
Author: Jennifer Robertson, MD, MSEd // Edited by: Alex Koyfman, MD (@EMHighAK, EM Attending Physician, UTSW / Parkland Memorial Hospital)
Case
A 50 year-old male presents to the emergency department (ED) with a five day history of worsening abdominal pain. He states this has never occurred before, but he thinks he has a known ventral hernia. He really has no other complaints other than the pain. Upon arrival, he appears diaphoretic and a little confused but is otherwise answering questions appropriately. The patient’s brother states that his brother is “always” sweaty and that the diaphoresis is nothing unusual. The patient denies any significant past medical history, including no history of diabetes, immunosuppression or chronic steroid use.
Initial vital signs (VS):
Heart rate (HR) 100 beats per minute (bpm), normal temperature, normal blood pressure, an oxygen saturation (SpO2) of 99% on room air (RA) and a respiratory rate of 24 breaths per minute.
Initial examination:
The patient is an obese male who appears ill and diaphoretic. He is somewhat tachypneic but is able to answer questions in full sentences. He has clear breath sounds and remains slightly tachycardic. His abdominal exam appears grossly abnormal, including marked distention and firmness. There is focal enlargement of his abdomen in the right lower quadrant and he has overlying erythema and warmth of this site. His genitourinary exam is normal.
Initial interventions:
An initial concern was for an incarcerated hernia, possibly bowel necrosis. Two large bore peripheral intravenous (IV) lines were placed and an initial crystalloid bolus was administered. Broad spectrum antibiotics were given immediately due to concern for early sepsis. Labs were ordered and pending. An electrocardiogram (ECG) was obtained showing sinus tachycardia without any acute abnormalities. The patient was deemed hemodynamically stable enough to go to computed tomography (CT) scan for imaging.
Sepsis: General Review
Extensive research, peer reviewed articles and online sites have studied, reviewed and evaluated sepsis and its dangers. The current article is not intended to cover sepsis or its definitions, however the following excellent articles can be reviewed on emdocs.net for an extensive review:
http://www.emdocs.net/fluid-choice-does-it-matter/
http://www.emdocs.net/utility-obtaining-lactate-measurement-ed/
http://www.emdocs.net/early-sepsis-why-do-we-miss-it-and-how-do-we-improve/
http://epmonthly.com/article/sepsis-mimics/
http://www.emdocs.net/the-dangers-of-over-resuscitation-in-sepsis/
http://www.emdocs.net/septic-shock-who-should-be-treated-with-early-pressors/
In general, sepsis can be a continuum from a very mild infection to fulminant septic shock. As a medical student and resident, one may have been taught that the airway always takes priority in any unstable patient, especially in altered patients who cannot protect their airways and those with primary airway or pulmonary diseases. However, immediately intubating a patient with sepsis may not be the right thing to do, especially if he or she is hemodynamically unstable. It should be mentioned that with the exception of the need for pre-oxygenation (see #2 below), this review is not about the patient who requires immediate intubation. Importantly, one should never wait until a patient’s physiologic reserve is completely gone and thus, if any planned resuscitation fails, then intubation should not be delayed (1).
Case Continuation
The patient returns from the CT scanner and the read is pending. The nurse taking care of the patient notifies you that the cardiac monitor demonstrates an irregularly irregular rhythm at 180 beats per minute.
Repeat examination:
HR 180 (irregular)
Blood pressure 90/50 mmHg
RR 40 breaths per minute
Patient more confused, remains diaphoretic
Repeat ECG: atrial fibrillation with rapid ventricular response (RVR), rate 180
The nurse asks what to do next…
Issues to Consider Prior to Intubation
There are two main issues to consider prior to intubating an unstable patient who requires an urgent but not immediate airway. These issues include (1) hemodynamic instability such as severe tachycardia, bradycardia and hypotension and (2) hypoxia that does not respond to standard oxygen therapy.
