
Authors: Morgan Penzler, MD, (Emergency Medicine Resident, Atrium Health’s Carolinas Medical Center); Kathryn T Kopec, DO (@KopecToxEM, EM Attending Physician, Medical Toxicologist, Carolinas Medical Center, Charlotte, NC) // Reviewed by: James Dazhe Cao, MD (@JamesCaoMD, Associate Professor of EM, Medical Toxicology, UT Southwestern Medical Center, Dallas, TX); Alex Koyfman, MD (@EMHighAK); Brit Long, MD (@long_brit)

Case:
A 34-year-old male presented to the emergency department after being found down with an empty 500 count bottle of acetaminophen (APAP) 500 mg. He was noted to be bradycardic, hypotensive, and obtunded upon arrival, with dried emesis on his face and shirt. He was promptly intubated for airway protection, and a broad toxicologic workup was pursued. The APAP level returned at > 500 mcg/mL, and initial liver function tests (LFTs) were normal (ALT 17 IU/L, AST 21 IU/L). Treatment was started with N-acetylcysteine (NAC) and a one-time dose of fomepizole at 15 mg/kg.
Questions:
- What is the mechanism of action of fomepizole?
- What is the appropriate dosing of fomepizole?
- What is the role of fomepizole in APAP toxicity?
Background:
Fomepizole (4-methylpyrazole, 4-MP) is primarily known for its role in the treatment of toxic alcohol ingestions. Fomepizole is a potent inhibitor of alcohol dehydrogenase (ADH), which prevents methanol and ethylene glycol from being broken down into their respective toxic metabolites (Figure 1).1
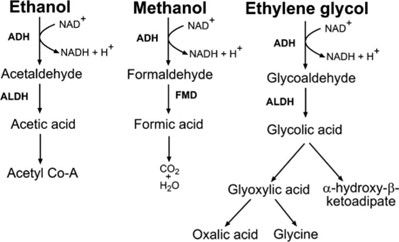
Figure 1: Metabolism of Toxic Alcohols2
The main goal when treating toxic alcohols is blocking ADH which can be accomplished using ethanol or fomepizole. Fomepizole is highly preferable to ethanol, as it has a significantly higher affinity for ADH when compared to ethanol.2 Fomepizole also has minimal side effects compared to ethanol (intoxication, central nervous system depression, etc.) and does not require therapeutic monitoring of serum concentrations. Conversely, fomepizole is more expensive than ethanol (~$5,000 per 48 hours of therapy) and is not available in every clinical setting.2
Dosing of Fomepizole for Toxic Alcohols3
- Initial dose is 15 mg/kg IV, followed by 10 mg/kg IV every 12 hours for 4 doses.
- If treatment is required for more than 48 hours, dosing should be increased back to 15 mg/kg as fomepizole begins to stimulate its own metabolism.
- For patients requiring hemodialysis:
- Administer fomepizole at the start of dialysis if the last dose was > 6 hours earlier.
- At the end of dialysis:
- If dialysis lasted 1-3 hours, give a half dose, then resume every 12-hour dosing.
- If dialysis lasted >3 hours, give a full dose, then resume every 12-hour dosing.
- Continue fomepizole until serum toxic alcohol concentrations are expected to be less than < 25 mg/dL with no acid-base disturbances.1
Fomepizole’s Effects on Pharmacokinetics:
Fomepizole’s administration affects the half-lives of methanol and ethylene glycol as it is a potent ADH blocker. Methanol exhibits dose dependent kinetics but with larger ingestions, seems to predominately exhibit first-order elimination. With fomepizole administration, the half-life of methanol was noted to be approximately 54 hours, compared to a half-life of about 3 hours with no fomepizole administration.4 Ethylene glycol is dependent upon the kidneys for excretion. With normal renal function the half-life is roughly 8.6 hours.5 With the use of fomepizole, in a patient with normal renal function, the half-life increases to approximately 14-17 hours, and can be up to 49 hours in patients with a creatinine above 1.2.6 These increases in half-lives are essential to understanding patients with toxic alcohol ingestions as they may require a prolonged hospitalization and/or hemodialysis to resolve their toxicity.
