
Authors: Charles Kieffer, MD (EM Resident, University of Kentucky, Lexington, Kentucky), Ryan Doucette (EM Resident , Sunrise Health GME Consortium), Jacob Avila, MD (@UltrasoundMD, EM Attending Physician, University of Kentucky), Scott Rubenstein (EM Attending Physician, Sunrise Health GME Consortium), Faith Louthan (MS-2, University of Kentucky College of Medicine) // Reviewed by Edward Lew (@elewMD); Alex Koyfman, MD (@EMHighAK); and Brit Long, MD (@long_brit)
Cases
Case 1: You are working a shift and EMS arrives with a 22-year-old man with a stab wound to the right chest. Patient is in pain and mild to moderate respiratory distress. His vital signs show a HR of 109, BP 107/63, RR 24, SpO2 93%. How would you manage this patient?
Case 2: You are working a shift and EMS arrives with a 33-year-old woman with a stab wound to the right mid abdomen. Patient is in obvious pain. Her vital signs show a HR of 107, BP 103/53, RR 24, SpO2 99%. Her FAST is negative. How would you manage this patient?
Case 3: An 18-year-old man presents with a stab wound to the mid upper abdomen and shortness of breath. He is in mild distress. His vital signs show a HR of 107, BP 103/67, RR 19, SpO2 96%. FAST is positive. What imaging studies would you order and what injuries are you concerned about?
Anatomy
The thorax (chest cavity) is boarded by the diaphragm at the inferior most aspect and is confined by the ribs anteriorly, posteriorly, laterally and superiorly. Important structures contained within are the heart, lungs, tracheal, esophagus, and major blood vessels.
 The abdominal cavity is bound by the diaphragm superiorly and the upper plane of the pelvic cavity inferiorly (1). The abdomen houses organs for digestion, kidneys and major blood vessels. The aorta bifurcates at the level of the fourth vertebra, which is generally the umbilicus in smaller habitus individuals.
The abdominal cavity is bound by the diaphragm superiorly and the upper plane of the pelvic cavity inferiorly (1). The abdomen houses organs for digestion, kidneys and major blood vessels. The aorta bifurcates at the level of the fourth vertebra, which is generally the umbilicus in smaller habitus individuals.
Trauma literature divides the abdomen into 4 distinct regions (2,3):
- Anterior abdomen – anterior axillary lines laterally, costal margin superiorly and groin crease inferiorly
- Thoracoabdominal area- Fourth intercostal space anteriorly, inferior angle of the scapula posteriorly and costal margin inferiorly
- Posterior abdomen- subcostal margin superiorly, posterior axillary lines laterally, buttock crease inferiorly
- Flank- costal margins superiorly, ASIS inferiorly, and between the anterior and posterior axillary lines laterally
Each region carries higher risk for particular injuries. The posterior abdomen and flank are more associated with retroperitoneal and solid organ injuries, while the thoracoabdominal region is higher risk for injuries to the diaphragm and the anterior abdomen is highest risk for hollow viscus injury (2).

Approach to the Patient with Abdominal Trauma
All patients with abdominal trauma, blunt or penetrating should have a Focused Assessment with Sonography in Trauma (FAST) examination. The use of point of care ultrasound (POCUS) in Emergency Medicine is well established and particularly FAST exam is widely utilized. FAST consists of four views: perihepatic space (including Morrison’s pouch), perisplenic space, pericardium, and the pelvis (4). The extended FAST, or eFAST, includes the assessment of lung sliding bilaterally to determine the presence of a pneumothorax. While the use of sonography in the Western Trauma Association (WTA) recommendations is limited to the pericardial assessment (2), other literature shows FAST exam is an excellent adjunct when used in initial and even subsequent assessment of abdominal trauma (5,6). In penetrating abdominal trauma (not limited to stab wounds in most studies) FAST has demonstrated excellent specificity (94.1-100%) but low sensitivity (28.1-100%) for diagnosing intraperitoneal free fluid, presumably blood in the case of trauma (7). The negative predictive value in assessing for free intraperitoneal fluid in blunt abdominal trauma in one study, for example, was 92% for the initial exam and increased to 96.6% NPV after subsequent examination within 24 hours (6). This is a low risk, expedient exam that has the added benefit of not requiring the patient to leave the emergency department. POCUS is also widely available, portable and can give the practiced clinician crucial data when other, more advanced imaging studies are not available.
