Originally published on Ultrasound G.E.L. on 6/22/20 – Visit HERE to listen to accompanying PODCAST! Reposted with permission.
Follow Dr. Michael Prats, MD (@PratsEM) from the Ultrasound G.E.L. team!

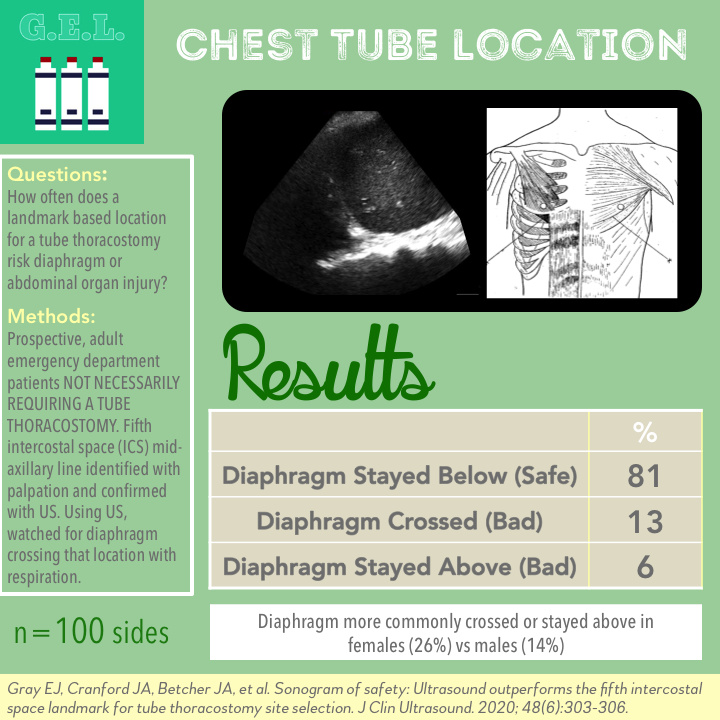
Sonogram of Safety: Ultrasound Outperforms the Fifth Intercostal Space Landmark for Tube Thoracostomy Site Selection
J Clin Ultrasound April 2020 – Pubmed Link
✳Check out the Ultrasound Podcast on this article (including interview with the authors!)
Take Home Points
1. Placing a tube thoracostomy in the fifth intercostal space at the midaxillary line has the potential for serious complication or organ injury in a significant proportion of asymptomatic patients.
2. There may be a role for point-of-care ultrasound in determining the safest location for tube thoracostomy.
Background
Tube thoracostomy is commonly performed in patients with trauma, pneumothorax, and a variety of other thoracic pathologies. Generally, a landmark approach is used to guide the location and placement. Unfortunately, whether due to technique or variation in patient anatomy, there can be serious complications from a misplaced chest tube including organ injury, infection, and hemorrhage. We use ultrasound to guide or assist many other procedures, including thoracentesis which is actually pretty similar. Ultrasound can identify the region you want to go in and find the things you want to avoid hitting. So the idea of this study was to see if ultrasound could help identify the most safe and appropriate location for placing a chest tube, laying the groundwork for an ultrasound-assisted approach to this procedure.
Questions
When the anatomic landmark method (confirmed by ultrasound) is used to identify the fifth intercostal space, how often does POCUS determine that this location is safely above the diaphragm through the entire respiratory cycle?
Population
Single academic center
Inclusion:
- Presenting to the emergency department
- Able to raise arms over head
✳ Note these were not patients who actually needed a chest tube
Exclusion:
- Pregnancy
- Prisoners
- <18 years old
- ≥100 years old
- Refused or could not consent
Design
Prospective convenience sample
Any patient meeting criteria in the ED could be enrolled. They did not have to require a tube thoracostomy
For the anatomical approach, ribs were palpated to find the fifth intercostal space. This was verified with ultrasound. This was marked in the midaxillary line bilaterally.
This area was then scanned with ultrasound, noting the location of the diaphragm through respiration. This was repeated on the contralateral side.
Also recorded height, age, weight, gender, and medical history including prior thoracic procedures.
The main outcome was seeing if the diaphragm either crossed the marked area or stayed consistently above the area, based on the ultrasound of the selected anatomic location. They assigned a score of 0 for crossing and 1 for staying above the location.
Who did the ultrasounds?
A research physician. Study specific training not specified
The Scan
Curvilinear transducer

The study notes that palpation began at the Angle of Louis (the sternal angle or manubriosternal junction) to find second rib.
The ultrasound was oriented in a frontal plane in the mid-axillary line
Learn how to do an ultrasound-guided Thoracentesis on ACEP’s Sonoguide!
Check out Pulmonary Pathology on the POCUS Atlas!

