, tears, saliva, semen,) and staining of contact lenses may occur. It potentially interacts with the following medications: oral contraceptives, anticoagulants, hypoglycemic, theophylline, antiarrhythmics, dapsone, anticonvulsants, antifungals, corticosteroids, and antiretrovirals.
Pyrazinamide use can result in hepatitis, arthralgia, flushing, and gout. Diabetics may experience more lability in blood glucose levels. Ethambutol is most commonly associated with optic neuritis (avoid use in children younger than 7 years or in cases of impaired renal function). (20)
Infection Control in the ED
- Strict isolation practices should be observed for patients suspected or confirmed to have TB.
- During transport, patients should wear surgical masks covering their mouth and nose.
- Both aerosol isolation + contact isolation employed.
- Isolations rooms should have private bathrooms and the number of persons entering the rooms should be limited.
- Doors should be kept closed as much as possible.
- Negative pressure rooms.
- Cough inducing/ aerosol generating procedures should be performed only if necessary (e.g. intubations and suctioning, bronchoscopy, sputum induction).
- Staff dealing with these patients should wear gloves and high-efficiency particulate filter masks or respirators (N95 or N100). (20)
Key points
- TB remains a devastating and fairly ubiquitous disease throughout several parts of the world despite recent downward trends in incidence.
- It can present in a variety of ways so a high index of suspicion is needed when evaluating patients with signs and symptoms suggestive of possible infection.
- Patients co-infected with HIV or otherwise immunosuppressed tend to present more atypically.
- Effective management relies on prompt recognition
- Diagnosis relies on a combination of adequate history and clinical, radiographical and microbiological data.
- Treatment should be started only after consultation with Infectious Disease specialists at your institution.
- Strict adherence to isolation precautions is paramount in preventing the spread of infection in the ED.
References / Further Reading:
- World Health Organisation. (n.d.). Tuberculosis (TB): WHO Global TB report 2016. Retrieved August 6, 2017, from World Health Organisation: http://www.who.int/gho/tb/en/
- Frieden T, S. T. (2003;). Tuberculosis. Lancet, 362(9387).
- (n.d.). Trends in Tuberculosis 2015. Retrieved August 6, 2017, from https://www.cdc.gov/tb/publications/factsheets/statistics/tbtrends.htm
- WHO TB Global Report. (n.d.). Retrieved August 5, 2017, from http://www.who.int/tb/publications/global_report/high_tb_burdencountrylists2016-2020summary.pdf?ua=1
- Irene G. Sia, M. M. (2011). Current Concepts in the Management of Tuberculosis. Mayo Clinic Proceedings, vol 86 (4): 348-361.
- Richard E. Rothman, M. P.-H. (2006). Communicable Respiratory Threats in the ED: Tuberculosis, Influenza, SARS and other aerosolized infections. Emergency Medicine Clinic of North America, 24 (989-1017).
- http://www.isradiology.org/tropical_deseases/tmcr/chapter5/large5/05-006B.jpg
- Vu D. Phan, J. M. (2015). Tuberculosis. In J. E. Tintinalli, Tintinalli’s Emergency Medicine: A comprehensive study Guide, 7th edition (pp. 459-464).
- Anton Pozniak, M. F. (2016, january 12). Clinical manifestations and complications of pulmonary tuberculosis. Retrieved august 5, 2017, from Uptodate: https://www.uptodate.com/contents/clinical-manifestations-and-complications-of-pulmonary-tuberculosis?source=search_result&search=tuberculosis&selectedTitle=1~150
- Sokolove P, R. L. (2000). The Emergency Department Presentation of patients with active Pulmonary Tuberculosis. Acad Emerg Medicine, 1056-60.
- Peto HM, P. R. (2009). Epidemiology of extrapulmonary tuberculosis in the United States, 1993-2006. Clin Infect Dis. , 49:1350-1357.
- Baumann MH, N. R. (2007). Pleural tuberculosis in the United States: incidence and drug resistance. 131:1125-1132
- Gopi A, M. S. (2007). Diagnosis and treatment of tuberculous pleural effusion in 2006. Chest. 131:880-889 .
- Phypers M, H. T. (2006). CNS tuberculosis: a longitudinal analysis of epidemiological and clinical features. Int J Tuberc Lung Dis. 10:99-103.
- Sutlas PN, U. A. (2003). Tuberculous meningitis in adults: review of 61 cases. Infection. 31:387-391 .
- Reuter H, B. L. (2005). Epidemiology of pericardial effusions at a large academic hospital in South Africa. Epidemiol Infect. 133:393-399.
- Mehta JB, D. A. (1991). Epidemiology of extrapulmonary tuberculosis: a comparative analysis with pre-AIDS era. Chest, 99:1134-1138.
- , S. (2001). Tuberculosis control in the 21st century. Emerg Infect Dis. 7(2):259–62.
- Lee KS, S. K. (1993). Adult-onset pulmonary tuberculosis: findings on chest radiographs and CT scans. AJR Am J Roentgenol. 160:753-758.
- Nickson, C. (2016, December 14). Tuberculosis. Retrieved August 5, 2017, from Life in the Fastlane: https://lifeinthefastlane.com/ccc/tuberculosis/
- Tuberculosis (TB). (2017, June 29). Retrieved August 10, 2017, from https://www.cdc.gov/tb/topic/treatment/ltbi.htm
- Kadhiravan T, D. S. (2010 Jul-Sep). Role of corticosteroids in the treatment of tuberculosis: an evidence-based update. Indian J Chest Dis Allied Sci. 52(3):153-8.
- Lange C, A. I. (2014). Management of patients with multidrug-resistant/extensively drug-resistant tuberculosis in Europe: a TBNET consensus statement. The European Respiratory Journal. 44(1):23-63.






{kind=link}