
Welcome back to the “52 in 52” series. This collection of posts features recently published must-know articles. Our second post looks at the SALSA trial.

Authors: Sarah Mongold, MD (Chief Resident, Emergency Medicine Physician, San Antonio, TX); Brannon Inman (Chief Resident, Emergency Medicine Physician, San Antonio, TX) // Reviewed by: Alex Koyfman, MD (@EMHighAK); Brit Long, MD (@long_brit)
Risk of Overcorrection in Rapid Intermittent Bolus vs Slow Continuous Infusion Therapies of Hypertonic Saline for Patients With Symptomatic Hyponatremia
AKA: THE “SALSA” TRIAL
Let’s Cha-Cha into this one (I’m sorry I had to).
Clinical question:
What is the risk of overcorrection of hyponatremia using hypertonic saline (3%) as rapid intermittent bolus (RIB) versus slow continuous infusion (SCI)?
Study design:
- Prospective, multicenter, investigator initiated open label (not blinded) randomized clinical trial
- Serum sodium measured every 6 hours for 2 days
- Hypertonic saline administered for 24-48 hours
PICO:
Population:
- Included moderately severe to severe symptomatic hyponatremic patients > 18 years with glucose corrected sodium below 125 mmol/L
- Severe symptoms included vomiting, stupor, seizure, and coma (GCS ≤8)
- Performed in 3 general hospitals in the Republic of Korea
- Patients were excluded if they had:
- primary polydipsia (urine osmolality ≤100 mOsm/kg)
- were pregnant or breastfeeding
- anuria
- arterial hypotension (systolic blood pressure <90 mm Hg and mean arterial pressure <70 mm Hg)