The most commonly injured organs in the setting of penetrating abdominal trauma in order are the small intestine, liver, spleen, stomach/colon, with kidney injury and vascular injury accounting for 3-4% of injuries each. Liver and small intestine account for the vast majority of injuries with a rate of 30% each (8). Management of specific organ injuries is left in the hands of the surgeons and is out of the scope of an Emergency Medicine Physician.
Management of penetrating abdominal injuries has changed over time, from mandatory exploratory laparotomy to selective conservatism. In the setting of isolated abdominal stab wounds the decision begins with hemodynamic stability of the patient. Unstable patients are directed to the operating room as well as patients with evisceration or impalement (9,10).
Common accepted reasons to proceed directly to laparotomy would include patients with peritoneal signs, unstable vital signs, evisceration or obvious signs of internal organ damage (ie hematemesis or gross blood via NG or per rectum, free air on diagnostic imaging).
Care of a hemodynamically stable patient is often dictated by the resources available to the physician. Serial clinical examinations (SCEs), local wound exploration (LWE) and diagnostic imaging (DI) are the three main clinical pathways and will be dictated by resources available and influenced by the region of the abdomen injured. The WTA recommends hemodynamically stable patients with injuries to the flank or posterior abdomen receive DI, particularly high-resolution CT imaging, due to the difficulty detecting injuries to the retroperitoneal space with SCEs and slower progression of injuries becoming clinically obvious in this particular anatomic space (11).
LWE is generally used in anterior abdominal stab wounds to assess if the anterior fascia has been penetrated. This approach is limited by patient cooperation, body habitus, and type of stab wound. A clearly negative LWE can rule out significant abdominal injury and, in the right clinical setting, patients can be safely discharged without further workup. A positive LWE does not necessarily indicate the need for emergent laparotomy if the patient is not displaying any of the above indications for laparotomy, and these patients can be moved to either SCE or DI pathways depending on the practice setting and resources available (2).
SCEs have been used successfully in many settings, including multiple studies performed in South Africa, where the large majority of abdominal trauma is penetrating (3,12,13). SCEs are effective when examinations are performed at frequent intervals (4-6hrs), vitals are recorded at the same intervals, and are best when performed by the same practitioner(s) so that small changes in the clinical picture can be appreciated (2,3). This approach has been shown to be reliable at not only reducing the number of negative laparotomies performed and decreasing overall healthcare costs, but also has a high sensitivity in determining patients that require delayed laparotomy. It was also noted that the delay in time to laparotomy did not significantly affect the clinical outcomes or hospital length of stay in the South African studies (3,12,13).
Approach to the Patient with Thoracic Stab Wounds
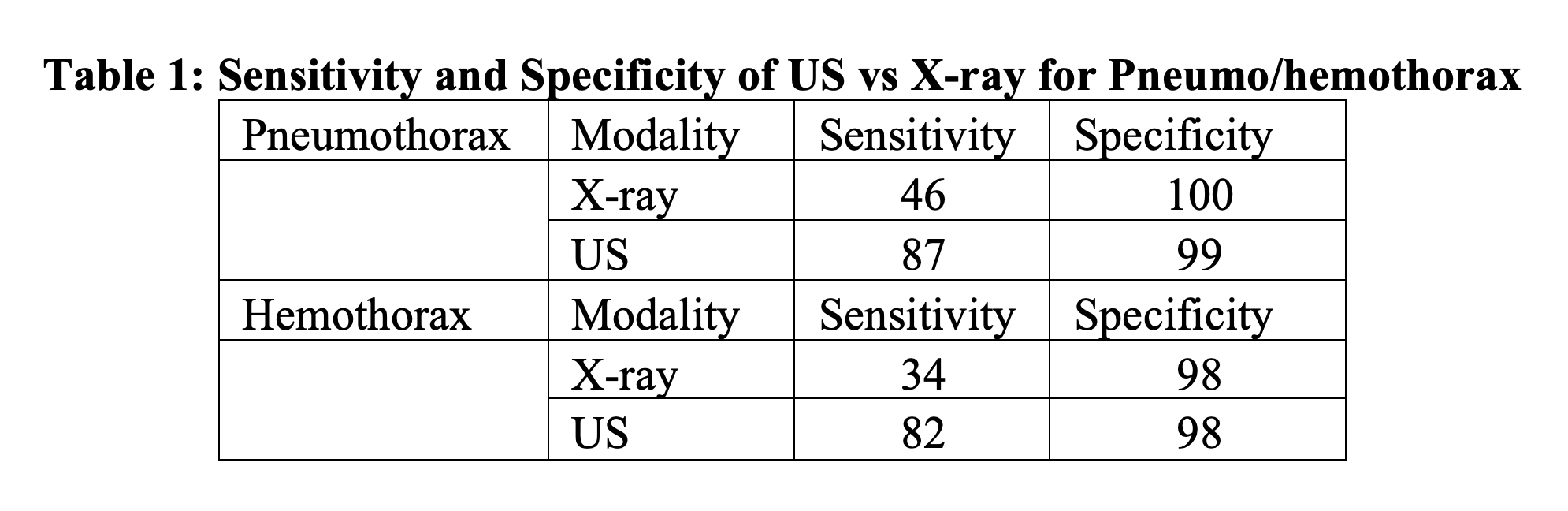
Patients with thoracic stab wounds should have an evaluation consistent with ATLS protocol and should include an eFAST. Overall it appears that US is a better modality than x-ray in diagnosis of hemo and pneumothorax with plain films likely missing smaller, less clinically significant injuries. US has been found to be both highly sensitive and specific for pneumothorax and hemothorax while chest x-ray is specific but has poor sensitivity (14,15,16). Pooled data is shown below in Table 1 (15,16).
