Authors: Todd Duppong, MD (PGY2, Emergency Medicine Residency Program, Morristown Medical Center), Cynthia Santos, MD (Assistant Professor Emergency Medicine, Medical Toxicology, Rutgers NJMS) // Edited by: Alex Koyfman, MD (@EMHighAK, EM Attending Physician, UTSW / Parkland Memorial Hospital), and Brit Long, MD (@long_brit, EM Attending Physician, San Antonio Military Medical Center)

Case:
A 35 year old lady intentionally overdosed on her prescription medication for fibromyalgia and recent diagnosis of depression. ECG shows sinus tachycardia (rate of 150), QRS ≥120 ms, and R wave elevation in aVR ≥3 mm. What are the action potential phases responsible for ECG changes? What ECG changes are associated with cardiotoxicity? Which medications cause changes in action potential/ECGs?
Background:
An electrocardiogram (ECG) is a rapid diagnostic tool frequently used for evaluation because of the predictable cardiotoxic effects from specific drugs. Serial ECGs should be performed in addition to a good history, physical examination, and evaluation of clinical findings/toxidrome to guide course and treatment.
Figure 1: Represents ECG and time associated action potential phases.[1] 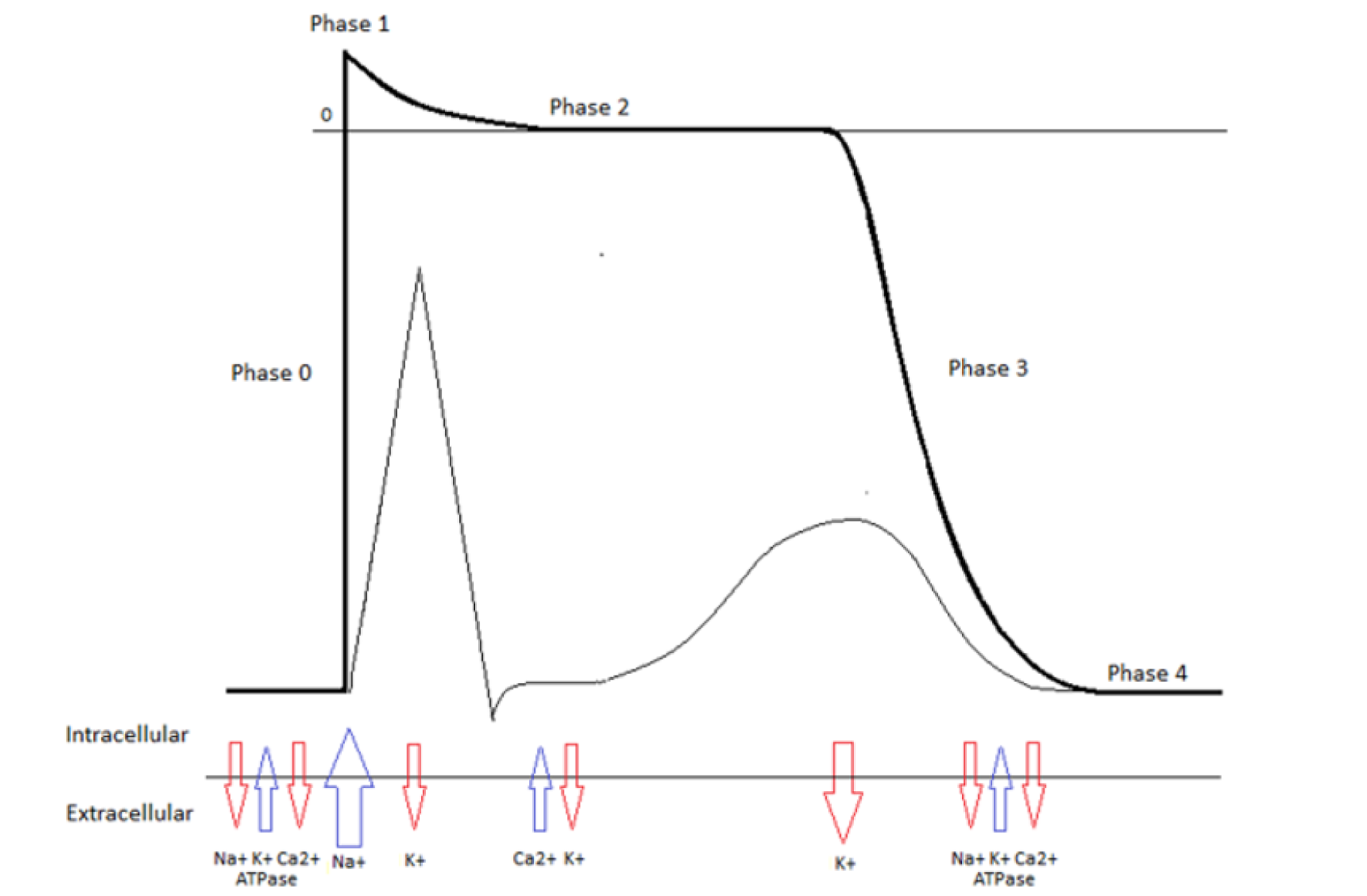
Pearls:
- Phase 0 is a rapid depolarization which results from sodium entering the cell. Sodium channel blockers result in ECG changes with a widened QRS complex.
- Examples of Sodium channel blockers include (phase 0): lidocaine, phenytoin, bufatoxin, tetrodotoxin, TCA, antihistamines
- ECG changes for sodium channel blockers: QRS widening, RBBB, right axis deviation, ventricular tachycardia/fibrillation, bradycardia, asystole, ST-T changes
- Class 1b antidysrhythmic (lidocaine, phenytoin, etc.) do NOT affect the QRS width because of the fast association/dissociation kinetics.
Figure 2: Common sodium channel blockers which cause QRS widening.[1]