- liver disease (defined as transaminase levels >3 times the upper limit of normal, known decompensated liver cirrhosis with ascites or diuretic use, hepatic encephalopathy, and varices)
- uncontrolled diabetes (A1C >9%)
- history of cardiac surgery, acute myocardial infarction, sustained ventricular tachycardia, ventricular fibrillation, acute coronary syndrome
- cerebral trauma, and increased intracranial pressure within 3 months prior to randomization
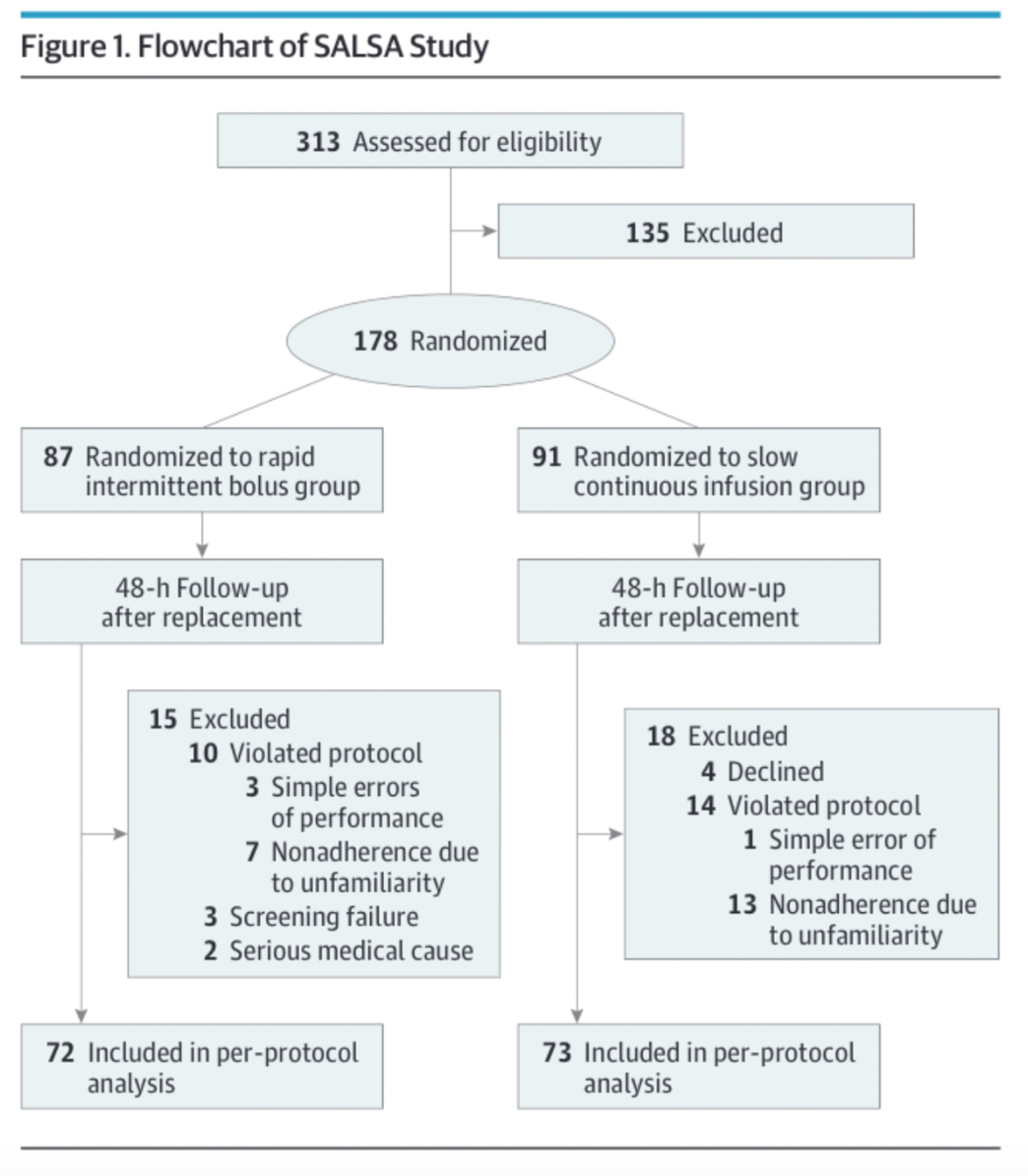
- 178 patients randomized, mean age 73.1 years, mean serum sodium 118.2 mmol/L
Intervention:
- 2 cc/kg 3% NaCl serial measurements and repeat dosing vs. observation vs. therapeutic relowering
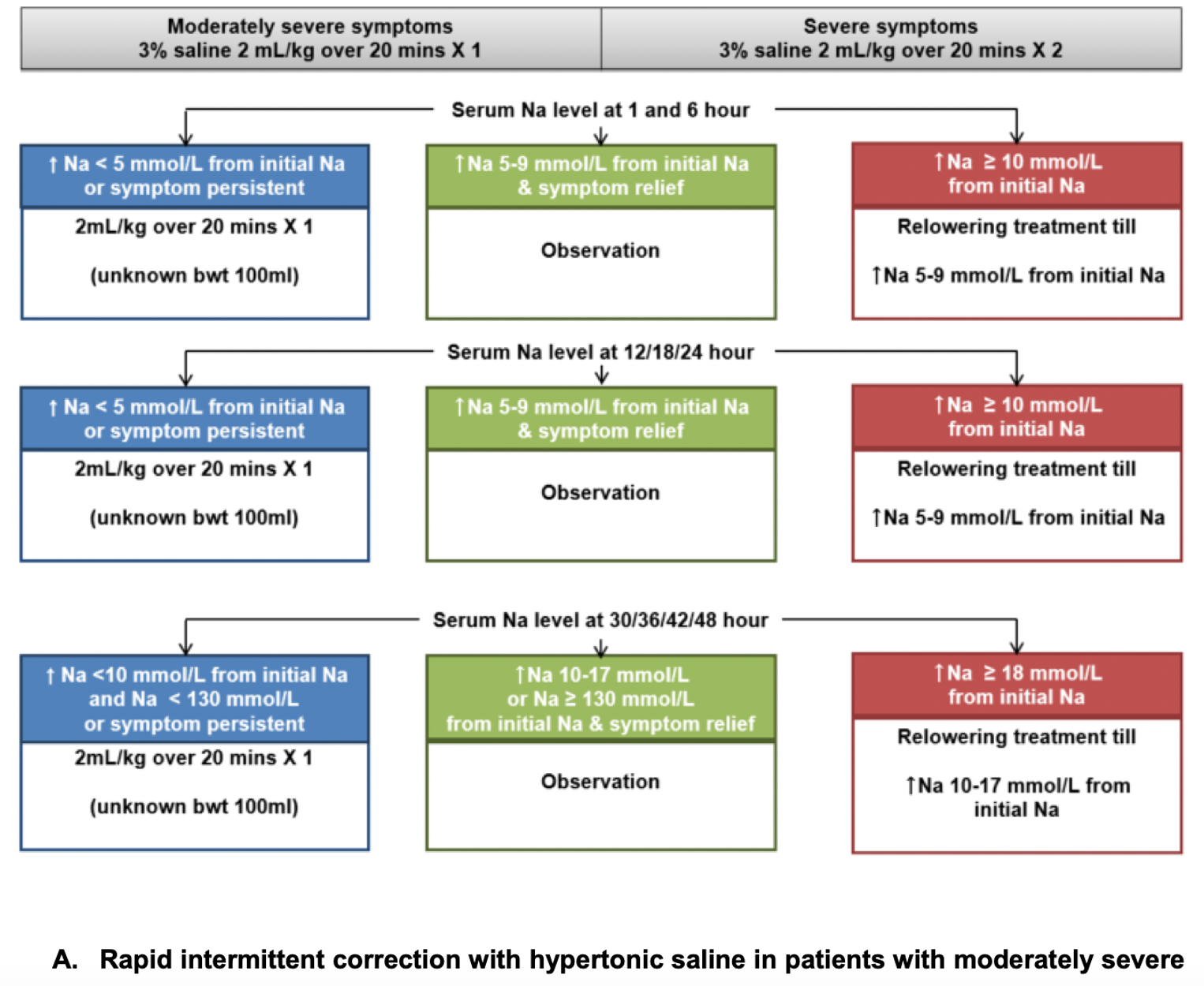
Excerpt from supplemental data within manuscript
Comparator:
- Weight and symptom severity based hypertonic saline infusion

Excerpt from supplemental data within manuscript
Outcome:
- Primary outcome was over correction, defined as increase in serum sodium of 12 mmol/L in 24 hours or 18 mmol/L in 48 hours
- Overcorrection occurred in 17% of RIB and 24 % of SCI (not statistically significant, P=0.26)
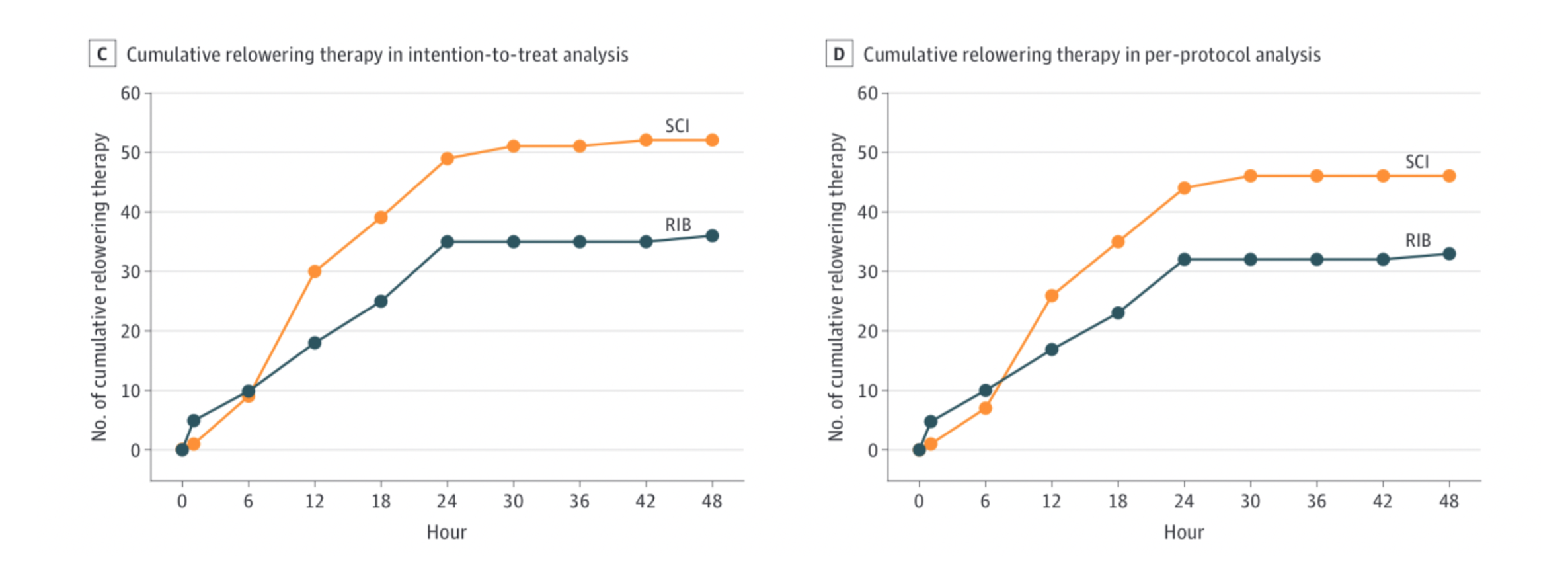
- Therapeutic relowering more common in SCI (41% in RIB, 57% in SCI, P=0.04)
- RIB demonstrated better efficacy in achieving target correction rate within 1 hour versus SCI
- Intention to treat analysis: RIB 32.3%, SCI 17.6%, absolute risk difference 14.6% (95% CI 2% – 27.2%), NNT 6.8