Pneumothorax
Definitive treatment is with tube thoracostomy, but if tension physiology is present, then needle or finger thoracostomy should be performed prior to definitive chest tube placement. When either procedure is performed, the usual tube thoracostomy location (mid axillary line at the 5th intercostal space) is utilized. This location is better than the traditional midclavicular line at the 2nd intercostal space as there is a higher chance of success, likely secondary to the chest wall being thinner (17,18).
Hemothorax
Tube thoracostomy is the initial treatment. If there is >1500mL initial drainage or >200mL/hr in an adult (3mL/kg/hr) then a thoracotomy is indicated. Historic teaching has maintained that a larger chest tube is needed for proper drainage of a hemothorax. However, a recent 2012 study found the size of a chest tube (36-40Fr vs 28-32Fr) made no statistical difference in the number of complications (pneumonia, empyema, retained hemothorax) (19).
In addition to chest tube placement, there are other considerations. For instance, massive intrathoracic hemorrhage, does the patient need transfusion? Does the patient need antibiotics and/or tetanus prophylaxis? Prophylactic antibiotic use in hemopneumothorax after closed tube thoracostomy placement is controversial. EAST trauma guidelines still do not recommend routine use of prophylactic antibiotics after chest tube placement as there is insufficient data at this time (20). Tetanus toxoid vaccination should be provided in the setting of a thoracic stab wound if the patient has not had an update in the last 5 years per the CDC guidelines.
Pericardial Effusion/Tamponade
This is another injury that will be picked up by eFAST, but should be suspected particularly in trauma arrest with penetrating injuries. Studies on this topic are generally looking at diagnosis of hemopericardium and not tamponade. In the clinical setting, finding hemopericardium in a pulseless trauma victim leads us down particular management pathways. As such, eFAST is also highly sensitive (100%) and specific (96-99%) in the diagnosis of hemopericardium in penetrating cardiac injury (9, 10). Definitive treatment for pericardial effusion due to blood is surgical treatment with a pericardial window. A temporizing procedure would consist of a pericardiocentesis. In a traumatic arrest situation, an Emergency Department Thoracotomy would be another treatment modality to utilize. Nonprocedural measures with this injury include fluid resuscitation before definitive treatment to increase preload.
Diaphragmatic Injury
Diaphragmatic injuries can range from insidious to easily apparent on initial presentation. They are generally very uncommon representing less than 1% of all traumatic patients and are usually found in conjunction with other thoracic or abdominal trauma, namely on the left side due to protection the liver provides. If diaphragm injuries (namely lacerations) are missed, there is increased risk of herniation of abdominal contents into the thoracic cavity, which can cause obstruction and/or strangulation. Stab and penetrating wounds make up 65% of diaphragmatic injuries (21).
Evaluation of diaphragmatic injuries in the ED should start with a plain film of the chest to evaluate for thoracic injuries and abdominal contents within the thoracic cavity. However, current generation CT scanners are the imaging modality of choice. Interestingly, older CT scanners have not changed the insidiousness of this diagnosis (22).