(1) Hemodynamic instability
Studies have shown that tracheal intubation is not a benign event. The simple act of intubating can cause hemodynamic changes that can affect post-intubation outcomes (2). In addition, the process of intubation typically requires induction agents and positive pressure ventilation, which can also significantly contribute to the hemodynamic changes seen during and after intubation (2, 3, 4, 5). In addition, repeat laryngoscopy attempts also can be detrimental (6). Not only can hemodynamic instability occur with intubation in normal, healthy patients, but it most definitely occurs in the critically ill emergency department (ED) patient and usually to a greater extent (2). The hemodynamic changes that result from laryngoscopy and tracheal intubation are complicated and multifactorial (8). However, research has demonstrated airway manipulation is a potent stimulator of the sympathetic and parasympathetic nervous systems, with initial increases in heart rate and blood pressure due to transient catecholamine release (3). Endogenous epinephrine has a very short half-life, however, and post-intubation hypotension (typically described as ≤ 90 mm Hg systolic) is thought to be due to rapid attenuation of this sympathetic tone (2). In addition, the addition of positive end expiratory pressure (PEEP) can further decrease cardiac preload by decreasing venous return (2). This is especially a problem in those patients who have diminished cardiac reserve, are hypovolemic, or septic (2). Extreme bradycardia and hypotension can also occur due to repetitive laryngoscopy and can also be worsened in those patients who have concomitant hypoxemia (2, 6).
While the hemodynamic changes during intubation can be considered “normal” physiologically, it is not a benign process (8). In fact, post-intubation hypotension (and really any hypotension in the ED) is associated with increased morbidity, prolonged patient stays, cardiac arrest and death (8-14). In addition, other studies have demonstrated that lower blood pressures and elevated shock indices (such as seen in sepsis) prior to intubation are associated with post-intubation hypotension and poorer outcomes (8, 10, 15, 16). Thus, hemodynamic resuscitation prior to intubation should be considered in the unstable (but not crash airway) patient (1, 12).
Case Continued
Upon re-examination, the patient remains diaphoretic and altered. Laboratory tests started to return and demonstrated a leukocytosis and a lactate level of 4.0. Surprisingly, the serum bicarbonate level was only mildly decreased. The CT read was still pending. Clinically, the patient was septic and likely from an intra-abdominal pathology. The decision was made to intubate and start a central line, however, given the new onset atrial fibrillation with RVR and low blood pressures, it was decided to first attempt synchronized cardioversion to see if conversion to sinus rhythm would allow for increased cardiac output and blood pressure prior to intubation. Using a small dose of ketamine for comfort and pain relief, the patient was cardioverted twice without success. He was finishing his second liter of crystalloid, remained hypotensive and tachycardic, and the nurse started to look concerned…
Solutions
A few strategies to avoid hypotension and maximize cardiac preload and afterload prior, during and after intubating an urgent airway (1, 2, 17):
(a) Maximize fluid status
(b) Consider using push dose vasopressors such as phenylephrine or epinephrine. The dose of push dose phenylephrine is 50-200 micrograms (mcg) every two to five minutes. The dose of push dose epinephrine is 5-20 mcg every two to five minutes. A good review of dosing can be seen at http://emcrit.org/wp-content/uploads/push-dose-pressors.pdf (18).
(c) Cardiovert any unstable rhythms
(d) Consider using induction and sedative agents that work best for each patient’s hemodynamic status. This article is not intended to be a review of pharmacologic agents. A nice medication review can be seen at http://www.emdocs.net/8751-2/ (19).
(e) Avoid too much PEEP after intubating if possible
Case Resolution
After a failed cardioversion, the patient’s blood pressure continued to decline. Three doses of push dose phenylephrine were given while the patient was prepared for intubation. His blood pressure rose and his heart rate declined with the phenylephrine, but he did remain in atrial fibrillation. The patient was given an induction dose of ketamine and intubated on the first pass without any complications. The patient’s CT read finally returned, demonstrating a ruptured bowel with pneumoperitoneum. A central line was placed and the patient was transferred to a higher level of care and he was extubated by day ten of hospitalization.
(2) Hypoxia
While the patient did not sustain hypoxia and had a normal PO2 on his initial and subsequent arterial blood gas (ABG) measurements, many patients do. On occasion, patients with an urgent, but not crash, need for an airway may not be able to sustain oxygen saturations above 90% on high levels of supplemental oxygen. In this case, ED providers may be eager to intubate the patient to “increase oxygen levels”. However, it is not the intubation that helps this but likely the positive pressure that is provided after intubation and during the patient’s therapy on the ventilator (17).
