Adult Intussusception: Not like Trix, Not Just for Kids
By Scott McClure MD
EM Resident Physician, UTSW / Parkland Memorial Hospital
Edited by Alex Koyfman, MD (@EMHighAK) and Stephen Alerhand, MD (@SAlerhand)
Your next case:
A 57 year-old male with hx of HTN and DM2 presents with a month-long hx of abdominal pain. He describes a severe cramping pain that comes and goes in waves, occasionally associated with nausea and vomiting. He has seen his PCP for this pain and states that the lab work and other investigations have been negative, though he in unsure if a CT scan has been performed. The patient is frustrated that no diagnosis has been found for his pain. He denies hx of abdominal surgery, and denies melena/hematochezia/hematemesis. The most recent episode of pain has been constant for 12 hours, and the last bowel movement the day prior was unremarkable. He is passing flatus.
VS T 37, P 98, BP 155/90, 98%, RR 16
Exam: Non-toxic appearing with unremarkable general exam with normal bowel sounds, very mild periumbilical tenderness without rebound or guarding.
Differential?
You name it and it is probably in the differential. All the way from ACS to gastritis to obstruction to supratentorial and everything in between. That is one of the most frustrating things about abdominal pain is that almost anything can cause abdominal pain whether it is primary, referred, or imagined. The key question we all ask ourselves on patients like this is how in depth do we want our work up to be. What are we worried about? What can we not miss? In this case, a non-toxic middle-aged male presents with multiple weeks of abdominal pain and an unknown but self reported negative workup. The key question is: should this man get imaging? If surveyed, many physicians would be in favor of scan, while many could make another argument that he does not need it.
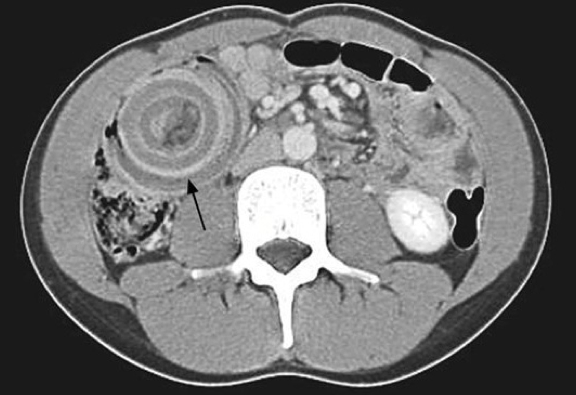
For the sake of the rest of this post, we will say the decision was made to proceed with CT scan, which showed an enteric intussusception with nonspecific small bowel mass being the lead point. We nailed the diagnosis! I can hear someone saying, “I knew it was intussusception all along!” After patting ourselves on the back, the question then becomes, now what? GI consult? Surgery? Rub some dirt on it?
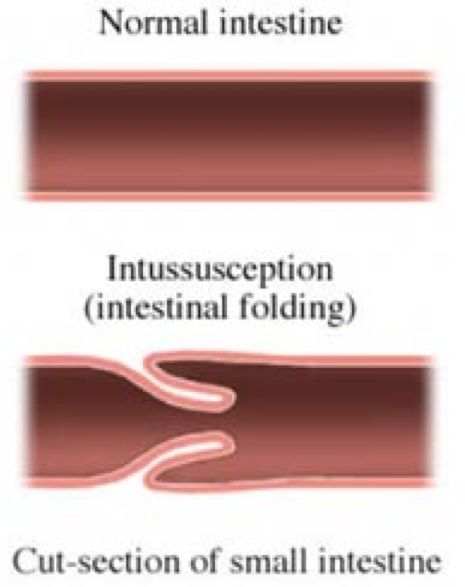
What is Intussusception?
It occurs is when part of the bowel (small or large) slides into an adjacent portion of bowel similar to how a telescope collapses for storage—hence the term “telescoping.” This can cause bowel obstruction proximal to the site, as well as ischemia since the blood supply to the affected bowel is cut off. Divided into 4 categories, enteric (only small bowel), colic (only large bowel), ileocolic (where the intussusception goes through the ileocecal valve, and ileocecal (where the ileocecal valve is the lead point of the intussusception).
 http://www.lifescript.com/health/centers/digestive/related_conditions/intussusception.aspx
http://www.lifescript.com/health/centers/digestive/related_conditions/intussusception.aspx
I thought Intussusception was only in children.
It is true that approximately 95% of cases of intussusception occur in children, but 1-5% occur in adults. It is the cause of 1-5% of all cases of intestinal obstruction in adults.