The decision to further evaluate for this injury is largely let up to the attending surgeon when diagnostic imaging is negative or inconclusive. The next step in evaluation would be single port laparoscopic surgery for direct visualization. Treatment is operative repair, generally completed laparoscopically.
Emergency Department Thoracotomy
EAST guidelines strongly recommend Emergency Department Thoracotomy (EDT) due to an increase in survival rate, 2.8% without and 15.8% with, specifically for penetrating thoracic stab wounds with signs of life (23). Of those without signs of life, survival rates are still improved for patients, 8.3% survival when compared to 0.2% without, but depends on factors such as down time and CPR time. However, when arrest time is greater than 15 minutes, EDT efforts are considered futile (23).
Signs of life are defined as pupillary response, spontaneous ventilation, measurable blood pressure, pulses, extremity movement or cardiac electrical activity. Patients with tamponade on FAST or those with the above without pulses, EDT would also be recommended. However, practice setting is also a very important factor when determining to initiate the procedure. Clinicians without immediate surgical backup should not likely complete an EDT as there is no definitive therapy/intervention after the procedure. Roberts and Hedges outline the following factors when deciding to initiate an EDT: mechanism of injury, location of injury, initial cardiac rhythm, resuscitation time, signs of life.
Very broadly, an EDT is completed by creating an anterolateral incision at the 4th/5th intercostal space starting at the sternum and extending to past the posterior axillary line followed by dissection down to and through the parietal pleura. The size of the incision is important to allow tools such as a rib spreader and physician hands into the chest cavity. Once in the chest cavity, an incision with scissors should be made in the caudal-to-cephalad direction on the pericardium to open the pericardial sac (pericardiotomy) taking care to not injury the phrenic nerve so that direct cardiac repair can be initiated. Afterward, aortic cross clamping can be accomplished if the injury is below the diaphragm and/or the hilum of the lung can be twisted in the event the injury is on the lung parenchyma is injured (24).
Summary
Like all trauma, evaluation of thoracic and abdominal stab wounds should be completed in a systematic fashion following standard ATLS trauma algorithm. Recent literature has changed the manner in which abdominal stab wounds are managed. What was once a mandated trip to the operating room and hospital admission, may now consist only of a local wound exploration discharged home to follow up. Stab wounds to the thorax are managed much as they have in the past 20 years with little change except maybe to the size of the chest tube. A high index of suspicion must still be had by the Emergency provider for injuries frequently missed by imaging modalities.
Case Conclusion
Case 1: Patient was found to have a hemopneumothorax. A chest tube was inserted with 300cc of blood and improvement of vital signs.
Case 2: With a negative FAST exam, local wound exploration was completed that showed no violation of the abdominal wall. She was observed in the department for a secondary examination and subsequently discharged home.
Case 3: Patient was found to have a pneumothorax that was treated with a chest tube. CT imaging of the chest, abdomen and pelvis were completed that showed free air in the diaphragm. He was taken emergently to the operative suite for small bowel repair and found to have a diaphragm injury that was repaired as well.
Pearls and Pitfalls
- Recognize that wounds within the thoracoabdominal cavity need to be evaluated for both chest and abdominal wounds due to diaphragm movement
- Patients who are stable with a negative FAST may be candidates for local wound exploration and discharged home if the abdominal fascia is not violated. Those with violation of the fascia will require CT imaging.
- Complete a secondary examination of every patient with a stab wound to evaluate for multiple penetrating sites.
- For needle thoracostomy, consider entry at the mid-axillary line at the 5th intercostal space as the chest wall is thinner.
References:
- https://www.britannica.com/science/abdominal-cavity
- Martin MJ, Brown CV, Shatz DV, et al. Evaluation and management of abdominal stab wounds. Journal of Trauma and Acute Care Surgery. 2018;85(5):1007-1015. doi:10.1097/ta.0000000000001930.
- Pradeep HN, Jens UB, Sorin EDU, et al. Non-operative management of abdominal stab wounds – an analysis of 186 patients. South African Journal of Surgery. 2007;45(4):128-132.
- Salen PN, Melanson SW, Heller MB. The Focused Abdominal Sonography for Trauma (FAST) Examination: Considerations and Recommendations for Training Physicians in the Use of a New Clinical Tool. Academic Emergency Medicine. 2000;7(2):162-168. doi:10.1111/j.1553-2712.2000.tb00521.x.