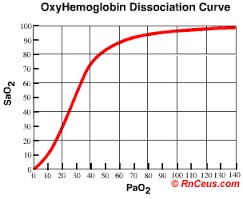
The goal of pre-oxygenation is to get the oxygen saturation as high as possible in order to allow for enough time for intubation and prevent severe hypoxemia during the procedure (17). If patients are intubated prior to adequate pre-oxygenation, they are at risk for a rapid decline in oxygen levels. This is even more pronounced in the obese and critically ill patients (20, 21). The oxygen-hemoglobin dissociation curve demonstrates this physiology.
Severe hypoxemia is a risk factor for cardiac arrest and thus, it is imperative that patients, even those whose oxygen saturations do not reach above 90% on supplemental oxygen, receive adequate pre-oxygenation prior to intubation (7, 17, 22). Patients with poor alveolar oxygenation whose oxygen saturations do not rise with simple supplemental oxygen may be undergoing a number of possible pathologies such as dead space where there is normal ventilation but no perfusion, a shunt, and a low venous oxygen saturation (17). Examples include a septal cardiac defect (anatomic shunt), pneumonia or pulmonary edema (physiologic shunt), a pulmonary embolism (dead space), and shock states (poor venous oxygen saturation) (17).
In order to properly pre-oxygenate the above types of patients, it may be necessary to incorporate other techniques prior to intubation. It is imperative that emergency physicians understand this need to take the time to properly pre-oxygenate and not to “jump to intubation” when a patient does not respond to simple supplemental oxygen therapy and a standard bag valve mask. Techniques to consider include: (1) Non-invasive positive pressure ventilation (NIPPV) and the use of PEEP valves, (2) Apneic oxygenation and (3) Delayed sequence intubation (17, 21, 22).
(1) NIPPV – In a patient whose oxygen saturation does not improve with standard pre-oxygenation techniques, such as a patient with shunting, may require positive pressure ventilation. In this case, positive pressure ventilation has been shown to improve the efficiency of gas exchange, recruit more alveoli, increase lung volumes and increase the amount of time it takes for desaturation to occur (17, 21). In order to achieve this, a standard continuous positive airway pressure (CPAP) machine can be utilized, maintaining a PEEP of 5 to 15 cm H20 (17). Another strategy is to use the ventilator for this and the 2010 article by Dr. Weingart can be reviewed for the proper ventilator settings for pre-oxygenation (17). If a patient cannot tolerate the positive pressure mask, then a technique called delayed sequence intubation can be used as mentioned below (17, 23).
Another noteworthy topic is the use of the BVM. Standard BVMs do not provide any PEEP. Therefore, if there is a shunt and the patient’s oxygenation is not improving with the BVM, a tool called a PEEP valve can also be used (17). It is imperative that the mask seal is tight, otherwise the PEEP valve will not be useful (17).
(2) Apneic Oxygenation – The very act of rapid sequence intubation does entail a period of apnea while the tube is being placed. It is thought that placing supplemental oxygen via nasal cannula may be helpful to supply additional oxygen while the patient is apneic. It has been demonstrated that alveoli continue to take up some oxygen, even without active breathing (22). While carbon dioxide does increase during this time, the patient still may be oxygenated during the apneic period with the idea of “apneic oxygenation” (17, 22). Of note, once the patient is paralyzed, it is important to make sure that the tongue and posterior pharynx is not occluding the airway and a head tilt with chin lift is adequate for most patients. A nasal or oral airway may be required as well (22).
(3) Delayed sequence intubation – For the difficult patient who requires pre-oxygenation, a simple facemask may not work, as it may be pulled off due to agitation or confusion. In addition, the added hypoxia and hypercapnia may add to any agitation, causing patients to become even more uncooperative (17). One proposed way to get around this agitation is with a concept called “delayed sequence intubation” (DSI). Several articles have been written by Dr. Weingart and his articles are listed below for review. However, in short, DSI consists of administering a sedative agent that does not cause spontaneous respirations to decline, such as ketamine at a dose of 1-1.5 mg/kg slow intravenous push (17). After giving the medication, the patient becomes calmer, allowing proper preoxygenation to occur (17, 23). After the patient is adequately preoxygenated, then standard rapid sequence intubation can occur. This procedure was recently researched by Dr. Weingart in 2015 with promising results (23). The same concepts of needing PPV may be required in those patients who demonstrate shunt physiology.