Fomepizole Use in APAP Toxicity:
Fomepizole more recently has been used as an adjunct in treatment of APAP overdose.7 It is thought to offer a benefit in APAP toxicity via two different mechanisms.
1: Fomepizole is a CYP2E1 inhibitor and has been shown to reduce conversion of APAP to NAPQI.
- Acetaminophen is broken down by CYP450 enzymes, primarily 2E1, into the toxic metabolite, NAPQI (Figure 2). A study by Lee et al. demonstrated that CYP2E1 knockout mice were considerably less sensitive to acetaminophen’s hepatotoxic effects when compared to wild-type animals.8 Using x-ray crystallography, the structure of CYP2E1 and its active sites were dissolved in a complex with two small molecular weight inhibitors, indazole and fomepizole. This study assisted in the discovery that fomepizole can bind to the CYP2E1 active site, causing inhibition of the enzyme, suggesting the potential to lead to decreased production of toxic metabolites.9
2: Fomepizole also inhibits c-Jun-N-terminal kinase (JNK).
- JNK can increase the oxidant stress and mitochondrial membrane permeability leading to hepatic injury.10 Fomepizole acts as an inhibitor at the ATP binding site of JNK. Inhibition of JNK prevents further toxicity during the metabolic phase by reducing development of reactive oxygen species.10
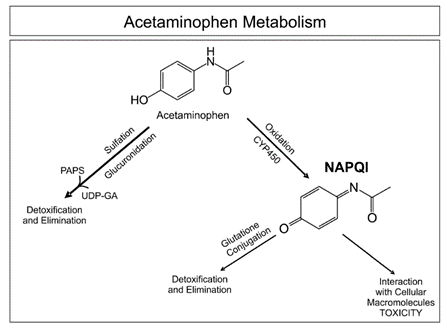
Figure 2: Metabolism of Acetaminophen11
Indications for Fomepizole Treatment in APAP Toxicity:
Currently, fomepizole has only been used experimentally in patients who are at a high risk of developing significant hepatotoxicity. One method of determining risk of severe hepatotoxicity is using the aminotransferase multiplication product. An aminotransferase multiplication product of > 10,000 mg/L x IU/L has been associated with a high likelihood of developing hepatotoxicity.12 This level is obtained by multiplying the serum APAP concentration by the alanine transaminase activity (ALT) level. Other markers that may indicate patients that are at high risk for subsequent development of significant hepatotoxicity include a history of chronic ethanol use (as these patients have upregulated CYP2E1), delay in administration of NAC > 8 hours after ingestion, or a serum APAP half-life of > 4 hours.13,14 It has also been suggested that in massive overdoses, APAP levels of > 600 mcg/mL the use of fomepizole may be beneficial.15
Dosing of fomepizole is not yet standardized in its use for APAP toxicity. In one study, the standard dosing for toxic alcohol ingestion was used (15 mg/kg IV over 30 min, with repeated doses of 10 mg/kg every 12 hours) at the physicians’ discretion or until APAP levels were undetectable.7,16 Other case reports have noted using a single dose of 15 mg/kg IV.13
Case Followup:
The patient’s LFTs peaked at 48 hours post ingestion (ALT 124 IU/L, AST 80 IU/L), then normalized over the next 4 days. He was successfully extubated and was transitioned to care under the psychiatry team once medically cleared.
Clinical Pearls:
- Fomepizole is an inhibitor of ADH, CYP2E1, and c-JNK.
- Traditionally used to treat toxic alcohol ingestions but has an emerging role in the treatment of APAP toxicity.
- Typical dosing for toxic alcohol toxicity includes initial bolus of 15 mg/kg IV, followed by 10 mg/kg IV every 12 hours for 4 doses.
- Dosing in APAP toxicity varies but often is initiated at 15 mg/kg IV.
