
Welcome back to the “52 in 52” series. This collection of posts features recently published must-know articles. This week the series covers an RCT from the New England Journal of Medicine: “Immediate Transfusion in African Children with Uncomplicated Severe Anemia”.

Author: Christiaan van Nispen, MD (Emergency Medicine Physician Resident, San Antonio, TX) and Brannon Inman (Chief Resident, Emergency Medicine Physician, San Antonio, TX) // Reviewed by: Alex Koyfman, MD (@EMHighAK); Brit Long, MD (@long_brit)
Immediate Transfusion in African Children with Uncomplicated Severe Anemia
Clinical question:
In African children presenting with uncomplicated severe anemia, is there a mortality benefit to performing immediate whole blood transfusion?
Study design:
- Factorial, open-label RCT
PICO:
Population:
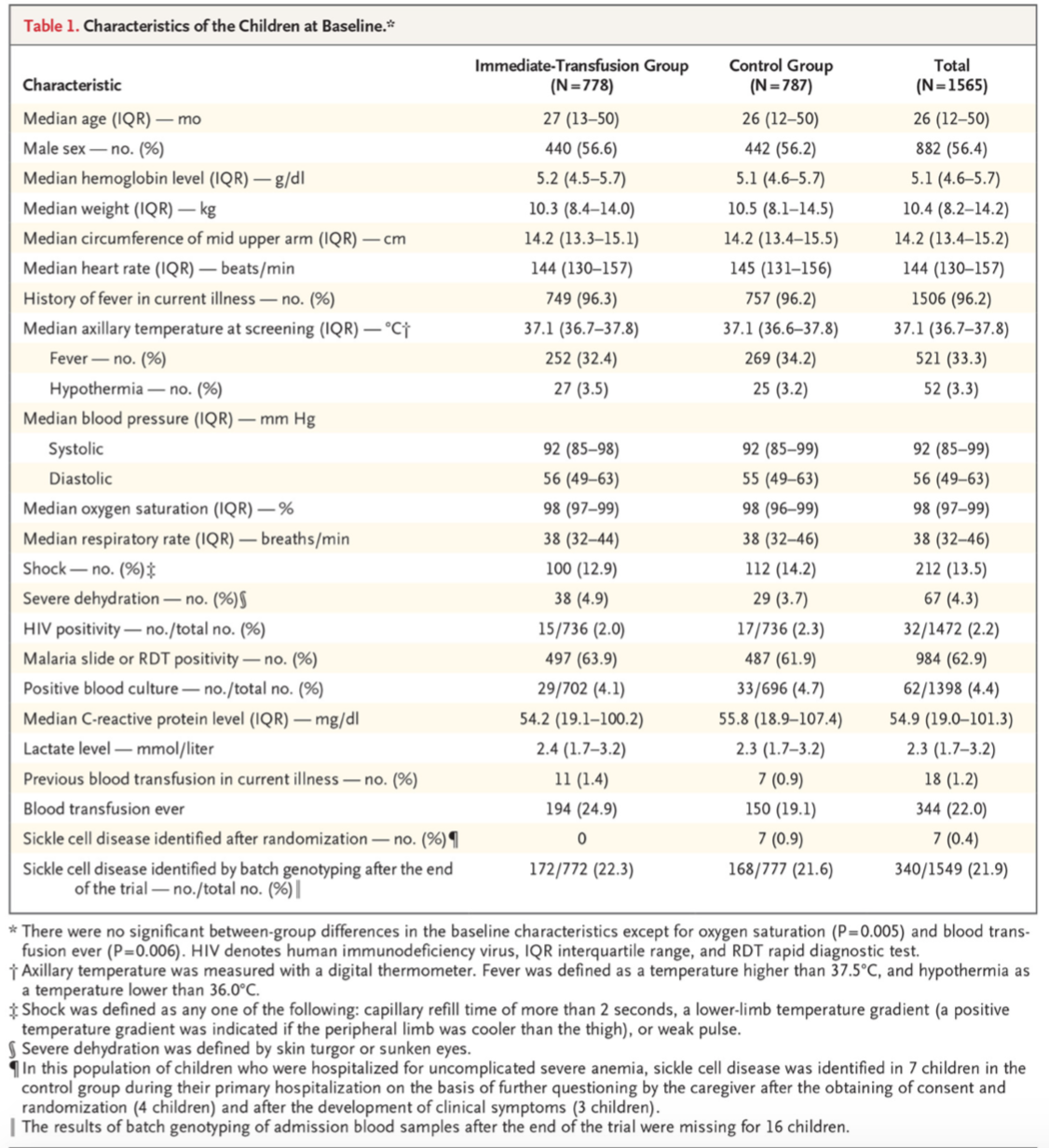
- 1565 children aged 2 months to 12 years, mean 26 months
- Inclusion criteria
- Severe anemia with (defined as a hemoglobin level of 4-6 g/dL)
- Anemia needed to be asymptomatic
- Exclusion criteria included:
- Altered mental status
- Respiratory distress
- Hemoglobinuria during the present illness
- Hemoglobin level less than 4 g/dL
- Reported history of sickle cell disease
- Additionally excluded if had hepatic, renal, or heart failure, or if there was an established past medical history of sickle cell anemia
- Enrollment halted whenever blood products were unavailable
- 3 hospitals in Uganda and 1 hospital in Malawi
Intervention: There were two intervention groups
- Immediate 20 mL/kg transfusion of whole blood or equivalent and admission to the hospital ward
- Immediate 30 mL/kg transfusion of whole blood or equivalent and admission to the hospital ward
- After initial randomization, patients in the intervention arm underwent a second randomization to determine which volume they would receive