Results
50 patients → 100 sides scanned
- Mean age 51.6
- 38% female
- 18% had COPD or asthma
- 1 patient had a prior tube thoracostomy, no other patients had prior thoracic procedures
Primary Outcome – % of hemi-diaphragms that either crossed or stayed above the marked location
81% of diaphragms were below area marked (this is good, this is what we want if we are placing a chest tube at this location)
13% crossed (this is bad, potentially dangerous)
6% were above (this is worse, highest risk of problems)
Other Findings
Broken down by laterality – % of hemi-diaphragms that either crossed or stayed above the marked location
- Right 20% of the time (CI 11-33%)
- Left 18% (CI 9-31%)
Broken down by gender – % of hemi-diaphragms that either crossed or stayed above the marked location
- Female 26%
- Male 14%
Overall ultrasound showed the diaphragm crossed or stayed above the marked location in 24% of patients.
All patients with COPD, asthma, or previous thoracic surgery (total n = 10) had diaphragms that did not cross the fifth intercostal space.
Limitations
These were not patients who needed a chest tube. How were these patients selected? How can we be sure there are no biases in the selection process? We know that “normal” anatomy (or at least patients without this particular pathology requiring a chest tube) does not always equate to the pathologic anatomy. Interestingly, all of the patients with preexisting lung pathology had hypothetically safe diaphragms in this study. Nonetheless, further study is needed in a population that actually requires this procedure.
The study design is almost like a type of incorporation bias. By this I mean that it seems like they are attempting to compare a landmark approach to an ultrasound-guided approach but using ultrasound as the standard for the comparison. Obviously this would unfairly result in making the ultrasound approach look superior. Now they are not really doing that here because they are not truly comparing ultrasound to landmark (the paper title is pretty misleading in that respect). But it seems like they are using this paper to begin the argument that ultrasound guidance would result in greater safety than a landmark based approach. That is why it would have been valuable to have a separate standard – such as successful chest tube placement. Clearly, this study is only the preliminary work for the hypothesis that ultrasound-assisted tube thoracostomy is safer. We just have to keep this in mind moving forward.
Discussion
The exclusions from this study were understandable, but many of these populations would be interesting to evaluate. Pregnancy, the very young, the very old – all of these types of patients might have different anatomy that makes ultrasound even more valuable compared to landmark technique. Perhaps this could be the subject of further study.
Keep in mind that they effectively eliminated any inaccuracy that could have resulted from an inability to accurately find the 5th intercostal space. In this study, they confirmed the correct space by counting ribs with ultrasound. Therefore, it is possible that the anatomical location could have performed even worse in real practice.
As mentioned in their limitations section – it would be great if we knew where the safe place was! Based on this study, couldn’t we just say “go higher”? Many of us are already urging our learners to err on the more cephalad location. Finding a consistently safe location with ultrasound could be the next step. Use ultrasound to find a consistently safe region to do the procedure, whether by landmark or ultrasound assisted. On the other hand, perhaps the point is that no such universal anatomical location exists and that the ultrasound should be used in all cases.
Take Home Points
1. Placing a tube thoracostomy in the fifth intercostal space at the midaxillary line has the potential for serious complication or organ injury in a significant proportion of asymptomatic patients.
2. There may be a role for point-of-care ultrasound in determining the safest location for tube thoracostomy.
More Great FOAMed on this Topic
The Ultrasound Podcast on THIS article – with Jacob Avila, Mike Prats and an interview with the authors!
Our score

Expert Reviewer for this Post

Mary Beth Phelan, MD @mbphelan
Chief of the Division of Point of Care Ultrasound, Department of Emergency Medicine, Medical College of Wisconsin
Reviewer’s Comments
Excellent and thorough review. One pattern when reviewing this topic was the higher percentage of women in the current study with unexpected anatomic variation (ie diaphragm at or above recommended 5th ICS), or difficulty determining the recommended ICS related to anatomic landmark methods (see Bowness JS, Nicholls K, Kilgour PM, et al. Emerg Med J 2015;32:951–954. This indicates that gender deserves further investigation with respect to the impact US may have in increasing safety in this population as well as those with underlying lung disease and prior chest surgical procedures.
Future studies utilizing US to identify safer sites for chest tube insertion in patients requiring chest tubes would be able to evaluate whether respiratory status of a critical patient i.e. tachypnea or intubation impacts visualization or location of the diaphragm in addition to the anatomic and pathologic considerations discussed. I am not sure what to think of the discussion regarding incorporation bias. To me it seemed that the article described an evaluation of the 5th ICS by US and found by using US there were unexpected anatomic variations in a significant portion of the patients, at presumed safe sites. I agree with the blog post author that this is a great first step and the work needs to be replicated in a diseased population.
Cite this post as
Michael Prats. Chest Tube Location – Using POCUS to Assess Diaphragm Position. Ultrasound G.E.L. Podcast Blog. Published on June 22, 2020. Accessed on July 8, 2022. Available at https://www.ultrasoundgel.org/94.