References:
- Nelson, L., Hoffman, R., Howland, M. A., Lewin, N., Goldfrank, L., & Smith, S. W. (2019). Goldfrank’s Toxicologic Emergencies, Eleventh Edition (11th ed.). McGraw Hill / Medical.
- Kraut, J. A., & Kurtz, I. (2008). Toxic alcohol ingestions: clinical features, diagnosis, and management. Clinical Journal of the American Society of Nephrology, 3(1), 208-225.
- Lindros, KO, et al. The disulfiram (Antabuse)-alcohol reaction in male alcoholics: its efficient management by 4-methylpyrazole. Alcohol Clin Exp Res. 1981;5:528–530.
- Brent, J, et al. Fomepizole for the treatment of methanol poisoning. N Engl J Med. 2001;344:424–429.
- Sivilotti M, et al. Toxicokinetics of ethylene glycol during fomepizole therapy: implications for management. Ann Emerg Med. 2000;36:114–125.
- Baud, F, et al. 4-Methylpyrazole may be an alternative to ethanol therapy for ethylene glycol intoxication in man. J Toxicol Clin Toxicol. 1986;24:463–483.
- Link, S. L., Rampon, G., Osmon, S., Scalzo, A. J., & Rumack, B. H. (2021). Fomepizole as an adjunct in acetylcysteine treated acetaminophen overdose patients: a case series. Clinical Toxicology, 1-6.
- Lee, S. S., Buters, J. T., Pineau, T., Fernandez-Salguero, P., & Gonzalez, F. J. (1996). Role of CYP2E1 in the Hepatotoxicity of Acetaminophen (∗). Journal of Biological Chemistry, 271(20), 12063-12067.
- Porubsky, P. R., Meneely, K. M., & Scott, E. E. (2008). Structures of human cytochrome P-450 2E1: insights into the binding of inhibitors and both small molecular weight and fatty acid substrates. Journal of Biological Chemistry, 283(48), 33698-33707.
- Jaeschke, H., Akakpo, J. Y., Umbaugh, D. S., & Ramachandran, A. (2020). Novel therapeutic approaches against acetaminophen-induced liver injury and acute liver failure. Toxicological Sciences, 174(2), 159-167.
- Moyer, A. M., Fridley, B. L., Jenkins, G. D., Batzler, A. J., Pelleymounter, L. L., Kalari, K. R., … & Weinshilboum, R. M. (2011). Acetaminophen-NAPQI hepatotoxicity: a cell line model system genome-wide association study. Toxicological Sciences, 120(1), 33-41.
- Wong, A., Sivilotti, M. L., Dargan, P. I., Wood, D. M., & Greene, S. L. (2015). External validation of the paracetamol-aminotransferase multiplication product to predict hepatotoxicity from paracetamol overdose. Clinical toxicology, 53(8), 807-814.
- Shah, K. R., & Beuhler, M. C. (2020). Fomepizole as an adjunctive treatment in severe acetaminophen toxicity. The American journal of emergency medicine, 38(2), 410-e5.
- Schiødt, F.V., Ott, P., Christensen, E., Bondesen, S. (2002) The value of plasma acetaminophen half-life in antidote-treated acetaminophen overdosage. Clin Pharmacol Ther, 71:221-5.
- Filip, A.B., Berg, S., Mullins, M.E., Schwarz, E.S. On behalf of the Toxicology Investigators Consortium (ToxIC) (2022). Fomepizole as an adjunctive therapy for acetaminophen poisoning: cases reported to the toxicology investigators consortium (ToxIC) database 2015–2020, Clinical Toxicology, 60:9, 1006-1011.
- Rampon, G., Wartman, H., Osmon, S., & Scalzo, A. (2020). Use of fomepizole as an adjunct in the treatment of acetaminophen overdose: a case series. Toxicology Communications, 4(1), 1-4.





1 thought on “ToxCard: Fomepizole for Acetaminophen Toxicity”
Pingback: Quiz 178, February 3, 2023 – The FOAMed Quiz