
EM@3AM – Acute Chest Syndrome
Welcome to EM@3AM: Let’s review a cause of significant morbidity and mortality in sickle cell patients.
EM@3AM – Acute Chest Syndrome Read More »
Welcome to EM@3AM: Let’s review a cause of significant morbidity and mortality in sickle cell patients.
EM@3AM – Acute Chest Syndrome Read More »
Welcome to EM@3AM, an emDOCs series designed to foster your working knowledge by providing an expedited review of clinical basics. We’ll keep it short, while you keep that EM brain sharp.
EM@3AM – Acute APAP Toxicity Read More »

In need of a quick refresher on the management of penetrating injuries? Read on as we provide helpful tips while reviewing the basics.
Penetrating Wounds in the Emergency Department: Considerations for Management Read More »

Do you tweet during conference or lecture? This post evaluates the pros and cons of live-tweeting.
#EMConf: Live Tweeting? Read More »

Having difficulty determining whether or not your GI bleeder is stable for the floor? Read on as we discuss risk stratification tools and risk factors for severe GI bleeds.
GI Bleeds: Who Needs ICU Level Care? Read More »
Managing Sexual Assault in the Emergency Department
This review will address patient stabilization, provide recommendations for obtaining a medical and assault history, and detail pregnancy and sexually transmitted infection prophylaxis. An in-depth discussion of the forensic examination will be omitted, as requirements regarding healthcare provider training, tools contained within forensic collection kits, time allotted between alleged assault and court admissible evidence collection, and chain of custody legislation vary according to individual state law.
Managing Sexual Assault in the Emergency Department Read More »

Third trimester pregnant patients are not seen commonly in the emergency department, but when they are, they have the potential for severe complications such as hemorrhagic shock. This article reviews the most serious causes of bleeding in the third trimester of pregnancy and also discusses management options.
The Bleeding Pregnant Patient in the Third Trimester: Pearls and Pitfalls Read More »
Patients who undergo elective abortions may present to the emergency department for various symptoms and complications due to their recent procedures. This is a brief article of the complications of elective abortion. Workup and management of these complications are also reviewed.
Recent Elective Abortion Read More »

Intubation, especially in the septic and critically ill patient, can, by itself, cause hemodynamic abnormalities and/or hypoxemia and hypercapnea. In some situations, it may be important to make sure that the patient is adequately prepared for intubation, both from hemodynamic and pre-oxygenation standpoints. This is a brief review of some suggestions when intubating the very ill patient in the emergency department.
Unstable Sepsis: Airway First? Not Always Read More »
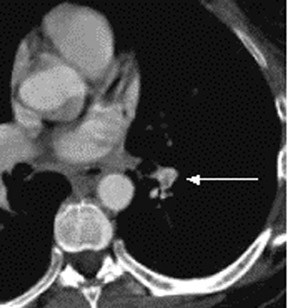
Pulmonary embolism (PE) is classically a life-threatening diagnosis, often considered in the work-up of patients with chest pain or dyspnea. Initial mortality rates of missed, untreated PE has been quoted as high as 26%, based on a 1960 study. This disease is common, with 400,000 patients affected with nonfatal PE and another 200,000 patients in the U.S. dying each year from this disease. PE is the third most common cause of death in cardiovascular disease after myocardial infarction and stroke.