Conclusions: Tracheal intubation is more complicated than a simple airway tube, especially in the critically ill and septic patients. While some patients require an immediate airway, many patients should be critically assessed prior to intubation. Proper pre-oxygenation should always occur and hemodynamic resuscitation should be considered in order to avoid post-intubation hypotension and increased morbidity and mortality.
References / Further Reading
- Manthous CA. Avoiding circulatory complications during endotracheal intubation and initiation of positive pressure ventilation. J Emerg Med 2010; 38 (5): 622-31.
- Mort TC. Complications of emergency tracheal intubation: hemodynamic alterations-Part I. J Intensive Care Med 2007; 22 (3): 157-65.
- Shribman AJ, Smith JG, Achola KJ. Cardiovascular and catecholamine responses to laryngoscopy with and without tracheal intubation. Br J Anaesth 1987; 59 (3): 295-99.
- Bucx MJL, Van Geel RTM, Scheck PAE, et al. Cardiovascular effects of forces applied during laryngoscopy.Anaesthesia 1992; 47 (12): 1029-33.
- Schwab TM, Greaves TH. Cardiac arrest as a possible sequela of critical airway management and intubation. Am J Emerg Med 1998; 16 (6): 609-12.
- Mort TC. Emergency tracheal intubation: complications associated with repeated laryngoscopic attempts. Anesth Analg 2004; 99 (2): 607-13.
- Mort TC. The incidence and risk factors for cardiac arrest during emergency tracheal intubation: a justification for incorporating the ASA Guidelines in the remote location. J Clin Anesth 2005; 16 (7): 508-16.
- Heffner AC, Swords DS, Nussbaum ML, et al. Predictors of the complication of post-intubation hypotension during emergency airway management. J Crit Care 2012; 27 (6): 587-93.
- Heffner AC, Swords DS, Kline JA. The frequency and significant of post-intubation hypotension during emergency airway management. J Crit Care 2012; 27 (4): 417-e9.
- Schwartz DE, Matthay MA, Cohen NH. Death and other complications of emergency airway management in critically ill adults. A prospective investigation of 297 tracheal intubations. Anesthesiology 1995; 82 (2): 367-76.
- Heffner AC, Swords DS, Neale MN, et al. Incidence and factors associated with cardiac arrest complicating emergency airway management. Resuscitation 2013; 84 (11): 1500-04.
- Kim WY, Kwak MK, Ko BS, et al. Factors associated with the occurrence of cardiac arrest after emergency tracheal intubation in the emergency department. PLOS One 2014; 9 (11): e112779.
- Jones AE, Yiannibas V, Johnson C, et al. Emergency department hypotension predicts sudden unexpected in-hospital mortality: a prospective cohort study.”CHEST 2006; 130 (4): 941-46.
- Merz TM, Etter R, Mende L, et al. Risk assessment in the first fifteen minutes: a prospective cohort study of a simple physiological scoring system in the emergency department. Crit Care 2011; 15 (1): 1.
- Green RS, Edwards J, Sabri E, et al. Evaluation of the incidence, risk factors and impact on patient outcomes of post-intubation hemodynamic instability. CJEM 2012; 14 (2): 74-82.
- Lin CC, Chen KF, Shih CP, et al. The prognostic factors of hypotension after rapid sequence intubation. Am J Emerg Med 2008; 26 (8): 845-51.
- Weingart SD. Preoxygenation, reoxygenation, and delayed sequence intubation in the emergency department. J Emerg Med 2011; 40 (6): 661-67.
- http://emcrit.org/wp-content/uploads/push-dose-pressors.pdf.
- http://www.emdocs.net/8751-2/
- Dargin J, Medzon R. Emergency department management of the airway in obese adults. Ann Emerg Med 2010; 56 (2): 95-104.
- Baillard C, Fosse JP, Sebbane M, et al. Noninvasive ventilation improves preoxygenation before intubation of hypoxic patients. Am J Respir CritCareMed 2006; 174 (2): 171-77.
- Weingart SD, Levitan RM. Preoxygenation and prevention of desaturation during emergency airway management. Ann Emerg Med 2012; 59 (3): 165-75.
- Weingart SD, Trueger S, Wong N, et al. Delayed sequence intubation: a prospective observational study. Ann Emerg Med 2015; 65 (4): 349-55.





4 thoughts on “Unstable Sepsis: Airway First? Not Always”
Pingback: Global Intensive Care | LITFL Review 244
Pingback: Länkar v34 | Internmedicin