Control:
- Admission and expectant management (same interval re-evaluations and hemoglobin level studies), with transfusion if hemoglobin < 4 g/dL or development of severe symptoms (those outlined in symptomatic exclusion criteria).
Outcome:
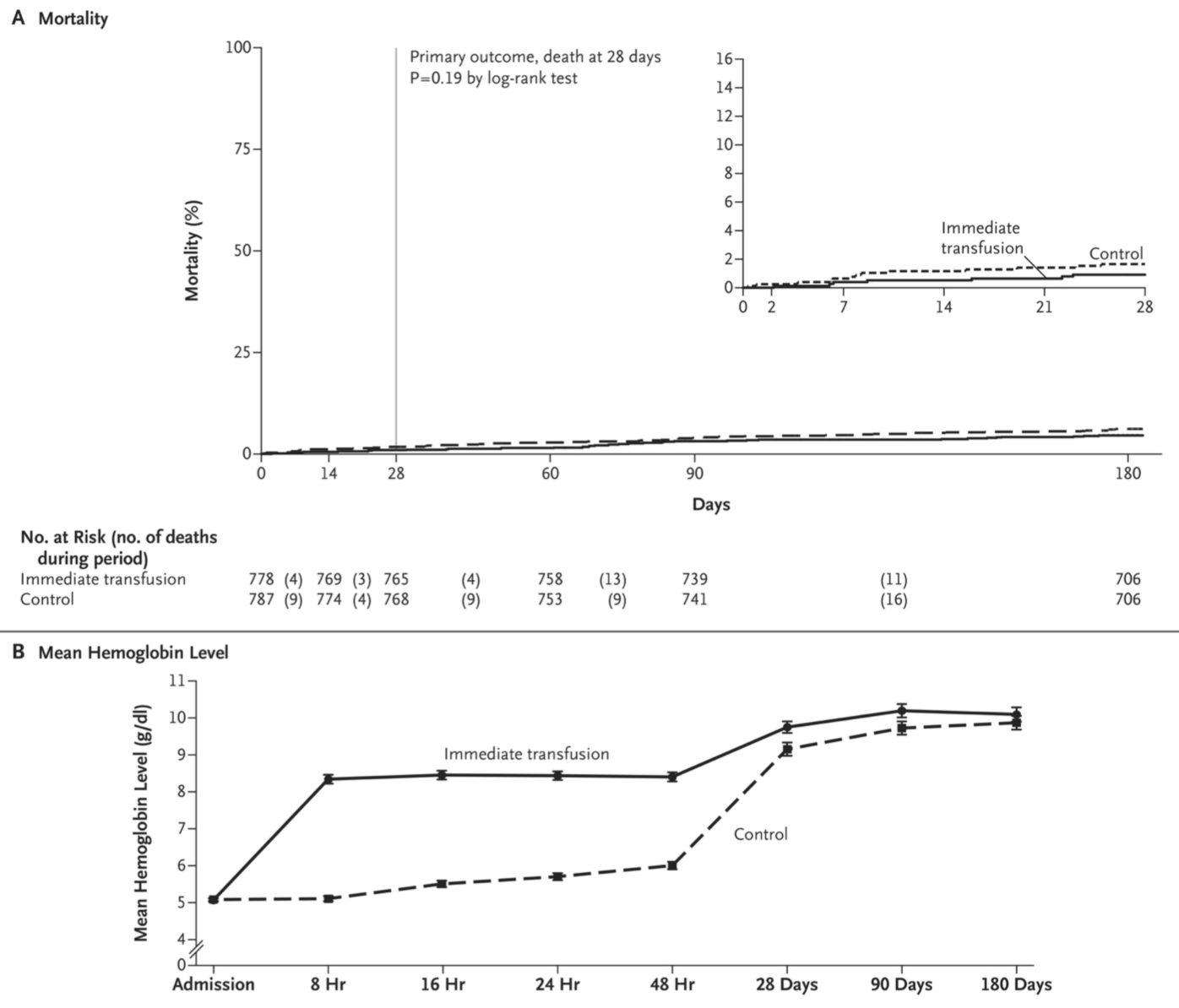
- No statistically significant difference in the primary outcome of mortality at 28 days.
- No statistically significant difference in secondary outcomes of mortality at 48 hours, 90 days, or 180 days.
- The control group was much more likely to develop profound anemia (hemoglobin < 4 g/dL) during the index hospitalization, thus requiring a transfusion (39.3% vs. 1.4%).
- By 28 days the mean hemoglobin level of the control group approached the immediate transfusion group and remained so at 90 and 180 days.
- The intervention group had a shorter hospitalization duration (3 versus 4 days), though the control group’s hospitalization was less costly despite the longer length of stay.
Take aways:
- This study seeks to determine if there is merit in transfusion of asymptomatic, generally healthy children in an area of the world that is short on blood donations.
- The patients were evenly randomized between groups with limited loss to follow-up are assets
- The authors significantly overestimated the expected mortality of the control group, leading to the study to be under-powered to detect subtle differences between the groups; the existence of multiple intervention groups also does not help in this regard
- Although not statistically significant, mortality percentage was lower in the 20 mL/kg group than the control group, and lower still in the 30 mL/kg group, so questions are raised as to whether this would have achieved significance with more power
- External validity is limited.