- Dammers D, Moumni ME, Hoogland I, Veeger N, Avest ET. Should we perform a FAST exam in haemodynamically stable patients presenting after blunt abdominal injury: a retrospective cohort study. Scandinavian Journal of Trauma, Resuscitation and Emergency Medicine. 2017;25(1). doi:10.1186/s13049-016-0342-0.
- Blackbourne LH, Soffer D, Mckenney M, et al. Secondary Ultrasound Examination Increases the Sensitivity of the FAST Exam in Blunt Trauma. The Journal of Trauma: Injury, Infection, and Critical Care. 2004;57(5):934-938. doi:10.1097/01.ta.0000149494.40478.e4.
- Quinn AC, Sinert R. What is the utility of the Focused Assessment with Sonography in Trauma (FAST) exam in penetrating torso trauma? Injury. 2011 May; 42(5): 482-7.
- Jeroukhimov I, Wiser I, Hershkovitz Y, et al. Frequency of intra-abdominal organ injury is higher in patients with concomitant stab wounds to other anatomical areas. BMC Emerg Med. 2018; 18(1): 18. Published 2018 Jun 27.
- Patel AN, Brennig C, Cotner J, Lovitt MA, Foreman ML, Wood RE, et al. Successful diagnosis of penetrating cardiac injury using surgeon-performed sonography. Ann Thorac Surg. 2003;76:2043–6.
- Rozycki GS, Feliciano DV, Ochsner MG, Knudson MM, Hoyt DB, Davis F, et al. The role of ultrasound in patients with possible penetrating cardiac wounds: A prospective multicenter study. J Trauma. 1999 Apr;46(4):543-5
- Pfeifer, R et al. Missed injuries in trauma, a literature review. Patient Saf Surgery. 2008. 2:20
- Mnguni M, Muckart D, Madiba T. Abdominal Trauma in Durban, South Africa: Factors Influencing Outcome. International Surgery. 2012;97(2):161-168. doi:10.9738/cc84.1.
- Dayananda K, Kong V, Bruce J, Oosthuizen G, Laing G, Clarke D. Selective non-operative management of abdominal stab wounds is a safe and cost effective strategy: A South African experience. The Annals of The Royal College of Surgeons of England. 2017;99(6):490-496. doi:10.1308/rcsann.2017.0075.
- Ebrahimi A, Yousefifard M, Mohammad Kazemi H, et al. Diagnostic Accuracy of Chest Ultrasonography versus Chest Radiography for Identification of Pneumothorax: A Systematic Reviw and Meta-Analysis. Tanaffos. 2014;13(4):29–40.
- Ojaghi Haghighi SH, Adimi I, Shams Vahdati S, Sarkhoshi Khiavi R. Ultrasonographic diagnosis of suspected hemopneumothorax in trauma patients. Trauma Mon. 2014; 19(4).
- Inaba K, Branco BC, Eckstein M, et al. Optimal positioning for emergent needle thoracostomy: A cadaver-based study. J Trauma. 2011; 71(5): 1099-1103.
- Laan DV, Vu TD, Thiels CA, et al. Chest wall thickness and decompression failure: A systematic review and meta-analysis comparing anatomic locations in needle thoracostomy. Injury. 2016; 47(4): 797–804.
- Moore FO, et. al. Presumptive Antibiotics in Tube Thoracostomy. J Trauma. 73(5):S341-S344, November 2012.
- Inaba, et al. Does size matter? A prospective analysis of 28-32 versus 36-40 French chest tube size in trauma. J Trauma Acute Care Surg. 2012 Feb;72(2):422-7.
- Moore FO, et. al. Presumptive Antibiotics in Tube Thoracostomy. J Trauma. 73(5):S341-S344, November 2012.
- National Trauma Data Base. American College of Surgeons 2000-2004. https://ntdbdatacenter.com/
- Uhlich et al. Diagnosis of diaphragm injuries using modern 256-slice CT scanners: too early to abandon operative exploration. Trauma Surg Acute Care Open. 2018; 3(1): e000251.
- Seamon MJ, Haut ER, et al. Emergency Department Thoracotomy. The Journal of Trauma and Acute Care Surgery. July 2015. 79(1):159-173.
- Jones, R.F. & Rivers, E.P. (2014). Resuscitative Thoracotomy. In J. R. Roberts, C. B. Custalow, T. W. Thomsen, & J. R. Hedges (Eds.), Roberts and Hedges’ Clinical Procedures in Emergency Medicine (6th ed.). Philadelphia: Elsevier/Saunders.