- Phase 1 is the initial repolarization (overshoot). The voltage-sensitive sodium channels close and potassium ions efflux from the cell.
- Phase 2 is the plateau phase which balances the calcium influx and potassium efflux.
- Examples of Potassium channel blockers include (phase 2 and 3): antipsychotics and methadone.
Figure 3: Potassium channel blockers result in QT prolongation followed by torsade de pointe.[1]
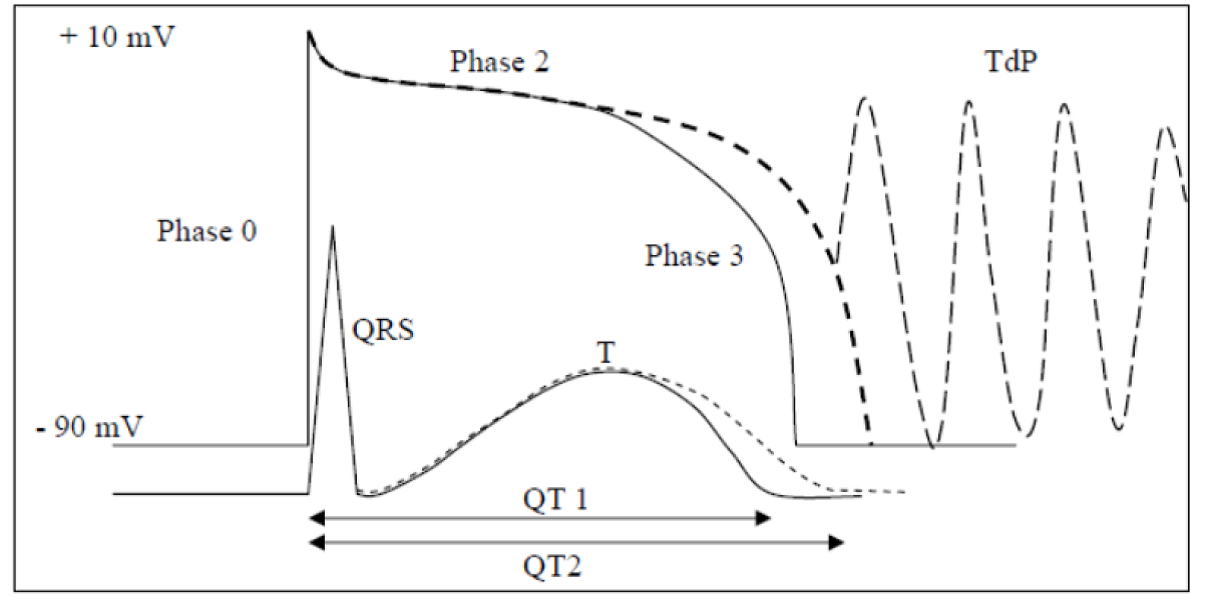
- Phase 3 is the repolarization phase which results from the L-type calcium channels closing while the rectifier potassium channels open resulting in potassium efflux and net positive outward current.
- ECG changes for potassium channel blockers: QT prolongation, T- or U-wave abnormalities, premature ventricular beats, torsade de pointes, sinus tachycardia.
Figure 4: Common potassium channel blockers. [2]

- Phase 4 is the resting membrane potential which is maintained by the Na-K-ATPase and maintains the negative membrane potential at around -90 mV.
- ECG changes for Sodium-Potassium ATPase inhibitors:
- Excitant activity: atrial/junctional premature beats, atrial tachycardia, atrial flutter/fibrillation, accelerated junctional rhythms, premature ventricular beat, bigeminy and multifocal, ventricular tachycardia, bi-directional ventricular tachycardia/fibrillation.
- Suppressant activity: sinus bradycardia, sinoatrial block, type I second degree AV block, type II second degree AV block, complete AV block, bundle branch blocks.
- Combination: atrial tachycardia with AV block, sinus bradycardia with junctional tachycardia, Wenckebach with junctional premature beats, regularization of ventricular rhythm with atrial fibrillation.
- Examples of Sodium-Potassium ATPase inhibitors include (phase 4): cardiac glycosides (digoxin, digitalis, budodienolides).
- Hypokalemia potentiates digitalis toxicity.

References:
- Santos C., Manini A. Electrocardiographic Interpretation. In: Part 3: Investigations of cardiocirculatory failure. New York, NY: Mount Sinai School of Medicine.
- Lionte C., Bolaga C., Sorodoc L. Toxic and Drug-Induced Changes of the Electrocardiogram. Advances in Electrocardiograms – Clinical Applications. 15: 271-296.
- Yates C., Manini A. Utility of electrocardiogram in drug overdose and poisoning: theoretical considerations and clinical implications. Current Cardiology Review. 2012; 8: 137-151.





1 thought on “Tox Card: Cardiovascular Drug Effects on the Action Potential and ECG”
Pingback: Länkar v41-42 | Internmedicin