- Study involves hospitals in just two countries.
- As the mortality estimates were based on prior epidemiological research, questions remain as to whether the standard care received by these patients was at baseline superior to typical African hospitals.
- It is noted that this study did not enroll patients when blood was unavailable at the study hospitals, useful for study purposes but not a realistic condition during the actual practice of medicine in these geographical areas.
- Possible that patients admitted to these during periods of blood shortage suffered higher mortality than those in the control group of this study who had the advantage of still receiving blood products if hemoglobin dropped below 4 g/dL or were in extremis.
My take:
- This study supports the World Health Organization’s guideline for regions with limited access to blood products to not transfuse asymptomatic, generally healthy children with hemoglobin levels of > 4 g/dL. However, this study is insufficiently powered, and more research is warranted to ensure that this approach is not harmful.
- It is also possible that additional research would bear out that the overall approach is reasonable, with slightly altered parameters to minimize mortality or other severe outcomes (for example, increasing the mandatory transfusion threshold to 4.5 or 5 g/dL).
- Finally, not transfusing a child with hemoglobin levels of 4-7 g/dL likely would not meet the standard of care in many other countries where blood products are more abundant, even if it does meet World Health Organization guidelines in Uganda and Malawi.
Reference:
- Maitland K, Kiguli S, Olupot-Olupot P, et al. Immediate Transfusion in African Children with Uncomplicated Severe Anemia. N Engl J Med. 2019;381(5):407-419. Doi: 10.1056/NEJMoa1900105
.