- Per protocol analysis: RIB 29.2%, SCI 16.4%, absolute risk difference 12.7% (95% CI -0.8% to 26.2%)
Take away:
- No difference in achieving correction goal at 48 hours. Trend toward over correction in SCI (P=0.26). Relowering more common in SCI group (P=0.04).
- Rates of achieving target correction in 1st hour higher in the RIB group.
- This study asks an important clinical question and is the first prospective RCT evaluating RIB and SCI.
- Groups were similar at baseline.
- Unfortunately, the outcomes are not patient centered, and the 95% CIs were wide for overcorrection incidence.
- A significant number of patients were excluded because of protocol violations, and the exclusion criteria are complicated.
My take:
- I find RIB more feasible in the stressful environment of the ED, and it achieved target correction rate in the 1st hour at higher rates compared to SCI. When I think management of symptomatic hyponatremia is needed in the ED, I will be doing RIB.
- However, both RIB and SCIR therapy were safe and effective, and further RCTs are needed evaluating this question.
Reference:
- Baek SH, Jo YH, Ahn S, et al. Risk of Overcorrection in Rapid Intermittent Bolus vs Slow Continuous Infusion Therapies of Hypertonic Saline for Patients With Symptomatic Hyponatremia: The SALSA Randomized Clinical Trial. JAMA Intern Med. 2021;181(1):81-92. doi:10.1001/jamainternmed.2020.5519





1 thought on “52 in 52 – #2: The SALSA Trial”
Pingback: Quiz 162, July 15, 2022 – The FOAMed Quiz