Differences in children vs. adults
Unlike in children where 90% of intussusceptions are thought to be idiopathic, in adults the cause (lead point) is identified in 70-90% of cases. Most commonly the cause of these lead points is tumor (malignant more common than benign), adhesions, or inflammation (IBD). G, GJ, and J tubes have been seen to cause intussusception as well. In adults, the most common site will be an enteric intussusception, though any of the four are possible. The classic triad of abdominal pain, vomiting, and rectal bleeding is much less likely to occur in adults (although to be fair I have never seen it in children either). The most common symptom in adults is abdominal pain (70-80%), while other symptoms may include vomiting, diarrhea, or rectal bleeding/melena. Up to 20% of adults with intussusception may be asymptomatic.
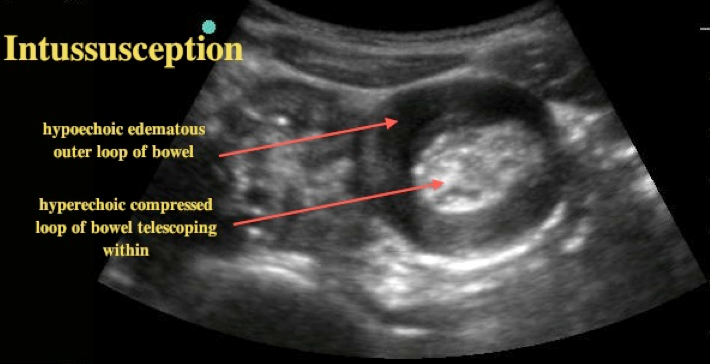
How do I make the diagnosis?
High clinical suspicion is required, as diagnosis can be easily missed in adults given non-specific symptoms. Acute abdominal series may show obstruction, or may be unremarkable. Ultrasound can be used to find intussusception similar to in children, though one must have the suspicion of intussusception to look for it. In truth, the diagnosis of intussusception is probably very low on our differential in the adult with undifferentiated abdominal pain. The gold standard is CT scan, with its very high specificity and sensitivity for diagnosing the disease. It is likely to show the cause or lead point, which is of great importance to our surgical colleagues.
 http://www.em.emory.edu/ultrasound/ImageWeek/Abdominal/toddler_abdominal_pain.html
http://www.em.emory.edu/ultrasound/ImageWeek/Abdominal/toddler_abdominal_pain.html
 http://www.anatomybox.com/intussusception/
http://www.anatomybox.com/intussusception/
Treatment
In contrast to children, surgical intervention is most commonly required as almost all cases are caused by a lead point (commonly malignancy), and thus likely to recur. Some cases can be managed non-operatively, but this decision needs to be made following CT scan with our surgical colleagues. The rest of care is symptomatic i.e. pain control, antiemetics, IV hydration. Similar to bowel obstruction, when the diagnosis is suspected all patients should be made NPO in anticipation of surgical intervention.
So I will nail this diagnosis every time right?
Maybe if you are Yoda. We are more likely to make this diagnosis while looking for something else such as bowel obstruction, diverticulitis, mesenteric ischemia, etc. The key point is to remember that in contrast to children, the management is usually surgical and all adult patients with intussusception should have a surgical consultation.
Sources/Further Reading
– Lindor, RA, et al. Adult intussusception: presentation, management, and outcomes of 148 patients. J Emerg Med. 2012 Jul;43(1):1-6. doi: 10.1016/j.jemermed.2011.05.098. Epub 2012 Jan 12.
– Soni S, Moss P, Jaiganesh T. Idiopathic adult intussusception. Int J Emerg Med. 2011 Mar 16;4:8. doi: 10.1186/1865-1380-4-8.
– Onkendi EO, Grotz TE, Murray JA, Donohue HD. Adult intussusception in the last 25 years of modern imaging: is surgery still indicated? J Gastrointest Surg. 2011 Oct;15(10):1699-705. doi: 10.1007/s11605-011-1609-4. Epub 2011 Jul 6.
– Yalmarthi S, Smith RC. Adult intussusception: case reports and review of literature. Postgrad Med J. 2005 Mar;81(953):174-7.
– Athanasios M, et al. Intussusception of the bowel in adults: A review. World J Gastroenterol. 2009 Jan 28; 15(4): 407–411.
– Waseem M, Rosenberg HK. Intussusception. Pediatr Emerg Care 2008;24:793–800.
– Karamercan A, Kurukahvecioglu O, Yilmaz TU, Aygencel G, Aytac ̧ B, Sare M. Adult ileal intussusception: an unusual emergency condition. Adv Ther 2006;23:163–8.
– Demirkan A, Yagmurlu A, Kepenekci I, Sulaimanov M, Gecim E, Dindar H. Intussusception in adult and pediatric patients: two different entities. Surg Today 2009;39:861–5.
– http://pubmed.org/pubmed/23331649
– http://pubmed.org/pubmed/24792936





1 thought on “Adult Intussusception: Not Like Trix, Not Just for Kids”
Pingback: emDOCs.net – Emergency Medicine EducationEM@3AM: Intussusception - emDOCs.net - Emergency Medicine Education